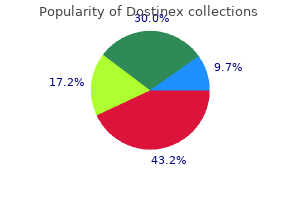
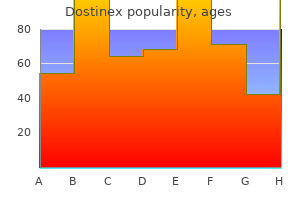
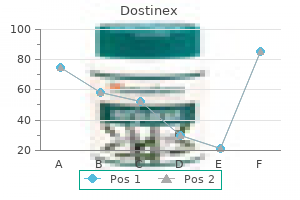
"Buy dostinex, menstruation 101."By: Noreen A Hynes, M.D., M.P.H. - Director, Geographic Medicine Center of the Division of Infectious Diseases
- Associate Professor of Medicine
 https://www.hopkinsmedicine.org/profiles/results/directory/profile/0010761/noreen-hynes
Purchase discount dostinex on-lineHowever, incising the decrease furrow and advancing the flap superiorly has additionally been carried out successfully. If the amount of brow skin to be resected coincides with a phase of skin between two furrows, much less scarring and a better smoothing effect can be obtained. B, the anterior flap is elevated till the forehead position is right, the overlap is resected, and the incision is closed with galeal and pores and skin closure. Chapter 6 � Surgical Rejuvenation of the Forehead and Eyebrows 219 Flap growth may be subgaleal or subcutaneous. Although a subgaleal flap is simpler to elevate and shut with a shorter scar, it transects the sensory nerves, inflicting brow numbness postoperatively. When a subgaleal flap is used, separate galeal closure is required, which reduces the stress on the pores and skin and subcutaneous flaps. B, He had a midforehead coronal incision for a brow carry, combined with an higher blepharoplasty. He is proven 3 months postoperatively, with a softening midforehead scar and repositioning of the eyebrows with proper spacing. B, Three months after a coronal midforehead lift and an higher blepharoplasty, the incision site is softening, brow position and spacing are restored, and the brow rhytids are decreased. The lifting impact of the classic direct forehead lift depends on the dimensions of the pores and skin excision. Our method requires a really brief and thin skin excision solely within the central and lateral a half of the forehead over the apex and leads to a small scar. The lifting energy of this technique relies upon not on the quantity of skin excised however on fixation of the forehead tissue to the frontalis muscle. In males, the small line caused by the incision is almost invariably much less visible than the prevailing brow creases current in most aged men. The vertical width of the skin excision by no means exceeds 6 mm and often is narrower. To facilitate excision of skin and subdermal brow fats, a small pores and skin hook is positioned in the nasal end of the wound for higher traction so that the section of incised skin could be tensed. The subdermal fats pad in the plane of the frontalis muscle is undermined with sharp scissors. The ellipse of skin and fats is undermined from the underlying frontalis muscle and excised. Efforts are made to produce perpendicular skin and flap edges to the excised area. The deep fatty edges of the wound are squared with a coagulating Bovie tip by sculpting the fats from the frontalis muscle. Two to three 4-0 Mersilene mattress sutures are introduced, first into the subbrow fat pad after which into the frontalis muscle under the undermined superior edge of the wound. The mattress sutures ought to be at the base of the brow fats on the forehead facet of the incision, and into the frontalis muscle on the undermined side of the incision. The upper fringe of the incision is undermined within the airplane of the frontalis muscle. B, the brow tissue is sutured to the frontalis muscle, advancing the brow upward to create a frontalis suspension of the forehead. C, A typical excision of suprabrow tissue, including pores and skin, dermis, and subcutane- Additional closure is obtained with intradermal sutures of 4-0 Vicryl and skin sutures of 6-0 nylon. Patients who desire a less invasive process and are much less involved with the forehead, however rather need minimal lateral forehead elevation, significantly combined with an upper blepharoplasty, are good candidates for a direct forehead raise. The results embrace delicate elevation of the lateral forehead, but more noticeably, an improved results of blepharoplasty. However, an higher blepharoplasty alone would have created brow ptosis because of the loss of compensatory frontalis action. B, He had a four-lid blepharoplasty with direct forehead fixation to stabilize the forehead in a traditional position. Correcting the higher lid ptosis alone would have eradicated compensatory arching of the brows, but would have brought on postoperative eyebrow ptosis. B, He is shown 3 months after ptosis restore, combined with a direct forehead carry and an higher and decrease lid blepharoplasty. B, He is shown 5 months after brow-lid blepharoplasty and a direct forehead raise to stabilize the brow-lash distance and stop postoperative forehead ptosis. D, Initial, deep suturing of the brow to the frontalis muscle with 4-0 Mersilene sutures. This is a worst-case scenario; however, the response in the incision line subsided after a couple of more weeks. Most sufferers with smaller incisions and fewer reactive skin have imperceptible scarring. Endoscopic eyebrow-forehead lifts and temporal lifts are the most common adjunctive brow procedures we use. These procedures additionally provide surgical correction of glabellar frown lines, medial and lateral brow ptosis, lateral temporal fullness, and periorbital smile traces. Endoscopic forehead lifts have proved efficient for reducing the scarring and morbidity associated with coronal brow lifts. It could be carried out as an isolated process, or it can be effectively mixed with upper blepharoplasty procedures. Additional know-how and gear are required, but the advantages of the process justify the extra expense. Complications have been few, and the general acceptance from sufferers and surgeons is high. In particular situations, various brow procedures can be useful, together with a direct brow lift, a traditional coronal raise, and a pretrichial biplanar carry. Subcutaneous temporal brow lift underneath native anesthesia: a useful technique for periorbital rejuvenation. Safety and efficacy of mixed higher blepharoplasties and open coronal brow carry: a consecutive collection of 600 patients. Identifying perfect forehead vector place: empirical analysis of three brow archetypes. Reducing the subconscious frown by endoscopic resection of the corrugator muscles. Presented on the Annual Meeting of the Los Angeles County Society of Plastic Surgeons, Los Angeles, Sept 1992. Comparison of subperiosteal vs subgaleal elevation techniques utilized in brow lifts. Commentary on: Subcutaneous temporal browlift under native anesthesia: a useful method for periorbital rejuvenation. In pursuit of optimal rejuvenation of the forehead: endoscopic brow raise with simultaneous carbon dioxide laser resurfacing. The sentinel vein: an necessary reference point for surgery in the temporal region. Therefore surgeons should have a low threshold for forehead instability and carry out brow stabilizing or lifting procedures throughout an upper blepharoplasty to reduce postoperative dissatisfaction and improve success. However, correct judgment is important to prevent overresection of skin, which can cause an unnatural aesthetic result and practical issues such as scarring, lagophthalmos, and corneal publicity.

Generic dostinex 0.25 mg free shippingOur present advice is to postpone lung transplantation in patients with established bone marrow illnesses. Treatment of those sufferers should, in any event, be performed by a specialised group with genetic experience. The triad is current in childhood, and bone marrow failure appears between the age of 10 and 20 years. These patients develop extreme pulmonary issues after haematopoietic stem-cell transplantation [37]. The coexistence of pulmonary fibrosis and bone marrow failure in a given particular person or in a family with autosomal dominant transmission is highly suggestive of telomerase complex mutation [42]. Patients with the same mutation, even in the same household, may current regular or elevated liver enzymes with variable levels of necrosis, inflammation, fibrosis and regeneration on liver histology [45]. All nine patients presented hepatopulmonary syndrome, defined as liver disease associated with evidence of intrapulmonary vascular dilatation leading to pulmonary gasoline trade abnormalities and hypoxaemia. Among the six patients with obtainable liver biopsy, the most common abnormality was nodular regenerative hyperplasia (n=4). Two sufferers received liver transplantation and developed lung fibrosis 18 months and 12 years later, respectively. Other manifestations Other manifestations linked to telomeropathy have been described, similar to cellular or humoral immunodeficiency, exudative retinopathies, central neurological involvement with cerebral calcifications and gastrointestinal bleeding [47, 48]. It is related to 4 of the six following traits: microcephalia, cerebellar hypoplasia, delayed pre-natal growth, delayed improvement, immunodeficiency and bone marrow failure. Telomere length has been measured in circulating leukocytes or in pulmonary epithelial cells [14, 50]. Telomere length diminishes physiologically with age by approximately 20% between 20 and 80 years of age [50]. It also diminishes within the case of exposure to tobacco or pesticides and in quite a few continual diseases [51�53]. This observation is in line with the speculation of telomeropathies with a qualitative and nonquantitative defect and not utilizing a discount in telomere measurement [54]. This may clarify, on the one hand, the phenomenon of genetic anticipation in families with the mutation, characterised by an earlier onset of the illness from era to technology and, however, an enhanced risk of pulmonary fibrosis with out transmission of the mutation due to transmission of shortened telomeres in a given family [57, 58]. However, neomutations are frequent and will explain as many as 50% of the cases [69]. The most frequent radiological sample associates predominant ground-glass opacities, septal thickening and cysts of variable measurement with a predominant distribution in the superior lobes [70�72]. In youngsters, totally different therapies have been reported with success: methylprednisolone, hydroxychloroquine and azithromycin [71, 74, 75]. Transmission was autosomal dominant with a phenotype associating early pulmonary fibrosis and lung cancer [77, 78]. All children with biallelic frameshift and nonsense mutations introduced with respiratory failure at birth. Biallelic missense, predicted splice site mutations or insertion/deletions had been related to older age of presentation and better prognosis. Other syndromes with pulmonary fibrosis associated with monogenic issues In addition to genetic problems linked to mutations of surfactant or telomerase complex genes, pulmonary fibrosis has been described during certain rare familial syndromes (table 1). Hermansky�Pudlak syndrome is a genetic disorder associated with defective lysosome-related organelles [83]. Depending on the mutated gene, as much as 80% of sufferers can present pulmonary fibrosis [85]. Two trials evaluated the impact of pirfenidone versus placebo, but contradictory results have been reported [87, 88]. The other, with 21 sufferers, reported a slowing of lung perform decline in handled sufferers [88]. Moreover, epigenetic regulation mechanisms might contribute to sure forms of familial pulmonary fibrosis. Genetic prognosis and counselling When a genetic type of pulmonary fibrosis is suspected, there are at present no guidelines on the genes to be analysed. The search for telomerase advanced mutations is also performed for sufferers with pulmonary fibrosis and suspected telomere syndrome. Without any mutation identified, a extra superior genetic analysis corresponding to exome sequencing may be thought of. In instances the place a mutation is recognized in the index case, the dangers to relatives can be evaluated based on the sort of transmission and the diploma of kinship. This may be specified by molecular exploration for these relatives who request it. In any case, sufferers should be inspired to avoid all poisonous factors, whether or not respiratory, hepatic or medullar, and especially tobacco smoke, environmental toxins and cytotoxic medicine. Regarding the risk of anticipation and the pleiotropic effects of telomerase complex mutations, genetic counselling has to be thought-about utilizing a multidisciplinary strategy and mentioned case by case. Telomerase advanced gene mutations are most frequently present in familial pulmonary fibrosis. Surfactant gene mutations are most frequently found in youngsters and could additionally be thought-about in young adults. However, some households also require recommendation from gynaecologists, nephrologists or rheumatologists. The first analysis is based on an explanation of the potential risks and a medical analysis, and, if the topic agrees, a complete blood count, liver blood test and genetic testing are performed. Conclusion Familial pulmonary fibrosis is relatively frequent and raises specific issues. Approximately 25% of households have an recognized mutation and may benefit from specific genetic counselling. Current research goal to identify new genes by full exome sequencing techniques in order to improve this proportion and develop specific therapies. Beyond physiopathological knowledge, detection of those mutations has sensible consequence for sufferers. Comprehensive cystic fibrosis mutation epidemiology and haplotype characterization in a southern Italian population. Nationwide prevalence of sporadic and familial idiopathic pulmonary fibrosis: evidence of founder impact amongst multiplex families in Finland. Familial pulmonary fibrosis is the strongest threat issue for idiopathic pulmonary fibrosis. A familial history of pulmonary fibrosis in sufferers with continual hypersensitivity pneumonitis. Familial idiopathic interstitial pneumonia: histopathology and survival in 30 sufferers. A Newfoundland cohort of familial and sporadic idiopathic pulmonary fibrosis patients: medical and genetic options.
Buy dostinexAlthough biofilms are very rare, they could be responsible for a few of the issues that had been previously reported as allergic reactions to fillers. Biofilms usually develop inside weeks after administration of the filler and current as erythematous, mildly tender nodules. If a tender nodule is current over the filler, administration of a broad-spectrum bactericidal antimicrobial agent for 2 to 3 weeks should be prescribed. Prevention of biofilms is essential in any generally carried out aesthetic procedure. A proper standard of care must be used to forestall any infection by acceptable aseptic precautions each earlier than and after the procedure: � All make-up ought to be cleaned off the skin and the world completely cleansed with either Hibiclens/alcohol pads or povidone-iodine before filler is injected. They can happen with all injectable dermal fillers and appear inside a number of months to years after injection, compared with 2 to four weeks for early nodules. If these measures end in repeated failure, surgical excision is the treatment of selection. This vascular event must be instantly acknowledged, and aggressive remedy must be performed to reverse the complications. The opposed occasion presents with mottled or blue skin appearance, edema to numerous levels, and should have an early or a delayed onset. These include the dorsal nasal arteries, angular artery and zygomaticotemporal, zygomaticofacial arteries. When stress is released the material moves distally into the retinal artery inflicting visible impairment or blindness. When injecting within the space of the mentioned vessels, hypodermic and microcannula needles should be instantly in touch with the bone. If the affected person reviews eye pain, altered vision, or blindness during injection of a filler, the physician needs to act expeditiously to keep away from a potentially catastrophic outcome. The first selection is to get the patient to an ophthalmology colleague as quickly as potential, whether or not to his or her office or to the emergency division. If need be, 911 must be known as to have an ambulance come to transfer the patient to the ophthalmologist. The use of blunt cannulas on this space may help to stop the risk of intraarterial injection. There are a number of forms of filler that could be chosen for various areas of the face. Forehead and glabellar strains can be improved with filler injections, and this can be mixed with botulinum injections to weaken the muscles that contribute to the traces. Filler is used to elevate the lateral forehead in addition to appropriate higher and lower eyelid hollowness. The tear trough deformity can be significantly improved with small volumes of filler, providing the affected person an different to surgery. This is an area the place technical finesse is essential to avoid overinjection, which could be visible and troublesome to right. The malar area is improved with the addition of quantity, adding a youthful angularity to the midface. The injection of filler to the nasolabial folds is also very effective for improving facial aesthetics. The injector must pay attention to the potential complications related to dermal fillers and knowledgeable about how to keep away from and manage them. Advances in facial rejuvenation: botulinum toxin sort a, hyaluronic acid dermal fillers, and mixture therapies- consensus suggestions. Treatment of hyaluronic acid filler-induced impending necrosis with hyaluronidase: consensus recommendations. Late-onset antagonistic reactions related to hyaluronic Acid dermal filler for aesthetic soft tissue augmentation. Aesthetic purposes of calcium hydroxylapatite volumizing filler: an evidence-based review and dialogue of present concepts: (part 1 of 2). A multicenter, single-blind randomized, managed examine of a volumizing hyaluronic acid filler for midface quantity deficit: patient-reported outcomes at 2 years. Facial soft-tissue fillers: assessing the state of the science conference-proceedings report. Lasers, fillers, and neurotoxins: avoiding issues within the cosmetic facial follow. Double-blind, randomized, controlled medical trial to evaluate security and efficacy of a metallic cannula with that of a standard needle for gentle tissue augmentation of the nasolabial folds. Efficacy and security of injection with poly-L-lactic acid compared with hyaluronic acid for correction of nasolabial fold: a randomized, evaluator-blinded, comparative research. Reliable delicate tissue augmentation: a scientific comparability of injectable soft-tissue fillers for facial-volume augmentation. Hyaluronic acid fillers and botulinum toxin kind A: a rationale for his or her individual and mixed use for facial rejuvenation. Minimizing pain, maximizing consolation: a new method for facial filler injections. Improvement of tear trough by monophasic hyaluronic Acid and calcium hydroxylapatite. Kosowski Key Points � Botulinum toxin is probably certainly one of the mostly used nonsurgical remedies for periorbital rejuvenation. Botulinum toxin has the power to lift the lateral forehead and enhance brow asymmetry. Botulinum toxin injection is essentially the most regularly performed cosmetic process in the United States. Although the primary revealed use of botulinum for wrinkle reduction was in 1992, ophthalmologists have been utilizing it to deal with strabismus and blepharospasm for the rationale that 1970s. Media attention has brought botulinum toxin to the forefront of facial rejuvenation, typically touted as a substitute for or a approach to postpone surgical procedure. Given its popularity among sufferers, periorbital surgeons must be conversant in its indications and limitations. In this chapter we describe the use of botulinum toxin for brow, periorbital, and midfacial rejuvenation. It blocks the discharge of presynaptic acetylcholine, thereby reducing muscle contraction. This prevents the activation of the postsynaptic myoneuronal unit, and thus muscular paralysis ensues. Food and Drug Administration for the treatment of facial getting older: Botox Cosmetic (onabotulinumtoxinA), Dysport (abobotulinumtoxinA), Myobloc (botulinum toxin type B; Solstice Neurosciences), and Xeomin (incobotuli- Chapter 20 � Cosmetic Uses of Botulinum Toxin 541 numtoxinA). Food and Drug Administration for the beauty correction of glabellar and lateral canthal strains, whereas Dysport and Xeomin have approval to be used in the glabellar area solely. Numerous "off-label" beauty uses of the merchandise are discussed later on this chapter. Dysport contains fewer associated hemagglutinin proteins than Botox, whereas Xeomin incorporates the entire hemagglutinin proteins which might be dissociated from the core neurotoxin through the manufacturing process, thus carrying a theoretically decrease threat for a hypersensitivity response at the injection web site and for the affected person growing tolerance to the product. Active bacterial or viral an infection at the injection website is a contraindication to the injection of neurotoxin. If a patient presents with concomitant warfarin or clopidogrel treatment, he or she should be knowledgeable in regards to the higher incidence of extended bruising related to injection when taking these medicine.
Order 0.5mg dostinex otcPassage of the trocar is tougher, as a outcome of it should be passed horizontally, and care have to be taken to shield the attention. When the stylet is faraway from the trocar, along with a single wire loop, as described with unilateral fixation, two extra single wires are also passed; these might be used to anchor nostril pads that shall be applied bilaterally. With a 16-gauge trocar, the wire loop and the 2 single wires can be handed from one aspect to the opposite through a single gap. For eyelid fixation, the sting of the upper and lower lids are connected with 4-0 Prolene sutures to wire loop already fashioned on one facet, and to a twisted loop of wire on the contralateral facet. The two single wires are left to protrude via the pores and skin incision, which is sutured closed across the wires. Several kinds of nostril pads are available for placement between the protruding wires on both canthus. These may be twisted to tighten the nostril pads and compress the inside canthal delicate tissue. After the wiring has been tightened, the skin sutures are left in place for 7 to 10 days. B, Trocar with stylet eliminated showing passage of a single wire loop, and two skin wires. C, Placement of nose pads over skin wires after the internal loop has been twisted tight. D, Closure of the canthal pores and skin incisions with the 2 pores and skin wires in place for fixation to nostril pads. Reconstruction of the lower canaliculus and higher canaliculus, in combination with eyelid reconstruction, can current postoperative epiphora with the necessity for secondary placement of a Jones tube. Intubation of the canalicular system or residual canaliculus with Crawford silicone tubes is essentially the most environment friendly technique for splinting the lacrimal system. The Crawford intubation set consists of silicone tubing with two bulb-tipped lacrimal probes wedged on both finish of the tube. Chapter 27 � Medial and Lateral Canthal Reconstruction 805 Technique the distal finish of the severed canaliculus is recognized. The tissue surrounding the canaliculus is undermined with sharp scissors to allow stretching of the canaliculus, and intubation of each canaliculi is then carried out. The lacrimal probes are passed through the upper and lower canaliculus and extracted from beneath the inferior turbinate with the utilization of a special hook. The lacrimal probes are then excised from the tubing, and the tubing is secured beneath the inferior turbinate. The tubing is fixated intranasally with a single square knot for ease of later extraction. B, Placement of silicone tubes in the residual canaliculus with reattachment of the lower lid. When a minimal of 70% of both the higher lid and decrease lid margins remains, each tarsal plate can be pulled laterally to shut the lateral canthal defect. Technique the residual higher lid is everted over a Desmarres retractor and a tarsoconjunctival flap is printed on the tarsal conjunctiva. It is essential to go away intact no much less than four mm of the higher lid tarsal margin to prevent instability of the margin. The lateral margin of the tarsal flap is then immediately sutured to the lateral canthus, if the periosteum of the lateral orbital rim is unbroken. If intact periosteum is current at the orbital rim, the lateral margin of the tarsal flap is then sutured directly to the canthal periosteum. E and F, Posterior lamella fixated to the lateral canthus and covered with a full-thickness skin graft. This easy flap makes use of excess ipsilateral upper eyelid skin to restore and proper scarring or defects at the lateral canthus. Skin transposition flaps at the lateral canthus are helpful to right this kind of epicanthus palpebralis. The transfer of the pores and skin flaps ought to always be accompanied by removing of subcutaneous scarring and adhesions and by subcutaneous debulking of the fold. Since most canthal defects additionally lengthen into the higher lid, the approaches are easily modified to encompass fixation and reinforcement of both the lower and upper lid. Chapter 27 � Medial and Lateral Canthal Reconstruction 811 suture FixatioN to the periosteum Fixation of the lateral edge of the tarsal plate to the periosteum on the lateral rim may be achieved with sutures. A small sturdy half-circle needle (P-2) is required for taking the periosteal chew inside the rim; 4-0 Prolene suture material supplies enough support and is nonreactive. Technique the periosteum of the lateral rim is uncovered as well as the sting of the temporalis fascia. To create flaps for the higher and lower eyelid, two parallel incisions are made 1. The periosteal flap is hinged at the inner fringe of the lateral rim and is raised and break up horizontally. The flaps are crossed to form an angle that can correspond to the lateral canthal angle. The remaining conjunctiva from the inferior and superior fornices is also mobilized to join the periosteal flaps. E, Configuration of an Enduragen patch and placement to reinforce eyelid attachment to the canthus. Chapter 27 � Medial and Lateral Canthal Reconstruction 813 drill holes In the absence of periosteum at the lateral rim, the edge of the eyelids should be fixated to the bone with sutures to achieve the desired rim place. Technique Two drill holes are made at the appropriate stage 3 mm contained in the rim; 4-0 Prolene sutures from the perimeters of the higher and decrease tarsal plates are crisscrossed by way of the holes to the outside of the rim and tied permanently. A new level of purchase for lateral fixation could be created with a miniplate spanning a bony defect. The plate is molded to the desired contour with the miniplate benders and placed into optimal position at the lateral orbital rim. Two holes are drilled above the frontozygomatic suture and two beneath the zygomatic arch. The lateral edges of the lid can then be refixated by the use of a everlasting suture. The suture is secured laterally to the miniplate on the correct degree for orientation of the lateral canthal angle. Elderly sufferers often require a less involved procedure and heal very properly with skin grafts. Reconstruction within the canthal areas is generally extra complicated than that within the lid areas. This is extra doubtless in the medial canthus than in the lateral canthus because of the coexistence of the lacrimal drainage system, and there will be more difficulty with bony fixation to produce a proper vector for the eyelid. Reconstruction of the lateral canthus, together with lateral canthoplasty and fixation of soft tissue, is mostly easier. Chapter 27 � Medial and Lateral Canthal Reconstruction 815 Optional methods for specific situations have been described which have served us well. We reemphasize that gentle tissue substitute in the eyelid proper can solely produce a functional eyelid when adequate fixation on the medial and lateral canthus is obtained.
Purchase dostinex from indiaThe anterior lamellar skin-muscle flaps can both be development or rotational flaps. These skin-muscle flaps should be backed with a posterior lamellar lining or graft to the posterior lamella for the higher lid. In many cases, conjunctiva from the upper lid fornix or an advancement flap of conjunctiva from the decrease lid can be utilized to complement the posterior lamellar lining. Free grafts of inflexible mucous membrane�lined tissue such as tarsoconjunctiva or palatal mucoperiosteum are perfect for this objective. A semicircular incision is made in the skin-muscle layer laterally and a flap developed and brought throughout the defect. A handy source of lining for the posterior lamella of the upper lid is conjunctiva (tarsoconjunctiva) from the lower lid. This supply of mucous membrane can be utilized to complement any of the other strategies of posterior lamellar replacement. B, Replacement of the anterior lamella of pores and skin with a rotational development flap. B, An upper blepharoplasty was performed, leaving the central half of the orbicularis for blood provide by deepithelialization and leaving the pores and skin on the distal blepharoplasty flap. The central half was preserved for blood provide and the distal half was folded inferiorly to reconstruct the lid margin. A flap of enough width ought to be ready to provide sufficient vertical width of the ensuing upper lid. Because some contraction occurs in the course of the postoperative period, vertical shortening is generally more of a problem than extreme length of the upper lid. The surrounding tissue and the bottom of the flap are undermined to permit the flap to rotate into the defect and to enable direct closure of the donor website. The vertical donor website incision is approximated with vertical mattress 4-0 Prolene or Monocryl mattress sutures in interrupted style; 6-0 nylon sutures are used for skin closure. The posterior lamellar free grafts generally will tackle a well-vascularized flap. The perfect lining of the flap, if out there, is conjunctiva from the decrease lid or fornix. B, Recruitment of posterior lamellar lining of the conjunctiva from the lower lid to be advanced upward. F, the patient is seen after repositioning of the base of the flap, showing the flap in position in the higher lid. Chapter 25 � Upper Eyelid Reconstruction 745 the brow flap is connected to the levator aponeurosis or remnants of the levator muscle with 6-0 silk mattress sutures to give the appropriate vertical mobility to the higher lid. Laterally, the tip of the flap is connected to the remnants of the lateral canthal tendon. The posterior lamellar lining graft is carefully rotated across the edge of the flap that varieties the brand new lid margin and sutured in place with operating 7-0 silk to make certain that mucous membrane quite than keratinized epithelium will keep up a correspondence with the cornea. If the undersurface of the forehead flap has been lined with a flap of conjunctiva from the lower lid, it can be separated in 2 weeks, leaving sufficient conjunctiva to cowl the lower margin of the brow flap, which becomes the new higher eyelid margin. After four to 6 weeks, the flap is separated from its base, and the base of the pedicle is repositioned into the donor (glabellar) space between the eyebrows. The lid may seem tight for many weeks earlier than the levator muscle begins to provide vertical mobility. The resultant eyelid skin is thicker than normal and could additionally be "thinned" with warning at a later date. The temporal brow flap supplies tissue for the upper lid and lateral canthal area and is suited for large defects in that space; however, it does introduce skin of a much greater thickness than is generally found in the upper lid area and should be reserved as a last-resort procedure. The flap is designed to be primarily based temporally and the base of the flap to angle as close as potential to the lateral canthus for good transposition. Undermining ought to be carried out temporally; nevertheless, one should keep in thoughts that the superficial branch of the temporal nerve supplying the forehead is in this area, and solely subcutaneous undermining ought to be carried out. The flap is then transposed into the higher lid or canthal defect, and the flap is anchored into position in the recipient higher lid defect. Closure of the unique website of the flap is performed with deep and cutaneous sutures. Care should be taken to attach the upper lid retractors to the flap to establish motion. A thicker flap pores and skin can provide sufficient upper lid movement but might produce a tethering impact on the lid. To right full-thickness defects of this kind, offset eyelid grafts can be utilized, usually of the full-thickness skin externally and mucous membrane for the posterior lamella. The higher lid is cut up and separated so that the two grafts are positioned at different ranges with each graft resting on its own vascular mattress to ensure survival. Because this system is normally employed with severely cicatrized upper lids, the grafts could undergo some contracture. Technique the vertically shortened upper lid is everted and a horizontal incision is made by way of the tarsal floor approximately 5 mm above the eyelid margin. The retractor is eliminated, the lid pulled downward with mattress sutures by way of the margin, and a horizontal skin incision is made across the higher lid above the superior fringe of the tarsal border with a scalpel. Sharp scissors are used to undermine the pores and skin superiorly and inferiorly, releasing any traction bands holding the eyelid within the retracted position. The lower edge of the pores and skin incision is then joined with the upper fringe of the tarsal incision. With the higher lid everted over a Desmarres retractor, a full-thickness buccal mucous membrane or chondromucosal graft is sutured into the posterior incisions between the cut edges of the tarsal conjunctiva with a steady 6-0 plain gut suture. An alternative methodology of suturing a mucous membrane graft in place on the undersurface of the lid is to use through-and-through mattress sutures which might be introduced through the lid and tied externally. With the lid retracted downward, a full-thickness skin graft is placed into the anterior incision with either interrupted or running 7-0 silk sutures. A momentary tarsorrhaphy is used for 1 week to maintain the lid on stretch to reduce retraction. In more extreme instances, there could additionally be lack of the anterior and posterior lamella of the upper and decrease lids. The priority is to shield the cornea from publicity and potential corneal ulceration. Commonly in burn patients, components of the posterior lamellar tarsoconjunctiva are nonetheless current. In more severe circumstances, inversion of residual conjunctiva could additionally be all that can be accomplished. In some circumstances of extreme systemic burns, only break up skin could be discovered, however it can be used to cowl Chapter 25 � Upper Eyelid Reconstruction 749 this space. If a flap can be utilized, an ear cartilage graft can be interposed between the flap and the closed conjunctival sac to type the idea of future eyelid construction for later procedures. With these extreme cases, there may be greater contracting forces, and the lids ought to remained fused longer, 2 to 3 months if attainable, to compensate for this drawback. The fused lids could be separated at that time to permit imaginative and prescient; however, normally revisional procedures are necessary for optimal results.
Syndromes - Persistent, watery diarrhea
- MRI scan of the heart
- Pulmonary function tests
- Calm and reassure the person.
- Pelvic or abdominal ultrasound
- Hearing loss that is new or getting worse
Order generic dostinex lineSphenooccipital chordomas produce signs related to compression or destruction of various adjacent buildings, such because the optic nerves or pituitary gland. Age-adjusted incidence charges and age-specific frequency, all races, both sexes, 650 instances. A, Anteroposterior radiograph of sacrum exhibits expansive lytic lesion of physique of sacrum. B, Lateral radiograph of lumbar backbone reveals uncommon sclerotic look of physique of L4 produced by vertebral chordoma. Lateral view of cranium shows destruction of sella turcica area of base produced by sphenooccipital chordoma (arrow). T2-weighted magnetic resonance picture of chordoma at base of cranium reveals excessive signal intensity mass in area of sphenoid bone (arrows). Vertebral chordomas produce lytic lesions that will involve two or extra adjoining vertebral bodies. Computed tomography and magnetic resonance imaging are indispensable in evaluating both the extent of the lesion and the involvement of adjacent constructions. They are incessantly myxoid or gelatinous in look and may mimic chondrosarcoma or mucinous adenocarcinoma. Despite good demarcation, the tumor usually extends beyond its grossly recognizable borders. Chordomas often contain the medullary canal, compressing the spinal twine and its nerves. The level of cellularity can range considerably amongst cases and in numerous areas of the identical tumor. In basic, most chordomas exhibit clearly recognizable nuclear pleomorphism with occasional giant atypical cells. Occasionally, the vacuoles encircle the nucleus, which stays centered in the cytoplasm and produces the so-called physaliphorous look. The traditional large physaliphorous cell has a centrally located nucleus surrounded by a slender rim of cytoplasm that in flip, is encircled by a hoop of more peripherally situated cytoplasmic vacuoles. Such lesions are descriptively referred to as lipoma-like chordomas and could additionally be confused with benign or malignant lipomatous tumors. On the opposite hand, extremely mobile lesions with minimal vacuolization and dense eosinophilic cytoplasm could mimic epithelial neoplasms. Areas of cartilage can range from small microscopic foci to large distinguished areas. Therefore chordomas may be occasionally tough to distinguish from chondrosarcoma. The time period chondroid chordoma has been proposed to designate hybrid lesions that exhibit features of each lesions-chordoma and chondrosarcoma. The controversy over this entity and its potential for scientific significance are discussed separately. The presence of irregular multivacuolated cytoplasm with centrally positioned, scalloped nucleus (that is, physaliphorous cells) is the hallmark of chordoma. Such classical cells are, nevertheless, uncommon; in the vast majority, the cells show dense eosinophilic cytoplasm or are lipoblast-like with single or several bigger cytoplasmic vacuoles displacing the nucleus peripherally. Cytologic features combined with radiologic and medical presentation allow right cytologic prognosis generally of chordoma. The immunohistochemical features such as coexpression of epithelial markers and S-100 protein could be additionally examined in cytologic preparations. Chordoma cells include intermediate filaments and are linked by desmosome-like junctions. The extracellular matrix consists of a fantastic, granular substance of low electron density. A, Computed tomography reveals lobulated mass protruding posteriorly and anteriorly from origin in sacrococcygeal junction. B, T1-weighted sagittal magnetic resonance picture of chordoma shown in A with bigger posterior and anterior low sign mass (arrows). Lateral radiograph of cervical spine exhibits damaging lesion of body of C2 (arrows). In common chordoma recapitulate a gene expression signature of notochordal cells. Among all the markers, brachyury appears to be essentially the most specific for chordoma and notochordal tissue and is useful in the differential prognosis. The commonest cytogenetic abnormality is hypodiploidy with loss of the short arm of chromosome three, and lack of proximal 1p as properly as monosomy of chromosome 10. Chordomas are also characterized by frequent positive aspects of genetic material on 5q, 7q, 12q, and 20q. The cytogenetic data suggests that tumor suppressor genes on 1p and 3q as nicely as oncogenes mapping to 5q, 7q, 12q, and 20q may play a role in the growth of those tumors. The presence of physaliphorous cells and a trabecular or cordlike arrangement along with a myxoid matrix are typical for chordoma. However, typical chondrosarcoma sometimes might present a cordlike arrangement of cells and myxoid stroma. In such situations, positivity for S-100 protein and adverse staining for epithelial markers favor chondrosarcoma. Other myxoid bone tumors, corresponding to chondromyxoid fibroma, which rarely happens within the axial skeleton, are very unlikely to be confused with chordoma. Highly mobile areas with cohesive solid cellular sheets and distinguished nuclear atypia can be confused, especially in a restricted biopsy specimen, with an epithelial neoplasm. Extensive clear-cell change and the signet-ring appearance of chordoma cells can result in a misdiagnosis of metastatic adenocarcinoma or much less frequently lipomatous tumor. Among numerous epithelial tumors metastatic to the skeleton a chromophobe variant of renal cell carcinoma could superficially resemble a chordoma. Strict adherence to medical and radiographic data usually helps to avoid this error. A, Axial computed tomography shows destructive mass protruding posteriorly and anteriorly from the sacrum (arrows). B, T1-weighted sagittal magnetic resonance picture of chordoma proven in A with predominantly anterior low signal mass (arrows). C, Sagitally minimize resection specimen of the tumor proven in A and B demonstrates a lobulated, fleshy tumor mass destroying the sacrum and lengthening to the delicate tissue anteriorly and posteriorly. D, Histologic section of same tumor reveals cords of chordoma cells with multivesicular cytoplasm growing in a myxoid stroma. A, Resection specimen of sacral chordoma displaying a gelatinous tumor growing anteriorly from the coccyx. C, Gross photograph of a bisected lumbar (L5) vertebral resection specimen displaying a gelatinous tumor mass changing nearly the entire vertebral physique. D, Specimen radiograph of tumor shown in C displaying damaging lesion replacing the vertebral body. A, Bisected tumor from sacral region reveals tan-gray soft tissue with myxoid appearance.
Cheap dostinex 0.25 mg mastercardB, In these instances, the trochar is always handed from the unaffected side by way of a small osteotomy. C, this supplies a neater vector for positioning the wire loop on the affected facet. The tissue in the area of the medial canthal tendon is sutured to the wire on the looped facet with 4-0 nonabsorbable suture such as Prolene. To repair the wire, a steel bolster pin is common by slicing an eight mm length from the central portion of the stylet of a 19-gauge angiocath. The pin is bent barely within the center and held in opposition to the lateral nasal bone on the conventional aspect with a vertical orientation and resting between the ends of the wire. The wire ends are twisted over the pin, anchoring it in opposition to the bone and providing glorious purchase for additional tightening of the wire. The wire loop is tightened by simultaneously pulling on the ends of the wires and twisting them over the pin until the telecanthus is slightly overcorrected. After the transnasal wiring is completed, however before the ultimate 1102 Part V � Orbital and Lacrimal Surgery pores and skin closure, the tags are eliminated and the loop of wire is minimize leaving two exterior wires exiting each pores and skin incision. These can lead to a continual, long-lasting, and disfiguring appearance in sufferers who had wonderful acute remedy. Changes happen in the intraorbital contents, which embrace fats atrophy with lack of intraorbital quantity and enophthalmos. Small modifications in the quantity of the orbit typically increase the dimensions of the orbital socket due to bone resorption. This contributes to a deep sulcus syndrome, with a depressed cheek and enophthamos that can be documented by a Hertel exophthalmometry measurement of more than 5 mm in an in any other case regular sighted eye. These sufferers appear to have a synthetic eye and are often requested by others whether or not they have a "glass eye. For patients with an acute unilateral or bilateral nasoorbitoethmoid fracture, surgeons must be proficient in transnasal wiring to stop the development of posttraumatic telecanthus. For sufferers with continual telecanthus, repeat unilateral or bilateral transnasal wiring can be carried out; nonetheless, newer, less invasive methods can be found, corresponding to the usage of a Mitek anchor to strengthen the medial canthal tendon. Recurrent orbital cyst as a late complication of silastic implant for orbital flooring fracture repair. Reconstruction of orbital ground fractures using autologous nasal septal bone graft. Late-onset orbital hematoma secondary to alloplastic orbital implant mimicking transient ischemic attacks. Epithelial inclusion cyst associated with a porous polyethylene orbital flooring implant. Respiratory epithelial ingrowth and hemorrhage as late complications of orbital flooring fracture restore with silicone sheet implant. Treatment with individual orbital wall implants in humans- 1-year ophthalmologic evaluation. Late correction of orbital-zygomatic-maxillary fractures mixed with orbital wall fractures. Rounding of the inferior rectus muscle as a predictor of enophthalmos in orbital ground fractures. Endoscopic transmaxillary repair of orbital floor fractures: a minimally invasive remedy. Clinical implications of orbital quantity change in the administration of isolated and zygomaticomaxillary complex-associated orbital floor injuries. Orbital cysts lined with each stratified squamous and columnar epithelia: a late complication of silicone implants. Although the scope of this subject is broad, with full textbooks devoted to the topic, a complete evaluation is offered here. Distal obstruction may be within the lacrimal sac or on the nasolacrimal duct opening under the inferior turbinate. Irrigation of a practical obstruction may be accomplished, with a mixture of antibiotic and steroid eyedrops into the lacrimal system with outflow in the nose, adopted by conservative management. Ideally, the basal tear secretion rate equals the speed of tear drainage and evaporation. Excessive tearing results from a disruption within the balance between tear manufacturing and tear loss. Tears enter the puncta, and about 90% are reabsorbed via the nasolacrimal duct mucosa, whereas 10% drain into the floor of the nasal cavity. Tears evaporate from the ocular floor at a variable price, but ideally tear evaporation roughly equals the distinction between basal secretion and drainage. The intimate relationship of eyelid place and movement is of great significance to maintaining an sufficient tear film. Disruption following eyelid surgery can produce disturbances starting from dry-eye syndrome to annoying epiphora, or watering of the eyes. The clean, moist floor of the cornea is the main refractive surface of the visible system, which, together with corneal transparency, enables light to pass by way of the lens and onto the retina, the place photoreceptors are activated. However, the presence of the sleek, moist refractive ocular floor required for vision comes at a value. Thus numerous protecting mechanisms are supplied to ensure imaginative and prescient by the ocular floor system, which is defined because the ocular surface, together with the floor and glandular epithelia of the cornea, conjunctiva, lacrimal glands, accessory lacrimal glands, and meibomian glands. Maintenance and safety of the smooth, refractive floor of the cornea is the operate of the ocular surface system. In addition, the ocular surface system contains the apical (tears) and basal (connective tissue) matrices, the eyelashes with their related glands of Moll and Zeis, the elements of the eyelids answerable for the blink, and the nasolacrimal duct. The tear film is structurally complicated, with three distinct layers: (1) the outermost layer: a surface of lipid/superficial lipid that contains oils and offers a coating to the inside layers, which comprise water. Since the exterior floor of the cornea is primarily avascular, the tear film keeps the cornea moist, which prevents ulceration of the cornea. The lipid layer serves to scale back lack of underlying aqueous tears within the open eye by sealing the tear movie and stopping evaporation. The oil is derived from fats exuded from meibomian gland openings along the eyelid margin. The sebaceous glands embody the glands of Zeiss and Moll and the meibomian glands. The superficial lipid layer of the tear movie is derived from the meibomian glands, which are embedded inside the eyelids. Meibomian gland dysfunction causes abnormalities within the secreted lipids and dry-eye signs might result from elevated evaporation of tears. Blocked or poorly functioning meibomian glands trigger problems with the lipid layer. Production of the parts of tear film come from: � the tarsal (meibomian) glands; there are about 25 in the upper tarsus and 20 within the decrease tarsus � the glands of Zeis on the palpebral margin of each eyelid � the glands of Moll, found at the roots of the eyelashes the oil secretors type the outer layer of the precorneal movie, most essential of which are the tarsal glands. Absence of the oil layer permits the precorneal movie to lower in thickness and quickly "run off of the cornea," and the evaporation rate is 10 to 20 instances quicker than normal. During waking hours, the lacrimal glands pump aqueous tears at a background level adjusting for environmental situations; that is known as basal secretor production. In addition to the main lacrimal glands, the following exocrine glands are within the subconjunctival tissue, and all together form the intermediate aqueous layer of the precorneal movie: � the accent lacrimal glands of Krause, about forty of which are in or in regards to the upper conjunctival fornix and about 6 within the lower fornix.
Purchase 0.25 mg dostinex with visaChapter 1 � Periorbital and Eyelid Anatomy 9 skin-MusClE layEr the eyelids could be divided into the anterior and posterior lamellae layers. A distinct transition exists between the thin eyelid pores and skin, which has a skinny dermis and lacks subcutaneous fat, and the thicker cheek pores and skin, which has a well-defined dermal layer and subcutaneous fats. The tarsoligamentous sling that supports the connective components contains the posterior lamella, which is made up of the tarsal plates of the higher and lower eyelids and the connecting periosteal attachments known as the canthal tendons. The tarsal plate should be considered the skeleton of the eyelids, so its restore throughout eyelid reconstruction is crucial. The orbicularis muscle is densely fixed to the whole anterior floor of the tarsal plate of the upper and lower lids. Posteriorly, the tarsal plates are lined by a tightly adherent conjunctiva that continues on the eyelid margin to the mucocutaneous junction. In kids, the tarsal plates and the canthal tendons maintain the eyelids firmly in opposition to the attention. With aging, the tendons and the tarsus might stretch, which allows the eyelids to be mechanically distracted from the globe by a quantity of millimeters. Scarring in the center lamella area probably entails scarring of the orbital septum and the orbital fats. The ordinary maximal height is about 10 mm, as measured centrally in the higher eyelid. The vertical top of the lower eyelid tarsus was measured in 20 sufferers who had been to undergo decrease eyelid resections and in 17 cadavers; the tarsal heights were discovered to be 3. The upper and decrease tarsus ought to be clearly recognized throughout procedures that involve eyelid restore or reconstruction so that tension-bearing sutures could be positioned via the tarsus. Medially and laterally, the tarsal plates have fibrous connections to the orbital rims; these are historically known as the canthal tendons. B, the tarsal plates and the canthal tendons are the support structures of the eyelid. B, the anterior reflection offers off a vertical extension anterior to the lacrimal sac fossa, whereas the posterior reflection extends and inserts in the space of the posterior lacrimal crest and the medial retinaculum. The anterior reflection of the lateral canthal tendon inserts on the anterior floor of the lateral orbital rim because the lateral orbital raphe. The lateral canthal tendon arises as a fibrous attachment from the lateral ends of the tarsal plates. It is identifiable as a broad band of connective tissue that extends from the lateral end of the tarsal plate to the lateral orbital tubercle. Laterally, the lateral canthal tendon passes deep to the septum and inserts posterior to the orbital rim. Superiorly, the lateral canthal tendon is contiguous with the lateral horn of the levator aponeurosis and the lateral retinaculum. The posterior side of the tendon is contiguous with the check ligament of the lateral rectus muscle, which is posterior to the tendon at its insertion into the orbital tubercle and the lateral canthus. Fibrous connections between the tendon and the verify ligament of the lateral rectus muscle recommend a useful relationship between the two. A lateral displacement of the canthal angle generally occurs in lateral gaze and involves a median of two mm of displacement with extreme abduction of the globe. These findings recommend that the tendon not solely supplies structural fixation of the lids to the lateral canthus but additionally imparts mobility to the canthal angle by its posterior fibrous attachments to the verify ligament of the lateral rectus muscle. Reconstructive surgical procedure of the lateral canthus is regularly required for the therapy of traumatic damage, tumor resection, and correction of eyelid malposition.
[newline]Surgical methods that present fixation of the lateral canthus to the inside side of the orbital rim will reproduce the normal positioning and pull of the lids in opposition to the globe. Attachment of the lid to the sting or anterior floor of the orbital rim must be averted, as a outcome of this can pull the lid away from the globe. B, the canthal tendon has a posterior vector; the orbicularis inserts on the lateral orbital rim with an anterior vector. At the lateral canthus, the preseptal and orbital orbicularis fibers pass uninterrupted anterior to the orbital rim, the place the superficial muscle attaches to the zygoma along a horizontal lateral palpebral raphe. Its attachment to the sting of the orbital rim is called the arcus marginalis, and it at that point turns into a thickening of the periosteum. The orbital septum forms the anterior barrier of the orbital contents, and it confines the orbital fats and different orbital structures. The inferior portion of the orbital septum extends medially to the anterior lacrimal crest. The lacrimal drainage apparatus travels within the house between the superior and inferior insertions of the septum. At the lateral canthus, the orbital septum is posterior to the superficial orbicularis and joins the lateral canthal tendon, and a posterior sheath of septum inserts at the lateral orbital tubercle. In the lower eyelid, the septum inserts on the inferior tarsus after joining with the lower eyelid retractors 4 to 5 mm beneath this structure. The junction of the septum and the levator aponeurosis in the higher eyelid varies by intercourse and race, which must be appreciated earlier than surgical procedure. In males, the levator septal insertion to the dermis usually varieties the higher lid crease at eight mm above the lid margin. In ladies, the upper lid crease is more generally 10 mm above the higher Chapter 1 � Periorbital and Eyelid Anatomy 15 lid margin. The Asian higher lid crease may be as little as four to 5 mm above the lid margin; alternatively, it might not exist at all, because the junction of the levator aponeurosis and the septum fuses at the lid margin, which allows preaponeurotic fats to lengthen to the pretarsal area. The lateral septum is thicker, and it creates a stronger separation between the intraorbital contents and the eyelids. The ensuing hematoma was decided to be the results of intraorbital bleeding as opposed to eyelid bleeding because of the demarcation line of the orbital septum. In whites, the orbital septum inserts above the superior border of the tarsus into the levator aponeurosis. In Asians, the orbital septum inserts extra inferiorly on the levator aponeurosis over the tarsus, which permits the anterior orbital fats to extend to the anterior tarsal house; the inferior extension of the orbital fats prevents the levator aponeurosis fibers from fanning out into the subcutaneous tissue to kind the eyelid crease. Appreciation of the anatomy of the septum is essential, notably when surgical procedures may involve septal manipulation. It overlies the connective tissue parts: the orbital septum and the tarsoligamentous sling. It serves because the closure muscle (protractor) for the eyelids, and it also offers tone animation to the eyelids. The orbital portion extends from the eyelids into the brow, the temple, and the cheek. Medially, the pretarsal orbicularis divides into two heads that pass superficial and deep to the canaliculi. The anterior pretarsal orbicularis head types the anterior crus of the medial canthal tendon that inserts into the frontal strategy of the maxillary bone. Laterally, the preseptal muscle types the lateral horizontal raphe; medially, it inserts into the anterior crus of the anterior medial canthal ligament. The orbital fibers also insert on the anterior medial canthal ligament, the orbital rim, and the nasal part of the frontal bone.
Order dostinex 0.25mg without prescriptionThe traditional blepharoplasty publicity can be used first, and if the fat is anterior to the orbicularis, an incision by way of the posterior floor of the orbicularis will allow the subcutaneous fat to prolapse posteriorly. His left eye subsequently underwent spacer implant within the lower lid to even the fissure shape in his left eye. C, Intraoperative picture of the identical patient displaying that the fats was primarily subcutaneous. An incision was made horizontally via the orbicularis muscle, and with digital strain the fat herniated into the submuscular aircraft where it was removed. The contour abnormalities could additionally be partly caused by deficiencies in tone, that are magnified by the anomalous contours caused by the fats deposits. Previous makes an attempt had been made to remove the fat via transcutaneous incisions. B, One week after surgical procedure, the affected person confirmed enchancment after a skin-muscle blepharoplasty and redraping of the skin-muscle flap. Chapter 21 � Fat Grafting and Complications within the Periorbital Region 585 intramuscular dePosits (usually accomPanying multiPlanar) Despite the most effective intentions of many surgeons, intramuscular micro fat injections not solely can undergo augmentation with weight achieve, but because of the situation throughout the muscle, present an virtually impossible downside of extraction. The undesirable presence of fats augmentation over time or after weight acquire may be remedied surgically or reversed, if the anomalous fat is accessible in a subcutaneous or submuscular aircraft. With the model new recognition of well-defined fats compartments within the midfacial space, the surgeon ought to place micro fats injections within the anatomic planes or compartments in the face. In this fashion, any irregular modifications in the fats, corresponding to augmentation, are extra simply corrected. B, the patient is proven after fats injection; she historically described a weight achieve during that interval. C, Her surgeon tried to take away the fats with liposuction, which left a sunken, deformed face. E, the affected person required a decrease blepharoplasty and midface lift by one other surgeon. F, the affected person is proven 2 years later with permanent changes to her face, which started with fat grafting. The recognition of fats grafting as an adjuvant to facial procedures has elevated in the past several years. A clear understanding of the growing older course of for each individual patient, as nicely as normal anatomy, is critical to obtain profitable fat grafting. The most profitable techniques use meticulous injection techniques to keep away from probably serious and generally everlasting issues. Autologous fats grafting can offer longer-term outcomes than artificial injectables, is available, and is extremely method dependent. Syringe aspiration and fats focus: a simple method for autologous fats injection. Middle cerebral artery embolism and unilateral visible loss after autologous fats injection into the glabellar space. Advanced rejuvenative upper blepharoplasty: enhancing aesthetics of the higher periorbita. Autologous fats transfer national consensus survey: tendencies in strategies for harvest, preparation, and utility, and perception of short- and-long time period outcomes. Chapter 21 � Fat Grafting and Complications in the Periorbital Region 587 Kranendonk S, Obagi S. Autologous fats switch for periorbital rejuvenation: indications, technique, and issues. Osteoplasty flap approach for repair of latent (30-year) post-traumatic frontal sinus mucocele: case report and review of the literature. Although this is a localized anatomic downside, its analysis and treatment are complicated due to the big selection of circumstances that cause ptosis, the variety of procedures needed to correct its totally different manifestations, and the crucial nature of higher eyelid function and its impact on ocular well being. Even when the prognosis is obvious, many variables have to be weighed before a surgical answer could be devised. Indications for particular surgical procedures are described intimately, as are the surgical steps for executing them. We begin by contemplating the initial workup of a ptosis patient and the necessary thing inquiries to be addressed for correct evaluation. This is adopted by a comprehensive part on the decision-making process, which features a collection of algorithms that function a road map for choosing the most effective surgical procedures for several sorts of ptosis. The objective is to present a rationale for problem-solving and supply a greater perspective on why certain ptosis procedures are utilized in particular medical conditions. The remainder of the chapter focuses on specific strategies for treating "normal" ptosis issues in addition to uncommon or complicated types of ptosis. Patient Evaluation: Seven Questions to Consider When contemplating surgical correction of ptosis, the surgeon should address seven basic questions; the answers provide the key to ptosis evaluation and surgical planning. It is necessary to distinguish between congenital and acquired forms of ptosis, as a outcome of the levator muscle exhibits distinct anatomic differences for each kind, and its response to repair procedures differs as well. B, Levator anatomy in a patient with congenital ptosis showing the similar old poor differentiation of anatomy. In most cases of congenital ptosis, the levator muscle is underdeveloped and stiff, with poorly outlined anatomic structures; lagophthalmos is present in downgaze. B, Downgaze reveals lagophthalmos in the eye with ptosis as a end result of stiffness in the fibrotic levator muscle. C, An old photograph of the patient confirms that left ptosis was present at a a lot earlier age and is congenital. It is important to decide the amount of levator operate when selecting the most effective surgical procedure for elevating the upper lid. Therefore levator function should be measured in all patients; only then can the surgeon determine whether or not a ptosis repair on the levator muscle is indicated or whether or not a frontalis suspension process must be used. To measure levator function, the forehead have to be immobilized to get hold of a real reading of levator perform aside from brow exercise. The patient is then asked to look up while the forehead is immobilized, and the new place of the lid edge on the size will allow measurement of levator operate. A lid that moves 12 mm or more from downward gaze to upward gaze is considered regular. B, Lid in upgaze, the scale confirming the quantity of levator excursion of 12 mm, indicating good levator function. Levator dehiscence is acquired and normally occurs in older adults however may happen in youngsters following swelling or trauma. The commonest reason for aponeurotic dehiscence is involutional or idiopathic; nevertheless, dehiscence can occur from trauma, unusual eyelid swelling, long-term use of onerous contact lenses, cataract surgery from the refractor force, or any ocular surgical procedure. Proper correction of ptosis in this scenario is repair of the levator dehiscence with superior advancement of the tarsus. She had a cataract extraction in the left eye and reveals the changes of levator dehiscence generally seen after cataract surgical procedure.
Order 0.5mg dostinex visaIt capabilities to convert the anterior posterior pulling drive of the levator muscle to a superior path, which raises the eyelid. Laterally, the ligament joins with the pseudocapsule of the lacrimal gland and the frontal bone. Whitnall initially described the operate of this structure as a verify ligament of the levator, as a outcome of it limited the posterior pull of the muscle in the cadaver and because its location is analogous to the examine ligaments of the opposite extraocular muscular tissues. Larger levator resections are essential for elevations of the eyelid during ptosis surgical procedure if the ligament is cut. Dividing this strand during ptosis surgical procedure will cut back lagophthalmos in the lid postoperatively. Approximately eight to 10 mm below the point at which the superior transverse ligament crosses the levator muscle, a transition in the levator happens: it adjustments from a fleshy-appearing extraocular muscle right into a white fibrous aponeurotic sheath. Whitnall initially described the sheath as having a size of 7 mm from the musculoaponeurotic junction to the superior tarsal border; however, this may differ from individual to particular person. Anteriorly, the levator aponeurosis fuses with the orbital septum above the superior border of the tarsus and sends fibrous strands between the orbicularis oculi muscle septa to the pores and skin to type a supratarsal eyelid crease 8 to 10 mm above the margin. The levator aponeurosis inserts an additional 7 to eight mm onto the anterior floor of the tarsus. These insertions, which are referred to as the medial and lateral horns of the levator, also serve as verify ligaments to restrain the retraction of the higher lid. The horns may be loosened or divided throughout levator resection surgical procedure to allow the levator muscle to stretch adequately throughout ptosis procedures. The lateral horn is a strong, fibrous band that incompletely divides the lacrimal gland into two lobes: the orbital lobe and the palpebral lobe. It then continues inferiorly to insert on the lateral orbital tubercle behind the lateral canthal tendon. By contrast, the medial horn turns into thin because it passes over the mirrored superior indirect tendon to reach its insertion behind the posterior lacrimal crest. Appreciation of the anatomy of the levator is important in medical conditions that contain ptosis repair. In adult patients with acquired ptosis, the standard cause of this situation is the rarefaction or dehiscence of the aponeurosis. In sufferers with congenital ptosis cases, a dystrophy of the muscular portion of the levator with poor differentiation is the most common cause. C, Sagittal view of the insertion of the levator aponeurosis on the skin of the upper lid and the anterior floor of the tarsus. It originates from the undersurface of the levator muscle at the terminal striated muscle fibers of the levator palpebrae superioris. It arises from the underside of the striated levator muscle about 8 to 10 mm above the superior tarsal border. It is firmly hooked up to the levator only at its origin, and it may easily be separated from the latter under. The interruption of sympathetic innervation from the superior cervical ganglion ends in a lack of tone and normally 2 mm of blepharoptosis, which is seen in patients with Horner syndrome as the cause of ptosis within the classic scientific triad of ptosis, miosis, and anhidrosis. Treatment of this condition typically requires excision or detachment throughout levator aponeurosis recession for the correction of lid retraction. The capsulopalpebral head splits around and fuses with the sheath of the inferior indirect muscle. This is more evident within the young affected person; it happens 2 to three mm under the lid margin and 5 to 6 mm laterally. In the higher lid, there are typically thought of to be two extensions of fats or "fat pads. It is bordered posteriorly by the levator aponeurosis, medially by the trochlea, and temporally by the orbital lobe of the lacrimal Chapter 1 � Periorbital and Eyelid Anatomy 25 gland. The nasal fat pad can be easily identified during blepharoplasty by inserting mild pressure on the globe and opening the nasal septum just lateral to the branch of the medial palpebral artery. Between the nasal fats pad and the preaponeurotic pad is another small however distinct accumulation of fat that appears to be separate from the nasal fats pad and loosely related to the preaponeurotic pad: the transitional fat. The trochlear and supraorbital branches of the superior ophthalmic vein lie beneath it. Bleeding from this vein ought to be cauterized with direct visualization, as a outcome of deep, blind electrocautery can harm the trochlea and cause double imaginative and prescient. The nasal fat pad is partially separated from the central fat pad by the inferior indirect muscle. B, A extra detailed view of the fats compartments within the upper lid, together with the interpad septum and the transitional fats. It is superior to the lateral horn of the levator aponeurosis, nevertheless it sends secretory ducts around the aponeurosis to the palpebral lobe of the lacrimal gland beneath the aponeurosis. The orbital lobe is positioned within the fossa glandulae lacrimalis, a shallow fossa within the frontal bone at the superolateral orbit. The smaller palpebral lobe is connected to the orbital lobe by an isthmus posterior to the lateral horn of the levator muscle. Studies have shown that a lateral extension of the central preaponeurotic fats pad also extends to the lateral upper compartment in 15% to 20% of patients. This extension is anterior to the orbital lobe of the lacrimal gland, and it can be easily dissected away from the gland. Fullness within the lateral facet of the higher eyelid may end up from the release of the ligaments causing ptosis of the lacrimal gland. This layer is quickly appreciated with suborbicularis dissection under the infraorbital rim. Anterior to the orbicularis muscle layer is the malar fats pad, which is a triangular structure that offers fullness to the midface space. Aging-related adjustments of the midface are the results of complicated changes within the subcutaneous and bony volumes in addition to descent related to time. During upper lid surgical procedure, the looks of postseptal fats indicators that the surgeon has entered the preaponeurotic space. In some circumstances, extension and the appearance of the forehead fats in this space of the lid can confuse the surgeon. The brow fat is all the time anterior to the septum and should subsequently not be confused with postseptal fats. E, the malar fat pad is proven in its place anterior to the orbicularis muscle in the subcutaneous aircraft. B and C, Sagittal views of the first midface periosteal attachments, the orbitomalar ligament emanating from the inferior orbital rim and inserting in the orbicularis, and the dermis. The zygomaticocutaneous ligament originating over the malar space near the zygomaticofacial foramen and the origin of the zygomaticus muscle are proven. The cross-section of the periorbital anatomy illustrates the fats compartments as well as the orbitomalar ligament, the prezygomatic space, and the subzygomatic area.
References - Zeleke BM, Bell RJ, Billah B, et al: Hypoactive sexual desire dysfunction in community-dwelling older women, Menopause 24(4):391n399, 2016.
- Moran CA, Suster S: Primary mediastinal choriocarcinomas: a clinicopathologic and immunohistochemical study of eight cases, Am J Surg Pathol 21:1007n1012, 1997. Moran CA, Suster S: Primary germ cell tumors of the mediastinum: I. Analysis of 322 cases with special emphasis on teratomatous lesions and a proposal for histopathologic classification and clinical staging, Cancer 80:681n690, 1997. Moran CA, Suster S: Germ-cell tumors of the mediastinum, Adv Anat Pathol 5:1n15, 1998.
- Nesbitt LTJ: Glucocorticosteroids. In Bolognia JL, Jorizzo JL, Rapini RP, editors: Dermatology, vol 2, Edinburgh, 2003, Mosby, pp 1979n1989.
|
|