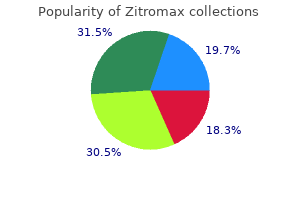
"Generic 250 mg zitromax, antibiotic resistance powerpoint."By: Dawn Sowards Brezina, MD - Assistant Professor of Medicine
 https://medicine.duke.edu/faculty/dawn-sowards-brezina-md
Buy generic zitromax 500mg onlineGipson I, Spurr-Michaud S, Tisdale A: Hemidesmosomes and anchoring fibril collagen seem synchronously during improvement and wound healing. Murakami J, Nishida T, Otori T: Coordinated appearance of beta 1 integrins and fibronectin during corneal wound therapeutic. Lambiase A, Manni L, Bonini S, et al: Nerve growth factor promotes corneal healing: structural, biochemical, and molecular analyses of rat and human corneas. Murakami J, Morimoto K, Nishida T, Otori T: Movement of corneal epithelium of rats in situ observed by time-lapse cinematography. Nishida T, Nakagawa S, Nishibayashi C, et al: Fibronectin enhancement of corneal epithelial wound therapeutic in rabbits in vivo. Hayashi K, Berman M, Smith D, et al: Pathogenesis of corneal epithelial defects: role of plasminogen activator. The significance of tear plasminogen activators within the inflammatory and traumatic lesions of the cornea and the conjunctiva. Vaheri A, Tapiovaara H, Myohanen H, Bitik J: Regulation of the pericellular activation of plasminogen and its function in tissuedestructive processes. Conn H, Berman M, Kenyon K, et al: Stromal vascularization prevents corneal ulceration. Berman M, Winthrop S, Ausprunk D, et al: Plasminogen activator (urokinase) trigger vascularization of the cornea. Berrman M, Leary R, Gage J: Evidence for a task of the plasminogen activator-plasmin system in cortical ulceration. Ohashi Y, Motokura M, Kinoshita Y, et al: Presence of epidermal progress think about human tear. Nishida T, Nakamura M, Murakami J, et al: Epidermal development issue stimulates corneal epithelial cell attachment to fibronectin by way of a fibronectin receptor system. Schultz G, Chegini N, Grant M, et al: Effects of progress factors on corneal wound therapeutic. Mishima H, Nakamura M, Murakami J, et at: Transforming progress factor-beta modulates results of epidermal progress factor on corneal epithelial cells. Ofuji K, Nakamura M, Nishida T: Signaling regulation for synergistic results of substance P and insulin-like progress factor-1 or epidermal development issue on corneal epithelial migration. Nakamura M, Nishida T, Ofujik K, et al: Synergistic effect of substance P with epidermal development factor on epithelial migration in rabbit cornea. Nakamura M, Chikama T, Nishida T: Up-regulation of integrin alpha 5 expression by combination of substance P and insulin-like development factor-1 in rabbit corneal epithelial cells. Mishima S: the effects of the denervation and the stimulation of the sympathetic and trigeminal nerve on the mitotic price of the corneal epithelium in the rabbit. Donnerer J, Amann R, Schuligoi R, Skofitsch G: Complete recovery by nerve progress factor of neuropeptide content material and performance in capsaicin-impaired sensory neurons. Crabb C: Endocrine influences on ulceration and regeneration in the alkaliburned cornea. Newsome D, Gross J: Prevention by medroxyprogesterone of perforation within the alkali-burned rabbit cornea: inhibition of collagenolytic activity. Tsubota K, Goto E, Shimmura S, Shimazaki J: Treatment of persistent corneal epithelial defect by autologous serum application. Nishida T, Ohashi Y, Awata T, Manabe R: Fibronectin � a new therapy for corneal trophic ulcer. Shimmura S, Igarashi R, Yaguchi H, et al: Lecithin-bound superoxide dismutase within the therapy of noninfectious corneal ulcers. Bonini S, Lambiase A, Rama P, et al: Topical treatment with nerve development issue for neurotrophic keratitis. Lambiase A, Rama P, Bonini S, et al: Topical remedy with nerve development factor for corneal neurotrophic ulcers. Khokhar S, Natung T, Sony P, et al: Amniotic membrane transplantation in refractory neurotrophic corneal ulcers: a randomized, managed scientific trial. Prabhasawat P, Kosrirukvongs P, Booranapong W, Vajaradul Y: Single and multilayer amniotic membrane transplantation for persistent corneal epithelial defect with and with out stromal thinning and perforation. Ivekovic B, Tedeschi-Reiner E, Petric I, et al: Amniotic membrane transplantation for ocular surface reconstruction in neurotrophic corneal ulcera. Sato H, Shimazaki J, Shinozaki K: Role of growth components for ocular floor reconstruction after amniotic membrane transplantation. Gundersen T: Conjunctival flaps within the therapy of corneal illness close to a model new technique of application. Dausch D, Landesz M, Klein R, Schroder E: Phototherapeutic keratectomy in recurrent corneal epithelial erosion. Ohman L, Fagerholm P: the affect of excimer laser ablation on recurrent corneal erosions: a potential randomized research. Kenyon Chemical accidents are probably devastating ocular surface injuries that can end result in everlasting visual impairment. These pathophysiologic processes have been discussed extensively elsewhere but are summarized briefly within the remainder of this part. Although partial transdifferentiation of conjunctival epithelium to corneal epithelium may be attainable,33�35 compelling proof means that conjunctiva-derived epithelium never absolutely expresses corneal epithelial phenotypic options. Limbal stem cells are the cells most qualified to restore practical competence of the corneal epithelial floor after injury. Corneal repair by keratocytes consists of both synthesis and degradation of stromal collagen. Persistent inflammation could delay reepithelialization and shift the web stability of corneal restore towards progressive stromal ulceration. Glass sharpening Glass frosting Mineral refining Gasoline alkylation Silicone manufacturing 1. Exploitation of identified pharmacologic intervention, which helps shift the stability towards restore, quite than ulceration, is the second main principle in the management of extreme chemical accidents. The healing pattern of the ocular surface epithelium can subsequently be used to make a more definitive dedication of the severity of limbal stem cell harm. Extensive limbal stem cell injury will in the end lead to either development of fibrovascular pannus or sterile corneal ulceration. In the absence of specific stains for limbal stem cells, a definitive diagnosis of the actual extent of limbal stem-cell loss could be made only after a number of weeks of observation of the epithelial therapeutic patterns. The extent of floor involvement could be decided by the size of the corneal and conjunctival epithelial defects. The depth of corneal and intraocular penetration may be estimated by evaluating corneal clarity, intraocular irritation, intraocular stress, and lens clarity. The depth of ocular surface penetration, and attainable limbal stem-cell harm, could be evaluated not directly by evaluation of vascular ischemia and necrosis of limbal and bulbar conjunctiva. The modified Hughes classification8,9,sixty three correlates the degree of limbal ischemia with prognosis. In recognition that the relation between the scientific appearance of limbal ischemia and prognosis is attributable to the precise damage of limbal stem cells, a extra recent classification scheme based on the degree of limbal stem-cell loss has been proposed). After a grade I harm with no limbal stem-cell loss, full reepithelialization with a normal corneal phenotype is complete inside 1 week.
Order zitromax 500 mg onlineIn contrast to acyclovir, which is only minimally phosphorylated by cellular (host cell) enzymes, ganciclovir appears to be extra susceptible to phosphorylation by enzymes in uninfected cells, especially in quickly dividing cells. This phosphorylation in uninfected cells can range from lower than 10% to being equal to that in virus-infected cells. Unfortunately, this additionally makes the drug extra poisonous to the bone marrow, inflicting a significant neutropenia in additional than 50% of patients treated. However, despite careful administration, ~40% of sufferers ultimately expertise reactivation of disease. Additional data supporting ganciclovir as virustatic come from histopathologic studies of enucleated globes from sufferers who died while receiving ganciclovir remedy. Because ganciclovir is poorly absorbed from the gastrointestinal tract, intravenous administration is preferred. It is unknown whether or not ganciclovir is distributed into human milk; nonetheless, no drug is current in the milk of lab animals. The major route of excretion is in urine, and it seems to be mainly through glomerular filtration. The intravenous route of ganciclovir therapy has been proven to be effective within the therapy of cytomegaloviral retinitis in immunocompromised sufferers. Usually, interruption of ganciclovir remedy or a decrease in dosage results in increased neutrophil counts. Thrombocytopenia (platelet rely < 50 000/mm3) can even result from a direct, dose-dependent impact of the drug. Ocular unwanted facet effects embody rhegmatogenous retinal detachment on account of ganciclovir-induced decision of retinitis. Local tolerance was superior with the gel formulation of ganciclovir with fewer complaints of discomfort (stinging, burning) or blurred imaginative and prescient after application. Oral ganciclovir and ganciclovir implants are efficient different routes of drug administration. The implant is placed surgically in the vitreous cavity, and might present therapeutic levels of up to 8 months relying on the speed of drug release. Because of the high pH of the ganciclovir infusion answer, irritation, phlebitis, and pain at the web site of intravenous infusion can occur. Foscarnet also wants to not be administered by fast or bolus intravenous injection as a result of the toxicity may be elevated by extreme drug ranges in the plasma. Side effects embody fever and gastrointestinal upset, including nausea, vomiting, diarrhea, anorexia, and belly ache. Intravitreal Antivirals Drug Ganciclovir (Cytovene) Foscarnet (Foscavir) Cidofovir (Vistide) Dosage 200�400 mg/0. Subsequent upkeep therapy is required with foscarnet, and the dosage range instructed is 90� one hundred twenty mg kg�1 day�1. This route is especially helpful for sufferers in whom ganciclovir is contraindicated on account of acyclovir allergy, and in whom intravenous foscarnet is contraindicated because of renal failure. In stem cell transplantation, preemptive remedy with foscarnet avoids the neutropenia and associated complications related to ganciclovir. In preclinical trials, it has been proven to be therapeutically efficient as a topical 0. It is a extremely efficient topical treatment of herpetic keratitis, of recurrent herpes labialis, and of the systemic (oral) therapy of herpes zoster. Compared with famciclovir, brivudin offers equal efficacy and security at a more convenient once-daily, dose schedule of a hundred twenty five mg qd. Pavan-Langston D, Lass J, Campbell R: Antiviral drops: comparative therapy of experimental herpes simplex keratouveitis. Hyndiuk R, Seideman S, Leibsohn J: Treatment of vaccinial keratitis with trifluorthymidine. Lin T, Chai C, Prusoff W: Synthesis and biological activities of 5-trifluoromethyl-5,azido-2,5, dideoxyuridine and 5trifluoromethyl-5,-amino-2,5,-dideoxyuridin. Coster D, McKinnon J, McGill J, et al: Clinical analysis of adenine arabinoside and trifluorothymidine in the therapy of corneal ulcers caused by herpes simplex virus. La Lau C, Oosterhuis J, Versteeg J, et al: Acyclovir and thrifluorothymidine in herpetic keratitis � a multicenter trial. Hyndiuk R, Raimundo E, Charlin T, et al: Trifluridine in resistant human herpetic keratitis. Shearer D, Bourne W: Severe ocular anterior phase ischemia after long-term trifluridine therapy for presumed herpetic keratitis. Lass J, Langston R, Foster C, et al: Antiviral medications and corneal wound therapeutic. Pepose J, Margolis T, Pavan-Langston D: Ocular vaccinia: problems and remedy, Am J Ophthalmol 2003; 136:343�347. National Institute of Allergy and Infectious Diseases collaborative antiviral research. Pavan-Langston D, Campbell R, Lass J: Acyclic antimetabolite therapy of experimental herpes simplex keratitis. DeMiranda P, Blum M: Pharmacokinetics of acyclovir after intravenous and oral administration. Schaeffer H, Beauchamp L, DeMiranda P, et al: 9-(2-Hydroxyethoxymethyl) guanine exercise towards viruses of the herpes group. Pavan-Langston D, Lass J, Hettinger M, Udell I: Acyclovir and vidarabine in the treatment of ulcerative herpes simplex keratitis. Young B, Patterson A, Ravenscroft T: Double-blind clinical trial of acyclovir and adenine arabinoside in herpetic corneal ulceration. Schwartz G, Holland G: Oral acyclovir for the administration of herpes simplex keratitis in kids. Barron B, Shimeld C, Claoue C, et al: the herpetic eye illness examine: a managed trial of acyclovir in steroidtreated herpes simplex stromal keratitis. Wilhelmus K, Gee L, Hauck W, et al: Herpetic eye illness study: a controlled trial of topical cortcosteroids for herpes simplex stromal keratitis. Wu X, Chen X: Acyclovir for the treatment and prevention of recurrent infectious herpes simplex keratitis. Tambasco F, Cohen E, Nguyen L, et al: Oral acyclovir after penetrating keratoplasty for herpes simplex keratitis. Erlich K, Mills J, Chatis P, et al: Acyclovirresistant herpes simplex virus infections in sufferers with the acquired immunodeficiency syndrome. Sonkin P, Baratz K, Frothingham R, Cobo L: Acyclovir-resistant herpes simplex virus keratouveitis after penetrating keratoplasty. Stranska R, Schuurman R, Nienhuis E, et al: Survey of acyclovir-resistant herpes simplex virus within the Netherlands: prevalence and characterization. Marsh R, Cooper M: Double masked trial of topical acyclovir and steroids within the remedy of herpes zoster ocular irritation. Cobo L, Foulks G, Liesegang T, et al: Oral acyclovir within the treatment of acute herpes zoster ophthalmicus.

Generic 250 mg zitromaxSuperior rectus and inferior rectus traction sutures may be used to assist within the posturing and stabilization of the attention. Scleral help with a Flieringa ring may be used for chosen patients which have a greater tendency for scleral collapse, similar to beforehand vitrectomized eyes, aphakic eyes, and pediatric sufferers. The appropriately sized ring is sutured onto the episclera ~3�4 mm from the limbus. The Flieringa ring must be removed as soon as enough sutures (either four or eight sutures) have been positioned to maintain the round form of the graft. The geometric axis is set by the intersection of the vertical and horizontal corneal meridians, while the optical axis represents the middle of the pupil, which is often slightly nasally displaced. Most surgeons favor to use the geometric center of the cornea for centration of the graft, though some surgeons prefer to place the graft center barely nasally to take into account the nasally displaced pupil. Surgical callipers could also be used to help in figuring out the geometric center of the cornea. In situations where the nature of the corneal pathology is marked eccentric, it could be essential to decenter the graft, such as in superior keratoconus with a hanging cone, peripheral problems similar to pellucid marginal degeneration, and peripheral ulcerative conditions. The applicable graft dimension is decided, based mostly on the dimensions of the corneal pathology and the dimensions of the cornea. In addition, much less endothelium is transplanted, which might be much less fascinating for patients with endothelial illness. The most typical diameters of trephines used to reduce the recipient cornea vary from 7. Alternatively, regional anesthesia within the type of a peribulbar or retrobulbar injection of a mix of lidocaine and a longer-acting anesthetic. The donor button could additionally be removed from an entire globe or extra generally, from a corneoscleral button. The corneoscleral button is placed endothelial facet up on a Teflon block and trephination is carried out with disposable trephines. Donor buttons trephined from the posterior corneal surface are slightly smaller in diameter than buttons trephined from the anterior floor. In sure conditions, corresponding to keratoconus, some surgeons prefer to use grafts of the same dimension as the recipient, to assist to scale back the diploma of postoperative myopia. The best trephination is one that produces a central, uniform reduce, with vertically aligned edges, whereas avoiding damage to the intraocular buildings. The numerous trephination methods could also be broadly divided into suction-assisted trephines or free-standing, handle-mounted trephines. Examples of suctionassisted trephines embrace the Baron Hessburg, Hanna, and Krumeich trephination methods. The donor cornea is commonly trephined on a Teflon block utilizing a hand-held Troutman Punch and Solan trephine, or suction-assisted trephines such as the Hanna system. Following donor cornea trephination, a generous amount of viscoelastic and fluid is then applied onto the donor to protect the endothelium, and the button is then passed to the scrub nurse to be carefully laid apart until needed. Modern anterior segment surgical procedure aims to reconstruct and proper as a lot of the anterior phase abnormalities as is safely possible. A viscoelastic agent is utilized into the anterior chamber as well as the edges of the recipient corneal bed simply prior to placement of the donor button, in order to defend the endothelium of the donor cornea in opposition to contact with different intraocular buildings throughout suturing. The use of viscoelastic brokers helps to reduce donor endothelial cell loss after keratoplasty. With a double-toothed Polack forceps, the superior fringe of the donor cornea is grasped and the needle of a 10-nylon suture is handed radially via the 2 tips of this forceps. The primary fixation of the graft is often by 4 interrupted 10�0 nylon sutures, placed within the 4 quadrants 90� aside. The anterior chamber is reformed with viscoelastic and suturing is continued, taking care to guarantee even and radial distribution of the sutures. The graft may be secured in place with either continuous sutures or interrupted sutures. The numerous strategies of suturing include inserting both 16 symmetrically positioned interrupted sutures, single or double operating steady sutures, or a mixture of 4 or eight interrupted sutures and a single steady suture. Interrupted sutures are used if uneven wound healing is anticipated, such as in scarred or necrotic areas of the recipient bed, or if there are sections of vascularization. An irregularly vascularized bed usually heals more rapidly in these areas where vessels are current and extra slowly within the avascular areas. This permits for selective suture elimination when suture loosening occurs or to correct postoperative astigmatism. Similarly, more sutures could also be required if the host bed is irregular in thickness, corresponding to when coping with corneal melting or marginal degeneration. Double running continuous sutures are used when the host bed is uniformly thick and avascular, and the wound is predicted to heal evenly, corresponding to in keratoconus or bullous keratopathy. Whatever the choice of suture method opted for, sutures should be handed deeply into the stroma at an equal depth for each donor and recipient to allow correct anterior�posterior donor�recipient apposition. Deep stromal bites are taken at ~80�90% depth, with care taken to not penetrate Descemets layer, which might contribute to wound leak at the finish of the operation. The surgeon ensures that the trephine is held perpendicular to the cornea and centered over it using the beforehand marked center as a information. The peripheral corneal ring between the blade and the limbus must be even to guarantee optimum centration. In order to stabilize the globe, the assistant exerts delicate traction on the recti sutures and barely uplifts the globe, while the surgeon could further grasp the limbus with a toothed forceps for added stability. The deal with with attached trephine is then gently rotated, with a gentle downward compressive force. The cornea is minimize by making easy back-and-forth rotations of the trephine round its axis whereas making use of agency even pressure. Excessive downward pressure might result in corneal distortion, leading to an undercut, sloping trephination edge. The anterior chamber is entered in a controlled method, utilizing a sharp blade held at an angle. Viscoelastic is then launched to reform the anterior chamber and to discourage prolapse of the iris, lens, and vitreous, because the remaining cornea is excised. Remnant tags of corneal tissue or Descemets membrane are rigorously trimmed flush with the scissors. The use of suction-assisted trephines, corresponding to Baron-Hessburg and Hanna trephination methods have the advantage of being able to retain the place of the trephine throughout trephination without undue downwards compression. Photogrammetric evaluation of host corneal trephination reveals that the Hanna trephination system presents the best precision and produces the most vertical minimize. In addition, these trephine techniques additionally achieve higher centration with the central gunsight of the Hanna trephine, and the crossed centration web site of the Barron-Hessburg trephine. However, sufficient suction may not always be simply achievable, corresponding to in small eyes or deformed globes, or when the ocular surface may be very irregular. It is particularly necessary that the donor and recipient edges are aligned correctly and that neither an override nor an underride exists. Poor apposition can intervene with reepithelialization of the graft and may lead to postoperative astigmatism. The use of an intraoperative keratoscope would help in distributing the strain of the graft by adjusting the tightness of sutures, thereby reducing postoperative astigmatism.
Effective zitromax 100mgPathophysiologically, sclerocornea might end result from developmental arrest of limbal anlage liable for each limbal differentiation and corneal curvature during neural crest migration, as is seen within the different mesenchymal dysgeneses. This maldevelopment, probably coupled with increased intraocular strain attributable to the angle abnormality, results in corneal opacity and thinning and to prominent buphthalmic enlargement of the complete anterior segment. Prognosis for keratoplasty as nicely as preservation of any functional vision is dismal. Detailed dialogue of the situation is offered here within the section dedicated to Corneal Endothelial Dystrophies. Top right, In this superior bilateral case with a number of congenital abnormalities, the complete cornea is sclerified, and the fantastic vascular arcades extend centrally from the conjunctiva and sclera. Middle proper, Transmission electron microscopy discloses a disorganized array of collagen fibrils that measure as a lot as 3 times normal diameter (52 500). Bottom inset, Light microscopy of the posterior cornea reveals irregularly thick and wavy stromal lamellae (S). Bottom right, Highermagnification electron micrograph of the area circled in backside left determine reveals multilaminar basement membrane materials interspersed with nice filaments (75 000). Epithelial Basement Membrane Dystrophy (Map�Dot�Fingerprint) Disorders involving the epithelium and its basement membrane may have a variable clinical appearance however in all probability involve a standard pathophysiology and clinical course. Because of the presumed primary abnormality in the epithelial basement membrane, even minor trauma could cause a serious epithelial breakdown, with impaired subsequent therapeutic. Top left, A 1-year-old lady was born with anterior staphyloma of the best eye and anterior section mesodermal dysgenesis of the left. The axial length is elongated to 24 mm because of disproportionate enlargement of the anterior section. Top proper, the left eye instantly after penetrating keratoplasty and anterior phase reconstruction. Middle left, Light microscopy of keratoplasty specimen shows secondary epithelial metaplasia into keratinized stratified squamous epithelium. Middle heart, Involved stroma of the identical specimen assumes the morphologic options of scleral tissue with the presence of plentiful blood vessels. Middle right, Transmission electron microscopy of the corneal stroma discloses abnormally thick (440 �) collagen fibrils (43 400). Bottom, Transmission electron microscopy of this similar space discloses iris pigment epithelial cells and stromal tissue lining the posterior corneal floor (6400). Hykin and colleagues92 prospectively examined 117 patients with histories of recurrent corneal erosions. They discovered that 23 had only epithelial basement membrane dystrophy with no history of trauma. Seventy-five sufferers had histories of trauma but no slit-lamp evidence of dystrophy. Williams and Buckley93 acknowledged that map�dot�fingerprint dystrophy is the most typical reason for recurrent erosion generally apply. Many ultrastructural studies of map�dot�fingerprint dystrophy have disclosed a discontinuous multilaminar, thickened basement membrane beneath the irregular epithelium. More widespread coalescence of this subepithelial materials gives the scientific maplike image. Other configurations of aberrant basement membrane and fibrillar collagen could be discovered extending in ridges into the epithelial layers, thus explaining the fingerprint sample. As they journey to the floor, they may coalesce with other cysts and, lastly, break via the surface, giving rise to an erosive episode. Unable to form correct hemidesmosomes or anchoring fibrils, the epithelium undergoes recurrent subclinical or overt episodes of dysadhesion. Moreover, intraepithelial extensions of abnormal basement membrane and collagenous materials may block the traditional surface migration of maturing epithelial cells, permitting the formation of encysted collections of particles. Thus, the cycle is to a level self-perpetuating, with primary faulty epithelial adhesion secondarily inflicting irregular epithelial maturation that, in turn, exacerbates the accumulation of irregular basement membrane and collagenous debris and leads to additional worsening of epithelial adhesion. Careful d�bridement of severely aberrant epithelium and, in some instances, superficial keratectomy to take away subepithelial particles are aids to conservative remedy with lubricants, hypertonic saline ointment, patching, or bandage soft contact lenses. When used as prophylaxis for recurrent erosion, one study confirmed no distinction between bland ointment and hypertonic saline ointment. Top left and heart, Clinical photograph of a 42-year-old lady with nontraumatic erosions exhibits traits of map dystrophy with superficial geographic haze interrupted by clear areas and few dots. Top right, Light microscopy of the medical dot sample reveals a large debris-containing intraepithelial cyst. Bottom right, Transmission electron microscopy of the evolving cyst that results from mobile dissolution leaving residual nonspecific cytoplasmic granular debris (asterisks) (8000). Top left and center, Two variants of fingerprint dystrophy show subepithelial ridges and appear refractile towards the pink fundus reflection. Top proper, Under direct illumination, in any other case faintly seen fingerprint lines are enhanced with fluorescein staining and cobalt mild. Bottom, Transmission electron microscopy of this same area discloses collagenous and granular composition of the subepithelial materials, in addition to cellular elements (asterisk), and an elaborate multilaminar basement membrane (bracketed area) loosely apposed to an undulating basal cell membrane (7000). Bottom, lower inset, Higher magnification of the bracketed space in backside determine resolves typical redundant laminations of the basement membrane (asterisks), underdeveloped hemidesmosomes (encircled areas), and absence of anchoring fibrils. Epithelial cells produce an abnormal multilaminar basement membrane, both within the normal location and intraepithelially. As the intraepithelial basement membrane thickens, it blocks the normal migration of epithelial cells towards the surface. Trapped epithelial cells degenerate to kind intraepithelial microcysts that slowly migrate to the surface. The abnormal basement membrane produces map and fingerprint changes, and microcysts produce the dot pattern seen clinically. Hereditary Epithelial Dystrophy (Meesmann, Stocker�Holt) the corneal dystrophy of Meesmann98�104 and of Stocker�Holt105 is a dominantly inherited abnormality of the corneal Corneal Dysgeneses, Dystrophies, and Degenerations contain a dense intracellular substance of unknown composition. In 1955, Stocker and Holt105 similarly described a dominantly inherited situation in patients 7 months to 70 years of age, characterised by gray, punctate, scattered corneal opacities that, with focal illumination, appeared as minute droplets. In some sufferers, this nodular thickening of the basement membrane produced an irregular epithelial floor. Densely packed clumps of microcysts throughout the opacities are evident on retroillumination. Vision is affected if the lesions contain the visual axis, however corneal erosions are infrequent. Light and electron microscopy show cycoplasmic vacuolization of all epithelial cells inside the affected areas. Both dystrophies are normally bilateral and symmetric and become evident in the first or second decade of life as painful recurrent erosive episodes. Patients develop decreased visual acuity due to anterior scarring and floor irregularity.

Diseases - Crandall syndrome
- Chromosome 1, q42 11 q42 12 duplication
- Exostoses, multiple, type 2
- Cutis verticis gyrata thyroid aplasia mental retardation
- Oligomeganephrony
- Leg absence deformity cataract
Discount zitromax 250mg lineVannas scissors are used to complete the removing of the lamellar keratectomy tissue as quickly as the inferior edge of the trephination is reached. If additional irregular stromal tissue is current, it may be removed by making a second deeper lamellar dissection. The needle is placed on a 3 mL air syringe after which launched bevel down into the bottom of the keratotomy incision. A partial-thickness anterior keratectomy is manually performed leaving a layer of posterior stroma intact anterior of the bubble. A sharp-tipped blade is used to rigorously penetrate the remaining stromal layers at the center of the cornea. A wire spatula is inserted into this central opening and advanced along the cleavage aircraft created by the air till its tip reaches the peripheral edge of the trephination groove. The technique involving intrastromal air injection to facilitate the deep lamellar dissection was initially described by Archila29 and later modified by Anwar. The base of the annular keratectomy incised by the trephine is inspected by opening the keratectomy with a zero. The again (dull) a half of a brilliant blade knife can be utilized to bluntly dissect to the specified depth. Another approach is to use intraoperative ultrasonic pachymetry and a micrometer-adjusted diamond knife to exactly establish the preliminary depth of the lamellar keratoplasty. A third approach for outlining the depth of the keratectomy has been described by Melles. A lamellar dissector or dull knife is positioned on the base of the annular keratectomy. At the air�endothelium interface, a specular mild reflex is created because the dissector indents and enters the stroma. The portion of the cornea posterior to the dissector 808 Lamellar Keratoplasty is seen as a darkish band between the tip of the dissector and the light reflex. The width of the darkish band is the thickness of posterior corneal tissue which can remain if a lamellar keratectomy is initiated at that specific stage. Once the depth of the keratectomy has been established, a Thornton ring is used to fixate and pressurize the attention and a lamellar pocket is dissected with a Paufique knife or related instrument. This pocket runs parallel to the posterior lamellae ~2�3 mm central to the edge of the base of the keratectomy incision and has a width of ~4 mm. Finally, Troutman corneal splitters or comparable lamellar dissectors are inserted into the first lamellar pocket and the posterior lamellae are separated using a rocking fan-like movement taking care to keep the dissection in a uniform horizontal aircraft until the whole space within the trephination has been dissected. Additional undermining peripheral to the trephination edge for 1�2 mm in the identical lamellar aircraft offers a pocket to help in dovetailing the donor graft to the recipient bed. The lamellar keratectomy is excised with Vannas scissors to expose the recipient bed. This is well done by injecting air via the optic nerve with a 30-gauge needle. A diamond knife is then set to the proper depth to acquire the desired thickness of the lamellar graft. The diamond knife is then used to minimize a 120� arc along the limbus of the donor globe. An anterior lamellar dissector is inserted into the base of the limbal incision and the posterior lamellae are separated utilizing a side-to-side sweeping movement. Care is taken to hold the dissector in the identical horizontal airplane until the dissection is full from limbus to limbus for the whole diameter of the donor cornea. If a particular shape of donor graft is desired (crescent or horseshoe), the entire diameter of the donor cornea is eliminated following the donor lamellar dissection and then this oversized graft is placed over the host recipient mattress and a graft is customary to fit the form of the recipient bed. A full-thickness stromal lamellar graft is obtained and could be trephined to the specified diameter. The microkeratome is out there with a variety of heads for slicing tissue from a hundred to 475 mm in thickness. The Moria microkeratome can be utilized with a complete globe, however corneal scleral rims can also be used with the Moria artificial chamber. The system facilitates donor tissue preparation with a easy floor and requires a minimal studying curve. The Barraquer cryolathe can be used to prepare smooth lamellar donor tissue with precise thickness and diameter. Use of corneal press to get hold of uniform hydration and thickness previous to cryolathing enhances the quality and precision of the lathed tissue. The donor tissue may be frozen for long-term storage or placed in tissue culture medium if surgery is deliberate within 1 week. Anterior stromal opacities which have a uniform thickness can be resected very efficiently with a microkeratome. One downside when using the microkeratome for lamellar resection is the inconsistency in the diameter of the resected tissue. Manual lamellar dissection was performed from the edge of the microkeratome resection to the sting of the trephination incision. This technique offers the advantage of a easy central host bed created by the microkeratome and a consistent and controlled bed diameter can be matched with donor tissue obtained by an analogous method. Typically, the size and the form of the recipient mattress are determined only after the abnormal tissue has been fully eliminated. A reliable technique for lamellar tissue resection is to outline the area to be eliminated with a diamond knife set to an appropriate depth. The lamellar resection of irregular tissue should lengthen ~1 mm into the healthy recipient tissue to guarantee a recipient mattress with secure margins. Supplementary undermining of the peripheral margins of the recipient mattress will help in securing the donor graft. Suboptimal visible acuity following lamellar keratoplasty is commonly blamed on interface haze but inferior visible results also happen if the posterior curvature of the recipient mattress is irregular. This abnormal posterior curvature could also be the most effective explanation for poor visual outcomes following lamellar keratoplasty for keratoconus even when the interface is completely clear. Manche reported excellent imaginative and prescient in two sufferers using sodium hyaluronate-assisted lamellar keratoplasty. However, all eyes were successfully treated with the lamellar keratoplasty method and no difference in visual acuity or endothelial cell depend was reported within the punctured versus nonpunctured group. Inferior visual acuity after lamellar keratoplasty is just as more doubtless to end result from an irregular posterior curvature. This is certainly the best rationalization for inferior visible outcomes obtained when lamellar keratoplasty is used to deal with keratoconus. This system permits for the preparation of the lamellar keratoplasty tissue using a donor corneal scleral rim which is secured onto the artificial chamber platform. The diameter of the donor tissue is set by adjusting the peak of the donor tissue protruding above the artificial chamber opening. An evaluation of the results and complication charges of these techniques provides an evidence-based strategy for choosing the optimal procedure. Lamellar Keratoplasty topographically measured with Orbscan, are particularly troublesome to remove with lamellar keratoplasty in older patients. These identical adjustments are much simpler to reverse in younger sufferers, which explains why youthful sufferers obtain better and sooner visible outcomes following lamellar keratoplasty than older patients.
Purchase zitromax 500mg fast deliveryFreidmann-Kein A, LaFleur F, Gendler E, et al: Herpes zoster: a attainable scientific signal for growth of acquired immune deficiency syndrome in high risk individuals. Vanhems P, Voisin L, Gayet-Ageron A, et al: the incidence of herpes zoster is much less probably than other opportunistic infections to be lowered by extremely lively antiretroviral remedy. Litoff D, Catalano R: Herpes zoster optic neuritis in human immunodeficiency virus an infection. McGill J, Chapman C: Comparison of topical acyclovir with steroids within the therapy of herpes zoster keratouveitis. Aylward G, Claoue C, Marsh R, et al: Influence of oral acyclovir on ocular problems of herpes zoster ophthalmicus. Colin J, Prisant O, Cochener B, et al: A double blind randomized trial to evaluate the efficacy and security of valaciclovir and acyclovir for treatment of herpes zoster ophthalmicus. Tyring S, Beutner K, Tucker B, et al: Antiviral therapy for herpes zoster: randomized controlled clinical trial of valacyclovir and famciclovir remedy in immunocompetent sufferers 50 years and older. Gheeraert P, Group: Efficacy and safety of famciclovir in the therapy of uncomplicated herpes zoster. Tyring S: Famiciclovir remedy (Famvir) for herpes simplex and herpes zoster infections. Tyring S, Belanger R, Bezwoda W, et al: A randomized, double-blind trial of famciclovir versus acyclovir for the remedy of localized dermatomal herpes zoster in immunocompromised sufferers. The National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. Wood M, Johnson R, McKendrick M, et al: A randomized trial of acyclovir for 7 days and 21 days with and without prednisolone for therapy of acute herpes zoster. Levin J, Gordon N, Smith R, et al: Desipramine enhances opiate postoperative analgesia. Urban B, France R, Steinberger E, et al: Longer term use of narcotic/antidepressant treatment within the management of phantom limb pain. Wasner G, Kleinert A, Binder A, et al: Postherpetic neuralgia: topical lidocaine is effective in nociceptor-deprived pores and skin. Bowsher D: the effects of preemptive remedy of postherpetic neuralgia with amitriptyline: a randomized, double-blind, placebo-controlled trial. Satterthwaite J, Tollison C, Kriegel M: Use of tricyclic antidepressants for the remedy of intractable pain. Watson C, Vernich L, Chipman M, et al: Nortriptyline versus amitriptyline in postherpetic neuralgia: a randomized trial. Kvinesdal B, Molin J, Froland A, et al: Imipramine remedy of painful diabetic neuropathy. Bowsher D: Factors influencing the options of postherpetic neuralgia and outcome when treated with tricyclics. Galen B: Neuropathic pain of peripheral origin: advances in pharmacologic remedy. Berger A, Dukes E, McCarberg B, et al: Change in opioid use after the initiation of gabapentin remedy in patients with postherpetic neuralgia. Rowbotham M, Harden N, Stacey B, et al: Gabapentin for the therapy of postherpetic neuralgia: a randomized managed trial. Gain P, Thuret G, Chiquet C, et al: Frontal and nasal nerve blocks within the remedy of extreme pain in acute ophthalmic zoster. Gain P, Thuret G, Chiquet C, et al: Facial anesthetic blocks in the therapy of acute pain during ophthalmic zoster. Tanure M, Cohen E, Grewal S, et al: Penetrating keratoplasty for varicella-zoster virus keratopathy. Henle G, Henle W: Observations on childhood infections with the Epstein-Barr virus. Sugiyama K, Ito M, Ichimi R, et al: A case of Epstein-Barr virus infection with exophthalmos and ocular muscle swelling. Pflugfelder S, Crouse C, Atherton S: Ophthalmic manifestations of Epstein-Barr virus infection. Pflugfelder S, Huang C, Crouse C: EpsteinBarr virus keratitits after a facial chemical peel. Pflugfelder S, Tseng S, Pepose J, et al: Epstein-Barr virus infection and immunologic dysfunction in sufferers with aqueous tear deficiency. Pinnolis M, McCulley J: Nummular keratitis associated with infectious mononucleosis. Morishima N, Miyakawa S, Akazawa Y, et al: A case of uveitis associated with continual active Epstein-Barr virus an infection. Onorato I, Morens D, Martone W, et al: Epidemiology of cytomegalovirus infections. Garau J, Kabins S, DeNassquo S, et al: Spontaneous cytomegalovirus mononucleosis with conjunctivitis. Weller T: the cytomegaloviruses: ubiquitous agents with protean clinical manifestations. Holland E, Bennett S, Brannian R, et al: the risk of cytomegalovirus transmission by penetrating keratoplasty. Mietz H, Aisenbrey S, Ulrich Bartz-Schmidt K, et al: Ganciclovir for the remedy of anterior uveitis, Graefes Arch Clin Exp Ophthalmol 2000; 238:905�909. Azar M, Dhaliwal K, Bower K, et al: Possible consequences of shaking arms with your sufferers with epidemic keratoconjunctivitis. Laibson P, Ortolan G, Dupre-Strachan S: Community and hospital outbreak of epidemic keratoconjunctivitis. Uchio E, Takeuchi S, Itoh N, et al: Clinical and epidemiological features of acute follicular conjunctivitis with particular reference to that caused by herpes simplex virus type 1. Dawson C, Hanna M, Wood T, et al: Adenovirus sort 8 keratoconjunctivitis in the United States. Laibson P, Dhiri S, Oconer J, et al: Corneal infiltrates in epidemic keratoconjunctivitis: response to double blind corticosteroid remedy. Harnett G, Newnham W: Isolation of adenovirus sort 19 from the male and female genital tracts. Boniuk M, Philips C, Friedman J, et al: Chronic adenovirus sort 2 keratitis in man. Darougar S, Quinlan J, Gibson J, et al: Epidemic keratoconjunctivitis and continual papillary conjunctivitis in London because of adenovirus type 19. Pettit T, Holland G: Chronic keratoconjunctivitis related to ocular adenovirus infection. Pavan-Langston D, Dohlman C: A double blind clinical study of adenine arabinoside therapy of viral keratoconjunctivitis.
Buy discount zitromaxAn imaging research of the orbits with skinny cuts and with attention to the lacrimal gland is useful in confirming the localization of the tumor to the conjunctiva. Because growth of systemic illness might occur years after the analysis of main conjunctival lymphomas, repeat systemic evaluation is recommended at 6 months interval for a minimal of 5 years. However, for intermediate-grade and high-grade tumors, radiotherapy remains the remedy of choice for native management. Patients with systemic illness are candidates for systemic chemotherapy along with any local therapy. Therefore if the lymphoma is localized to the conjunctiva and is low-grade, an affordable option could additionally be to defer treatment and observe for signs of recurrence or development of the tumor. Lin A, Stern G: Correlation between pterygium size and induced corneal astigmatism. Alaniz-Camino F: the utilization of postoperative beta radiation in the remedy of pterygia. Nakamura Y, Mashima Y, Kameyama K, et al: Detection of human papillomavirus infection in squamous tumours of the conjunctiva and lacrimal sac by immunohistochemistry, in-situ hybridization and polymerase chain reaction. Tabin G, Levin S, Snibson G, et al: Late recurrences and the need for long-term follow-up in corneal and conjunctival intraepithelial neoplasia. Frucht-Pery J, Sugar J, Baum J, et al: Mitomycin C therapy for conjunctivalcorneal intraepithelial neoplasia: a multicenter expertise. Seregard S, Kock E: Squamous spindle cell carcinoma of the conjunctiva; deadly outcome of a pterygium-like lesion. Tanaka M, Okisaka S, Nakayasu K, Kanai A: Clinical importance of inclusion cysts of nevi within the bulbar conjunctiva. Risk factors for recurrence, exenteration, metastasis, and death in one hundred fifty consecutive patients. Lamellar keratoplasty remained the preferred form of corneal transplant via the primary decade of the twentieth century and was endorsed by notable luminaries including Fuchs and Elshnig. Using an experimental rabbit model, he described a healing process by which donor tissue appeared to mildew along with recipient tissue. In 1840, M�hlbauer appearing on ideas espoused by von Walther developed an animal mannequin for lamellar keratoplasty utilizing triangular-shaped grafts. He designed a mechanical circular trephine that rotated automatically via a spring in its head and produced a vertical partial depth incision for lamellar keratoplasty. He additionally advocated using heteroplastic donor tissue after experiencing an endophthalmitis utilizing human donor tissue and because of his influence xenotransplantation remained popular by way of the first decade of the 20 th century. Magitot reported a lamellar homograft that remained clear for 1 12 months after surgical procedure. Lamellar keratoplasty became much less popular and by the late 1930s was not often performed by corneal surgeons with the notable exception of Louis Paufique. As a outcome, Paufique developed and refined his method for lamellar keratoplasty between 1943 and 1947, culminating in the landmark work Les Greffes de la Corn�e. Most corneal surgeons keep away from lamellar keratoplasty due to its perceived surgical problem and the broadly held belief that penetrating keratoplasty yields superior outcomes. However, recent improved microsurgical methods and instrumentation have led to elevated curiosity in lamellar keratoplasty. Since lamellar keratoplasty is an extraocular process, complications corresponding to endophthalmitis, expulsive hemorrhage, glaucoma, and cataract formation are mitigated. However, an important advantage is the host endothelium is spared, eliminating the potential for endothelial rejection, the main cause of graft failure following penetrating keratoplasty. Penetrating grafts reveal a pronounced endothelial cell loss in the first 12 months and progressive endothelial cell loss every following 12 months. Alternatively, lamellar keratoplasty reduces endothelial cell density by ~10% after 1 12 months followed by regular physiological cell loss. The indications, method, outcomes, and problems of lamellar keratoplasty are coated on this chapter. Lamellar keratoplasty avoids the complications of endothelial graft rejection and delayed endothelial cell loss seen with penetrating keratoplasty. Lamellar keratoplaty is an different selection to penetrating keratoplasty for the surgical treatment of keratoconus, corneal complications following refrective surgical procedure and corneal scars after infectious keratitis. One of the commonest indications for optical lamellar keratoplasty is contactlens-intolerant keratoconus. After lamellar keratoplasty, such sufferers are visually rehabilitated without fear of future endothelial graft reactions. Optical lamellar keratoplasty can additionally be helpful for the treatment of anterior stromal scars following trauma or infectious keratitis. Reis�B�ckler dystrophy commonly recurs in lamellar grafts but this downside is safely managed by replacing the graft. The interweaving configuration makes handbook lamellar dissection tough at this stage. Some of the extra creative shapes for tectonic lamellar keratoplasty include horseshoe- and crescent-shaped grafts. But the underlying cause for the corneal melt should be treated or the tectonic graft will fail on account of corneal melting. In the case of herpes zoster, inferior corneal melting is usually associated with exposure keratitis secondary to lagophthalmus, so the tectonic graft should be mixed with a lateral tarsarrophy. Anteriorly, the lamellae are interwoven and infrequently oriented obliquely to the corneal floor. In the posterior two-thirds of the stroma, the lamellae are oriented parallel to the corneal surface. Collagen interweaving can be extra extensive within the corneal periphery than in its heart. Different lamellar keratoplasty strategies that apply this knowledge are described beneath. A minimal trephination depth of 300 mm is beneficial to insure that the lamellar dissection begins within posterior stromal lamellae. Lamellar dissection of the anterior stroma may be very difficult because of the interlacing of these lamellae and even when the pathology is just present inside these lamellae the trephine depth ought to be set to guarantee reaching the level of posterior stroma. This initial lamellar dissection solely extends 3 mm axially from the inside edge of the trephine incision. No additional central extension of the lamellar dissection should be performed till this 3 mm dissection is accomplished alongside the periphery of the inner side of the trephine cut for 270�. Dissection of the peripheral interlacing corneal lamellae reduces the cohesive pressure required to extend the lamellar dissection axially and allows for a a lot easier and safer dissection of the central posterior lamellae. After completion of the 270� peripheral lamellar dissection, the central corneal lamellae could be peeled away by utilizing a Pollack forceps or another similar two-point fixation forceps. Using the Pollack forceps sustained upward, central traction is utilized to the inside fringe of the keratectomy tissue. The cohesive power of the peripheral and anterior stroma is greater than the central and posterior stroma.
Buy zitromax 500 mg low priceEndothelium bridges the hole in 6�8 weeks, with resultant stromal deturgescence and residual stromal scarring of varying severity. Although the abrupt onset of often huge corneal edema and profound visible loss is startling, management stays conservative medical therapy (patching, bandage gentle contact lens, lubricants, hypertonic brokers and sometimes topical steroids) plus reassurance that the state of affairs should resolve spontaneously inside 3 months. Top left, Clinical photograph in lateral projection demonstrates extreme anterior protrusion of the markedly ectatic cornea. The V-shaped conformation of the decrease lid is produced by the ectatic cornea in downgaze. Upper center right, Keratoscopic view of typical egg-shaped appearance of the central corneal mires caused by inferotemporal steepening. Lower center left, Corneal retroillumination is a useful approach to identify the place and extent of the cone. New regenerated endothelium (ne) traces the anterior floor of the ledge and posterior stroma (s). The affiliation with atopy and vernal keratoconjunctivitis has led to hypothesis that frequent, vigorous eye rubbing could worsen, accelerate, or even trigger keratoconus. When lens match or comfort turns into an issue due to a focal elevated pannus over the apex of the cone, superficial keratectomy may be carried out to smooth the corneal floor. Excimer laser phototherapeutic keratectomy may be cautiously relevant in comparable circumstances. In most instances, nevertheless, penetrating keratoplasty stays a highly profitable process of selection for long-term visible rehabilitation of advanced instances. The protruding cornea often is central to the area of thinning and remains of regular thickness (see Table forty three. These corneas are clear, avascular, and with out apical scarring, lipid deposition, or iron ring. There is a few consensus that keratoconus, keratotorus, keratoglobus, and pellucid degeneration are related as a result of these completely different conditions have been found to coexist in families. Histopathologic reviews demonstrate similar abnormalities in these varied issues. Because of extraordinarily irregular corneal topography, the therapy of pellucid zone degeneration is difficult. If the affected person is contact lens intolerant, a large-diameter, penetrating keratoplasty could additionally be carried out. Spectacle correction may help to achieve useful imaginative and prescient along with providing protection from corneal rupture. Left top and backside, Clinical images feature corneal ectasia occurring above the slender band of clear, skinny, nonvascularized cornea that parallels the inferior limbus (arrows). Right top and bottom, Slit-lamp view and corresponding illustration show normal corneal thickness central and peripheral to the band of thinning (arrow). Left, Clinical photograph of acquired keratoglobus exhibits globoid protrusion of clear, diffusely thin cornea. Right, Horizontal pupil�optic nerve part of this eye reveals bulging cornea and deep anterior chamber. The complete cornea is about one-third normal thickness, except in excessive periphery nasally and temporally. Alternative surgical approaches embrace crescentic lamellar keratoplasty, thermokeratoplasty, epikeratoplasty, and wedge or crescentic resection. The sort I limbal girdle is prone to be extra closely associated to early calcific band keratopathy as a result of it appears, as Vogt described it, as a white band with clear holes at several points and separated from the sclera by a clear interval. Both the juvenile and the adult varieties represent paralimbal stromal accumulations of ldl cholesterol esters, triglycerides, and phospholipids. Diseases causing an increase in b-lipoproteins include nephrotic syndrome, hypothyroidism, elevated ldl cholesterol intake, obstructive jaundice, and diabetic ketoacidosis. Rare lipoprotein issues causing arcus or generalized corneal clouding embody lecithin ldl cholesterol acyltransferase deficiency and Tangier illness. Idiopathic Furrow Degeneration Thinning of the cornea in older individuals within the space of an arcus senilis sometimes happens. Postirradiation Thinning Noninflammatory corneal excavation at the limbus could happen after excessive native doses of b-radiation. It is often bilateral, though typically asymmetric, and is seen primarily in youthful men. The condition progresses slowly over the course of years and customarily starts superiorly as a marginal opacification. Difficulties arise from the induced corneal astigmatism, and minor trauma could lead to rupture if thinning is sufficient. It is a white opacity in the medial and temporal limbal regions and could also be mistaken for corneal arcus. Left, the arcus lipoides shows a dense white annular opacity of the peripheral stroma. Right, At greater magnification, an intervening zone of clear stroma separates lipid deposition from the limbus. Top left, Clinical photograph of a affected person with polyarteritis nodosa shows a full-ring ulcer and related lipid deposition close to the limbus. Top proper, Light microscopy of the identical eye illustrates peripheral corneal thinning (arrows) similar to the area of medical ulceration. Bottom left, Severe necrotizing vasculitis of a medium-caliber artery confirms the prognosis. Bottom right, Light microscopy of a 47-year-old woman with rheumatoid arthritis who developed a perforated marginal corneal ulcer exhibits adherent iris included right into a fibrous scar. A Mooren-like ulcer has been reported after cataract surgical procedure,357 penetrating keratoplasty,358 corneal trauma and chemical burns,359 herpes zoster virus infection,360 syphilis, and tuberculosis. This kind is usually unilateral and responds to remedy extra typically than the extra severe kind that happens in youthful sufferers. Top right, Higher magnification discloses vascularization of the involved stroma with lipid deposition at the advancing edge. Bottom inset, Light microscopy reveals numerous foamy histiocytic cells and blood vessels (asterisk) within the anterior stroma. Bottom, Transmission electron micrograph shows histiocytic cells laden with neutral lipid inclusions (circled area). In extra aggressive circumstances, perforation may occur from collagenolytic processes or secondary infection, particularly within the potentiating presence of topical corticosteroids. Tissue adhesive and lamellar grafting could additionally be essential in the occasion of perforation. It was originally thought to be lipid in nature but in all probability contains iron from the international physique. There is often a history of prior corneal inflammatory episodes with resultant stromal vascularization. The lipid accumulations are, due to this fact, of a secondary nature, with extravasation of cholesterol and fatty acids from the vessels.
References - Schumacher S, Fichtner J, Stein R, et al: Pregnancy after Mainz pouch urinary diversion, J Urol 158:1362n1364, 1997.
- Sun Y, Chai TC: Up-regulation of P2X3 receptor during stretch of bladder urothelial cells from patients with interstitial cystitis, J Urol 171(1):448n452, 2004.
- Andrade EL, Forner S, Bento AF, et al: TRPA1 receptor modulation attenuates bladder overactivity induced by spinal cord injury, Am J Physiol Renal Physiol 300(5):F1223nF1234, 2011.
- Misell LM, Holochwost D, Boban D, et al: A stable isotope/mass spectrometric method for measuring the kinetics of human spermatogenesis in vivo, J Urol 175:242n246, 2006.
|
|