"Purchase reminyl 8 mg with visa, treatment impetigo."By: Keira A Cohen, M.D. - Co-Director, The Johns Hopkins Center for Nontuberculous Mycobacteria and Bronchiectasis
- Assistant Professor of Medicine
 https://www.hopkinsmedicine.org/profiles/results/directory/profile/10003818/keira-cohen
Reminyl 8mg on-lineEven although these muscles are extremely small, their tonic contraction is believed to cause retro-orbital headache. Also, extreme makes an attempt to focus the eyes can result in reflex spasm in varied facial and extraocular muscle tissue, which is a possible explanation for headache. A second sort of headache that originates in the eyes happens when the eyes are exposed to extreme irradiation by light rays, especially ultraviolet gentle. Looking at the sun or the arc of an arc welder for even a few seconds could result in headache that lasts from 24 to 48 hours. The headache generally results from "actinic" irritation of the conjunctivae, and the ache is referred to the floor of the head or retro-orbitally. However, focusing intense light from an arc or the solar on the retina also can burn the retina, which could possibly be the cause of the headache. Thermal gradations are discriminated by a minimal of three forms of sensory receptors-cold receptors, warmth receptors, and ache receptors. The ache receptors are stimulated solely by excessive levels of heat or cold and are responsible, along with the chilly and heat receptors, for "freezing cold" and "burning hot" sensations. The chilly and warmth receptors are positioned immediately under the skin at discrete separated spots. Most areas of the physique have three to 10 times as many cold spots as warmth spots; the quantity in different areas of the body varies from 15 to 25 cold spots/cm2 within the lips to 3 to 5 chilly spots/cm2 within the finger to less than 1 chilly spot/cm2 in some broad floor areas of the trunk. Warmth receptors are believed to be free nerve endings as a outcome of warmth indicators are transmitted mainly over unmyelinated sort C nerve fibers at transmission velocities of only zero. It is a special, small, type A myelinated nerve ending that branches several times, the ideas of which protrude into the underside surfaces of basal epidermal cells. Signals are transmitted from these receptors through thinly myelinated kind A nerve fibers at velocities of about 20 m/ sec. Some chilly sensations are believed to be transmitted in sort C nerve fibers as nicely, which suggests that some free nerve endings additionally might function as chilly receptors. Stimulation of Thermal Receptors-Sensations of Cold, Cool, Indifferent, Warm, and Hot. Note especially that these fibers respond differently at completely different levels of temperature. As the temperature rises to +10�C to 15�C, the cold-pain impulses cease, but the chilly receptors start to be stimulated, reaching peak stimulation at about 24�C and fading out barely above 40�C. Above about 30�C, the warmth receptors start to be stimulated, however these additionally fade out at about 49�C. Finally, at round 45�C, the heat pain fibers begin to be stimulated by warmth and, paradoxically, a number of the cold fibers begin to be stimulated once more, possibly due to harm to the chilly endings brought on by the extreme warmth. One can also perceive why extreme degrees of each cold and warmth can be painful and why each these sensations, when intense sufficient, might give virtually the same high quality of sensation-that is, freezing cold and burning sizzling sensations feel almost alike. Pain, Headache, and Thermal Sensations Stimulatory Effects of Rising and Falling Temperature-Adaptation of Thermal Receptors. When a chilly receptor is suddenly subjected to an abrupt fall in temperature, it turns into strongly stimulated at first, but this stimulation fades quickly through the first few seconds and progressively extra slowly during the subsequent half-hour or more. This implies that when the temperature of the skin is actively falling, an individual feels a lot colder than when the temperature remains cold at the same level. Conversely, if the temperature is actively rising, the individual feels a lot warmer than she or he would at the same temperature if it had been fixed. The response to adjustments in temperature explains the extreme degree of heat one feels on first entering a tub of sizzling water and the intense diploma of chilly felt on going from a heated room to outdoor on a chilly day. A few thermal alerts are additionally relayed to the cerebral somatic sensory cortex from the ventrobasal complicated. Occasionally, a neuron in cortical somatic sensory area I has been found by microelectrode research to be instantly conscious of both chilly or heat stimuli on a selected area of the skin. In different words, thermal detection probably results not from direct physical effects of heat or chilly on the nerve endings but from chemical stimulation of the endings as modified by temperature. However, when a large pores and skin area is stimulated suddenly, the thermal alerts from the complete space are cumulative. A temporary review of those bodily ideas is offered in this chapter, followed by discussion of the optics of the eye. Light rays ratio of the 2 refractive indices of the two clear media; and (2) the diploma of angulation between the interface and the getting into wave front. The light rays passing through the center of the lens strike the lens exactly perpendicular to the lens surface and, due to this fact, cross through the lens without being refracted. Toward both fringe of the lens, nevertheless, the light rays strike a progressively extra angulated interface. The outer rays bend increasingly more toward the middle, which is called convergence of journey through air at a velocity of about 300,000 km/sec, however they journey much slower through clear solids and liquids. The refractive index of a transparent substance is the ratio of the velocity of sunshine in air to the speed within the substance. Thus, if mild travels via a particular type of glass at a velocity of 200,000 km/sec, the refractive index of this glass is 300,000 divided by 200,000, or 1. Refraction of Light Rays at an Interface Between Two Media With Different Refractive Indices. The only impact that occurs is decreased velocity of transmission and shorter wavelength, as shown in the determine by the shorter distances between wave fronts. In this figure, the light rays are leaving air, which has a refractive index of 1. When the beam first strikes the angulated interface, the lower edge of the beam enters the glass forward of the higher edge. The wave entrance in the upper portion of the beam continues to travel at a velocity of 300,000 km/sec, whereas that which entered the glass travels at a velocity of 200,000 km/sec. This difference in velocity causes the upper portion of the wave entrance to move ahead of the lower portion so that the wave entrance is no longer vertical but is angulated to the proper. Because the course during which light travels is all the time perpendicular to the aircraft of the wave entrance, the direction of travel of the light beam bends downward. Light rays entering a glass surface perpendicular to the light rays (A) and a glass surface angulated to the light rays (B). This determine demonstrates that the distance between waves after they enter the glass is shortened to about two-thirds that in air. Bending of sunshine rays at each floor of a convex spherical lens displaying that parallel gentle rays are centered to a focus. Bending of light rays at each surface of a concave spherical lens exhibiting that parallel gentle rays are diverged. Half the bending happens when the rays enter the lens, and half happens as the rays exit from the opposite aspect. If the lens has exactly the proper curvature, parallel mild rays passing through every a half of the lens shall be bent exactly enough so that every one the rays will pass by way of a single level, known as the point of interest.
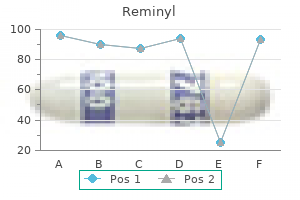
Order reminyl from indiaPain from the viscera is regularly local- surface of the physique, the individual usually localizes it in the dermatomal section from which the visceral organ originated in the embryo, not necessarily where the visceral organ now lies. Pain impulses cross first from the appendix by way of visceral ache fibers positioned inside sympathetic nerve bundles and then into the spinal wire at about T10 or T11; this ache is referred to an space across the umbilicus and is of the aching, cramping kind. Cross section of the spinal twine exhibiting principal ascending tracts on the best and principal descending tracts on the left. Tic Douloureux A lancinating or stabbing kind of pain sometimes occurs in some people over one facet of the face within the sensory distribution area (or a half of the area) of the fifth or ninth nerves; this phenomenon is known as tic douloureux (or trigeminal neuralgia or glossopharyngeal neuralgia). The pain seems like sudden electrical shocks, and it might seem for only some seconds at a time or could also be almost steady. The ache of tic douloureux can usually be blocked by surgically slicing the peripheral nerve from the hypersensitive area. The sensory portion of the fifth nerve is commonly sectioned immediately contained in the cranium, the place the motor and sensory roots of the fifth nerve separate from each other, so that the motor parts, which are essential for many jaw movements, may be spared whereas the sensory elements are destroyed. Furthermore, typically the operation is unsuccessful, indicating that the lesion that causes the ache might be in the sensory nucleus within the mind stem and never in the peripheral nerves. Brown-S�quard Syndrome If the spinal twine is transected completely, all sensations and motor functions distal to the phase of transection are blocked, but if the spinal wire is transected on just one side, the Brown-S�quard syndrome happens. All motor capabilities are blocked on the aspect of the transection in all segments below the level of the transection. Yet, only a few of the modalities of sensation are misplaced on the transected side, and others are misplaced on the alternative facet. The sensations of pain, heat, and cold-sensations served by the spinothalamic pathway- are lost on the opposite side of the body in all dermatomes two to six segments under the level of the transection. These impulses cause ache of the sharp kind immediately over the irritated peritoneum in the best lower quadrant of the abdomen. Some Clinical Abnormalities of Pain and Other Somatic Sensations Hyperalgesia-Hypersensitivity to Pain A ache nervous pathway generally turns into excessively excitable, which provides rise to hyperalgesia. Possible causes of hyperalgesia are the following: (1) excessive sensitivity of the ache receptors, called primary hyperalgesia; and (2) facilitation of sensory transmission, known as secondary hyperalgesia. An example of major hyperalgesia is the intense sensitivity of sunburned pores and skin, which ends from sensitization of the pores and skin pain endings by native tissue products from the burn-perhaps histamine, prostaglandins, and others. Secondary hyperalgesia regularly results from lesions in the spinal wire or the thalamus. Herpes Zoster (Shingles) Occasionally, herpesvirus infects a dorsal root ganglion. This infection causes extreme pain within the dermatomal phase subserved by the ganglion, thus eliciting a segmental sort of ache that circles midway around the body. The illness is called herpes zoster, or shingles, due to a skin eruption that always ensues. The cause of the pain is presumably an infection of the ache neuronal cells within the dorsal root ganglion by the virus. In addition to inflicting ache, the virus is carried by neuronal cytoplasmic move outward through the neuronal peripheral axons to their cutaneous origins. Here the virus causes a rash that vesiculates inside a few days and then crusts over within another few days, all occurring within the dermatomal space served by the infected dorsal root. Pain, Headache, and Thermal Sensations part in all dermatomes below the extent of the transection. Discrete "mild contact" is impaired on the side of the transection as a result of the principal pathway for the transmission of sunshine touch, the dorsal column, is transected. Headache Headaches are a sort of pain referred to the surface of the top from deep head constructions. Some headaches result from ache stimuli arising contained in the skull, but others outcome from ache arising outdoors the cranium, corresponding to from the nasal sinuses. Even slicing or electrically stimulating the sensory areas of the cerebral cortex solely sometimes causes ache; instead, it causes prickly kinds of paresthesias on the area of the physique represented by the portion of the sensory cortex stimulated. Also, nearly any kind of traumatizing, crushing, or stretching stimulus to the blood vessels of the meninges can cause headache. An particularly delicate construction is the center meningeal artery; neurosurgeons are careful to anesthetize this artery specifically when performing mind operations with use of local anesthesia. Conversely, pain impulses from beneath the tentorium enter the central nervous system mainly by way of the glossopharyngeal, vagal, and second cervical nerves, which also provide the scalp above, behind, and slightly below the ear. Subtentorial ache stimuli trigger "occipital headache" referred to the posterior a part of the head. One of essentially the most extreme complications of all is that ensuing from meningitis, which causes irritation of the meninges, together with the sensitive areas of the dura and the delicate areas across the venous sinuses. Such intense harm may cause excessive headache pain referred over the complete head. Removing as little as 20 milliliters of fluid from the spinal canal, notably if the individual stays in an upright place, usually causes intense intracranial headache. The weight of the mind stretches and in any other case distorts the varied dural surfaces and thereby elicits the ache that causes the headache. Migraine headache is a special kind of headache that will end result from abnormal vascular perform, although the exact mechanism is unknown. Migraine complications usually begin with various prodromal sensations, such as nausea, lack of vision in a half of the field of regard, visual aura, and different types of sensory hallucinations. Ordinarily, the prodromal symptoms start 30 to 60 minutes before the start of the headache. Any concept that explains migraine headache should additionally explain the prodromal symptoms. One theory of migraine complications is that prolonged emotion or pressure causes reflex vasospasm of a few of the arteries of the pinnacle, including arteries that provide the brain. The vasospasm theoretically produces ischemia of portions of the mind, which is answerable for the prodromal signs. Then, because of the extreme ischemia, something occurs to the vascular partitions, perhaps exhaustion of smooth muscle contraction, to enable the blood vessels to turn into flaccid and incapable of maintaining regular vascular tone for 24 to forty eight hours. Other theories about the cause of migraine complications embody spreading cortical depression, psychological abnormalities, and vasospasm attributable to excess local potassium in the cerebral extracellular fluid. There may be a genetic predisposition to migraine headaches because a constructive family historical past for migraine has been reported in 65% to 90% of cases. As many individuals have skilled, a headache usually follows extreme alcohol consumption. Discharge frequencies at different skin temperatures of a chilly pain fiber, a chilly fiber, a heat fiber, and a warmth ache fiber. Emotional pressure usually causes lots of the muscles of the top, particularly the muscles connected to the scalp and the neck muscles attached to the occiput, to become spastic; this mechanism is postulated as a common reason for headache. The ache of the spastic head muscular tissues supposedly is referred to the overlying areas of the top and provides one the identical type of headache as do intracranial lesions. The mucous membranes of the nose and nasal sinuses are sensitive to ache, but not intensely so.

Purchase reminyl 8 mg with visaThus, management of potassium concentration is significantly impaired when the aldosterone feedback system is blocked. A comparable impairment of potassium regulation is observed in people with poorly functioning aldosterone suggestions systems, similar to happens in sufferers with major aldosteronism (too much aldosterone) or Addison illness (too little aldosterone). A rise in distal tubular circulate rate, as occurs In addition to its stimulatory effect on renal secretion of potassium, aldosterone additionally will increase cellular uptake of potassium. This contributes to the powerful aldosteronepotassium suggestions system, as discussed beforehand. In this experiment, potassium consumption was elevated virtually sevenfold in canine beneath two circumstances: (1) beneath normal situations; and (2) after the aldosterone feedback system had been blocked by removing the adrenal glands and putting the animals on a onerous and fast rate of aldosterone infusion, in order that plasma aldosterone focus was maintained at a standard degree but might neither improve nor decrease as potassium intake was altered. Conversely, a lower in distal tubular move fee, as brought on by sodium depletion, reduces potassium secretion. The effect of the tubular move price on potassium secretion in the distal and collecting tubules is strongly influenced by potassium intake. There are two major effects of a high-volume flow fee that increase potassium secretion: 1. When potassium is secreted into the tubular fluid, the luminal concentration of potassium will increase, Chapter 30 Renal Regulation of Potassium, Calcium, Phosphate, and Magnesium Na+ consumption Acute Acidosis Decreases Potassium Secretion. Note that a high-sodium food plan decreases plasma aldosterone, which tends to lower potassium secretion by the cortical accumulating tubules. However, the high-sodium food plan simultaneously increases fluid delivery to the cortical accumulating duct, which tends to enhance potassium secretion. This discount in turn decreases intracellular potassium concentration and subsequent passive diffusion of potassium throughout the luminal membrane into the tubule. Acidosis may also scale back the number of potassium channels in the luminal membrane. With extra extended acidosis, lasting over a period of a number of days, there is a rise in urinary potassium excretion. The mechanism for this effect is due partially to an impact of persistent acidosis to inhibit proximal tubular sodium chloride and water reabsorption, which increases distal quantity delivery, thereby stimulating potassium secretion. Thus, chronic acidosis leads to a loss of potassium, whereas acute acidosis leads to decreased potassium excretion. With elevated tubular flow fee, the secreted potassium is continuously flushed down the tubule, minimizing the rise in tubular potassium focus and growing net potassium secretion. The effect of increased tubular flow fee is particularly important in serving to preserve normal potassium excretion throughout modifications in sodium intake. This intake is as a outcome of of their consumption of a food plan containing large amounts of fruits and vegetables and no processed foods. With industrialization and increased consumption of processed meals, which often have high sodium and low potassium content material, there have been dramatic increases in sodium consumption and reduces in potassium intake. In most industrialized international locations, potassium consumption averages only 30 to 70 mmol/day, and sodium consumption averages one hundred forty to 180 mmol/day. Experimental and medical research have shown that the combination of a high-sodium and low-potassium food plan increases the danger for hypertension and associated cardiovascular and kidney diseases. A diet wealthy in potassium, nonetheless, seems to defend against the adverse results of a high-sodium food plan, lowering blood strain and the risk for stroke, coronary artery disease, and kidney disease. The useful effects of increasing potassium consumption are especially obvious when combined with a low-sodium diet. Dietary tips revealed by varied organizations have recommended lowering the dietary consumption of sodium chloride to about sixty five to one hundred mmol/day (corresponding to 1. The extracellular fluid calcium ion concentration usually stays tightly managed within a few proportion points of its normal stage, 2. When the calcium ion focus falls to low levels (hypocalcemia), the excitability of nerve and muscle cells increases markedly and can, in extreme instances, end in hypocalcemic tetany. Hypercalcemia (increased calcium concentration) depresses neuromuscular excitability and might result in cardiac arrhythmias. About 50% of the whole calcium within the plasma (5 mEq/L) exists in the ionized form, which is the shape that has organic activity at cell membranes. The the rest is sure to plasma proteins (40%) or complexed in the nonionized kind with anions corresponding to phosphate and citrate (10%). Changes in plasma hydrogen ion concentration influence calcium binding to plasma proteins. Conversely, with alkalosis, a higher amount of calcium is sure to the plasma proteins. As with different substances in the physique, calcium consumption should be balanced with the online lack of calcium over the lengthy term. Unlike ions such as sodium and chloride, however, a lot of the calcium excretion happens in the feces. The ordinary fee of dietary calcium intake is about one thousand mg/ day, with about 900 mg/day of calcium excreted in the feces. Under certain circumstances, fecal calcium excretion can exceed calcium ingestion as a result of calcium can be secreted into the intestinal lumen. Therefore, the gastrointestinal tract and regulatory mechanisms that affect intestinal calcium absorption and secretion play a serious function in calcium homeostasis, as mentioned in Chapter eighty. Almost all of the calcium in the physique (99%) is saved within the bone, with solely about zero. The bone, subsequently, acts as a big reservoir for calcium and as a source of calcium when extracellular fluid calcium concentration tends to lower. Therefore, over the lengthy term, intake of calcium must be balanced with calcium excretion by the gastrointestinal tract and kidneys. The control of gastrointestinal calcium reabsorption and calcium trade in the bones is discussed elsewhere; the rest of this part focuses on the mechanisms that control renal calcium excretion. Therefore, the rate of renal calcium excretion is calculated as follows: Renal calcium excretion = Calcium filtered - Calcium reabsorbed Only about 60% of the plasma calcium is ionized, with 40% being bound to the plasma proteins and 10% complexed with anions similar to phosphate. Normally, about 99% of the filtered calcium is reabsorbed by the tubules, with solely about 1% of the filtered calcium being excreted. About 65% of the filtered calcium is reabsorbed in the proximal tubule, 25% to 30% is reabsorbed in the loop of Henle, and 4% to 9% is reabsorbed in the distal and amassing tubules. The mechanism for this active transport is much like that within the proximal tubule and thick ascending limb. Mechanisms of calcium reabsorption by paracellular and transcellular pathways within the proximal tubular cells. With calcium depletion, calcium excretion by the kidneys decreases on account of enhanced tubular reabsorption. Only about 20% of proximal tubular calcium reabsorption happens through the transcellular pathway in two steps; 1. Calcium diffuses from the tubular lumen into the cell down an electrochemical gradient because of the a lot higher concentration of calcium in the tubular lumen, compared with the epithelial cell cytoplasm, and because the cell interior has a negative cost relative to the tubular lumen. In the loop of Henle, calcium reabsorption is re- stricted to the thick ascending limb. Approximately 50% of calcium reabsorption within the thick ascending limb occurs via the paracellular route by passive diffusion as a outcome of the slight optimistic cost of the tubular lumen relative to the interstitial fluid.
Purchase reminyl lineNote that increasing alveolar ventilation to about twice normal raises extracellular fluid pH by about 0. Conversely, a lower in alveolar ventilation to one-fourth normal reduces the pH by 0. Because the alveolar air flow price can change markedly, from as little as zero to as excessive as 15 times regular, one can easily understand how a lot the pH of the body fluids may be modified by the respiratory system. The change in air flow price per unit pH change is far greater at decreased levels of pH (corresponding to elevated H+ concentration) in contrast with elevated ranges of pH. As discussed previously, the respiratory responses to metabolic alkalosis are limited by hypoxemia associated with reduced alveolar air flow. Because elevated H+ concentration tory regulation of acid�base stability is a physiological sort of buffer system as a outcome of it acts rapidly and retains the H+ focus from altering an extreme amount of until the slowly responding kidneys can remove the imbalance. In common, the general buffering power of the respiratory system is one to two times as great as the buffering energy of all different chemical buffers within the extracellular fluid combined. That is, one to two times as a lot acid or base can normally be buffered by this mechanism as by the chemical buffers. This mechanism decreases the Pco2 in extracellular fluid and reduces H+ focus back toward normal. Conversely, if H+ focus falls under regular, the respiratory heart turns into depressed, alveolar air flow decreases, and H+ focus will increase again toward regular. Although alkalosis tends to depress the respiratory centers, the response is usually much less robust and fewer predictable than the response to metabolic acidosis; the hypoxemia associated with reduced alveolar air flow finally prompts oxygensensitive chemoreceptors that tend to stimulate air flow and limit the respiratory compensation for metabolic alkalosis. Also, the power to reply to metabolic acidosis is impaired as a result of the compensatory reductions in Pco2 that might usually occur via elevated air flow are blunted. In these circumstances, the kidneys characterize the only real remaining physiological mechanism for returning pH toward regular after the initial chemical buffering within the extracellular fluid has occurred. Excreting acidic urine reduces the amount of acid in extracellular fluid, whereas excreting basic urine removes base from the extracellular fluid. The overall mechanism whereby the kidneys excrete acidic or fundamental urine is as follows. Large numbers of H+ are additionally secreted into the tubular lumen by the tubular epithelial cells, thus removing acid from the blood. Each day, the body produces about 80 mEq of nonvolatile acids, primarily from metabolism of proteins. Ordinarily, the respiratory mechanism for controlling H+ focus is roughly 50% to 75% efficient, comparable to a feedback acquire of 1 to 3 for metabolic acidosis. The primary mechanism for removal of these acids from the physique is renal excretion. Then, an extra 80 mEq of H+ should be secreted to rid the physique of the nonvolatile acids produced each day for a total of 4400 mEq of H+ secreted into the tubular fluid each day. All these processes are achieved through the same fundamental mechanisms, as mentioned within the subsequent few sections. This secondary energetic secretion of H+ is coupled with the transport of Na+ into the cell on the luminal membrane by the sodium-hydrogen exchanger protein, and the energy for H+ secretion towards a concentration gradient is derived from the sodium gradient favoring Na+ motion into the cell. About 95% of the bicarbonate is reabsorbed on this manner, requiring about 4000 mEq of H+ to be secreted every day by the tubules. The H+ is secreted from the cell into the tubular lumen by sodium-hydrogen countertransport. This excess H+ (80 mEq/day) rids the body of nonvolatile acids produced by metabolism. This sample of H+ secretion happens within the proximal tubule, thick ascending section of the loop of Henle, and early distal tubule. The gradient for Na+ movement into the cell then provides the power for shifting H+ in the incorrect way from the interior of the cell to the tubular lumen. The characteristics of this transport are totally different from those mentioned for the proximal tubule, loop of Henle, and early distal tubule. Active secretion of H+ via the luminal membrane of the sort A intercalated epithelial cells of the late distal and accumulating tubules. Primary lively secretion of H+ happens in special forms of cells known as the kind A intercalated cells of the late distal tubule and in the accumulating tubules. The main difference is that H+ moves throughout the luminal membrane by an lively H+ pump as a substitute of by counter-transport, as happens in the early elements of the nephron. Although secretion of H+ within the late distal tubule and amassing tubules accounts for much less than about 5% of the whole H+ secreted, this mechanism is important in forming maximally acidic urine. In the proximal tubules, H+ concentration could be increased only about threefold to fourfold and the tubular fluid pH can be lowered to only about 6. However, H+ concentration could be increased as a lot as 900-fold in the collecting tubules. To excrete the eighty mEq of nonvolatile acid formed by metabolism each day, about 2667 liters of urine would have to be excreted if the H+ remained free in resolution. The excretion of large quantities of H+ (on occasion as a lot as 500 mEq/day) in the urine is accomplished primarily by combining the H+ with buffers within the tubular fluid. Both turn into concentrated in the tubular fluid as a outcome of water is often reabsorbed to a larger extent than phosphate by the renal tubules. Another issue that makes phosphate essential as a tubular buffer is the fact that the pK of this technique is about 6. Under regular circumstances, the urine is slightly acidic, and the urine pH is close to the pK of the phosphate buffer system. Therefore, within the tubules, the phosphate buffer system normally functions close to its handiest pH range. There is one essential distinction in this sequence of H+ excretion from that discussed previously. Under normal conditions, a lot of the filtered phosphate is reabsorbed, and only 30 to forty mEq/day can be found for buffering H+. Therefore, much of the buffering of extra H+ in the tubular fluid in acidosis occurs via the ammonia buffer system. Ammonium ion is synthesized from glutamine, which comes mainly from metabolism of amino acids in the liver. This course of additionally provides the most important mechanism for generating new bicarbonate during continual acidosis. This titration reverses the events that occurred within the tubular lumen when the tubular fluid was titrated by secreted H+. To keep acid�base steadiness, the net acid excretion should equal the nonvolatile acid manufacturing in the body. Therefore, the speed of H+ secretion must be rigorously regulated if the kidneys are to carry out their capabilities in acid�base homeostasis successfully. The most essential stimuli for rising H+ secretion by the tubules in acidosis are as follows: (1) a rise in Pco2 of the extracellular fluid in respiratory acidosis; and (2) an increase in H+ focus of the extracellular fluid (decreased pH) in respiratory or metabolic acidosis. The tubular cells reply directly to an increase in Pco2 of the blood, as in respiratory acidosis, with an increase within the price of H+ secretion, as follows. The increased Pco2 raises the Pco2 of the tubular cells, causing elevated formation of H+ in the tubular cells, which in turn stimulates secretion of H+.
Cheap reminyl ukConsequently, there can no longer be any blood flow from peripheral vessels back to the proper atrium. That is, the greater the difference between the Psf and right atrial stress, the greater turns into the venous return. Therefore, the distinction between these two pressures known as the strain gradient for venous return. Mostoftheresistanceto venous return occurs in the veins, although some occurs within the arterioles and small arteries as well. Why is venous resistance so essential in determining the resistance to venous return The reply is that when the resistance within the veins will increase, blood begins to be dammed up, mainly in the veins themselves. However, the venous strain rises little or no because the veins are highly distensible. Conversely, when arteriolar and small artery resistances increase, blood accumulates in the arteries, which have a capacitance only one thirtieth as nice as that of the veins. Therefore, even slight accumulation of blood in the arteries raises the pressure greatly-30 times as much as within the veins-and this excessive stress overcomes a lot of the elevated resistance. Mathematically,itturnsoutthatabouttwo-thirdsofthe so-called resistance to venous return is determined by venous resistance, and about one-third is determined by the arteriolar and small artery resistance. Venous return curves depicting the effect of altering the resistance to venous return. Conversely, a rise in resistance to twice regular rotates the curve downward to half as nice a slope. Therefore, the very best stage to which the right atrial stress can rise, regardless ofhowmuchtheheartmightfail,isequaltothePsf. This requirement implies that (1) the venous return from the systemic circulation must equal the cardiac output from the center and (2) the best atrial pressure is identical for the heart and systemic circulation. In the wholesome adult, the approximate values for these are as follows: venous return = 5 L/min,Psf=7mmHg,rightatrialpressure=0mmHg, and resistance to venous return = 1. Therefore, in the regular circulation, the best atrial pressure, cardiac output, and venous return are all depicted by point A, known as the equilibrium point, giving a standard worth for cardiac output of 5 L/min and a right atrial stress of 0 mm Hg. Combinations of the main patterns of venous return curves displaying the consequences of simultaneous modifications in the mean systemic filling pressure (Psf) and in resistance to venous return. At the identical time, the increased blood volume distends the blood vessels, lowering their resistance and thereby lowering the resistance to venous return, which rotates the curve upward. This new curve equates with the cardiac output curve at point B, exhibiting that the cardiac output and venous return improve 2. The two strong curves demonstrate an evaluation of cardiac output and right atrial stress when the cardiac output (red line) and venous return (blue line) curves are regular. Transfusion of blood equal to 20% of the blood quantity causes the venous return curve to turn into the dashed curve. As a result, the cardiac output and right atrial strain shift from level A to point B. Determine the momentary pumping ability of the guts, and depict this capability in the type of a cardiac output curve. Determine the momentary state of circulate from the systemic circulation into the guts, and depict this state of move in the type of a venous return curve. Two curves within the figure depict the conventional cardiac output curve (red line) and the traditional venous return curve (blue line). There is simply one point on the graph, level A, at which the venous return equals the cardiac output and at which the best atrial pressure is the same for each the 254 brought on by increased blood quantity lasts for only some minutes because several compensatory effects immediately begin to happen: 1. The elevated cardiac output will increase the capillary strain in order that fluid begins to transude out of the capillaries into the tissues, thereby returning the blood volume towards regular. The elevated stress within the veins causes the veins to continue distending gradually by the mechanism known as stress-relaxation, especially causing the venous blood reservoirs, such because the liver and spleen, to distend, thus lowering the Psf. The extra blood circulate by way of the peripheral tissues causes an autoregulatory increase in the peripheral vascular resistance, thus growing the resistance to venous return. These elements trigger the Psf to return towards normal and the resistance vessels of the systemic circulation to constrict. Therefore, steadily, over a period of 10 to 40 minutes, the cardiac output returns nearly to regular. Sympathetic stimulation affects the heart and systemic circulation: (1) it makes the center a stronger pump; and (2) within the systemic circulation, it will increase the Psf due to contraction of the peripheral vessels, particularly the veins, and it will increase the resistance to venous return. Analysis of the effect on cardiac output of (1) average sympathetic stimulation (from point A to point C), (2) maximal sympathetic stimulation (point D), and (3) sympathetic inhibition caused by total spinal anesthesia (point B). Sympathetic stimulation also will increase pumping effectiveness of the guts by almost 100 percent. As a end result, the cardiac output rises from the traditional worth at equilibrium point A to about double normal at equilibrium point D, and yet the right atrial strain hardly adjustments. Thus, different degrees of sympathetic stimulation can enhance the cardiac output progressively to about twice normal for short periods, until other compensatory effects happen within seconds or minutes to return cardiac output to practically regular. The sympathetic nervous system could be blocked by inducing whole spinal anesthesia or through the use of a drug, corresponding to hexamethonium, that blocks transmission of nerve signals by way of the autonomic ganglia. The cardiac output falls from level A to point B, which is a decrease to about 60% of regular. The curves crossing at point B show the circulatory condition instantly after opening the big fistula. The principal effects are as follows: (a) a sudden and precipitous rotation of the venous return curve upward attributable to the large decrease in resistance to venous return when blood is allowed to move with almost no obstacle directly from the big arteries into the venous system, bypassing most of the resistance parts of the peripheral circulation; and (b) a slight increase within the degree of the cardiac output curve as a result of opening the fistula decreases the peripheral resistance and allows an acute fall in arterial pressure in opposition to which the guts can pump more simply. The net outcome, depicted by level B, is a rise in cardiac output from 5 L/min up to 13 L/min and a rise in right atrial pressure to about +3 mm Hg. The cardiac output now rises to almost sixteen L/min, and the right atrial pressure rises to about four mm Hg. ThePsfhasnowrisento+12 mm Hg, shifting the venous return curve one other 3 mm Hg to the best. Also, the extended elevated workload on the center has brought on the center muscle to hypertrophy barely, elevating the extent of the cardiac output curve nonetheless additional. In Chapter 21, evaluation of cardiac output regulation throughout train is presented. In Chapter 22, analyses of cardiac output regulation at various levels of congestive coronary heart failure are mentioned. From these knowledge, one can calculate that each liter of blood passing through the lungs absorbs forty ml of oxygen. Because the total quantity of oxygen absorbed into the blood from the lungs every minute is 200 ml, dividing 200 by forty calculates to a complete of 5 liters of blood that should pass through the pulmonary circulation every minute to take in this quantity of oxygen. Therefore, the quantity of blood flowing via the lungs each minute is 5 liters, which can additionally be a measure of the cardiac output. In animal experiments, one can measure the cardiac output utilizing an electromagnetic or ultrasonic flowmeter placed on the aorta or pulmonary artery to measure cardiac output. It demonstrates that the blood move rises quickly to a peak throughout systole after which, on the end of systole, it reverses for a fraction of a second.
Casein-derived peptide (Casein Peptides). Reminyl. - Are there any interactions with medications?
- How does Casein Peptides work?
- What is Casein Peptides?
- Dosing considerations for Casein Peptides.
- Are there safety concerns?
- High blood pressure, high cholesterol, anxiety, fatigue, epilepsy, intestinal disorders, cancer prevention, and reducing stress.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97053
Cheap reminyl 8mg visaTherefore, the infarcted area takes on a bluish-brown hue, and the blood vessels of the world appear to be engorged, despite lack of blood circulate. In comparability, about 8 ml oxygen/100 g are delivered to the conventional resting left ventricle each minute. This happens because the subendocardial muscle has the next oxygen consumption and further issue obtaining sufficient blood move as a result of the blood vessels within the subendocardium are intensely compressed by systolic contraction of the heart, as defined earlier. Therefore, any situation that compromises blood circulate to any space of the heart normally causes damage first in the subendocardial regions, and the damage then spreads outward toward the epicardium. When a few of the cardiac muscle fibers more than 40% of the left ventricle is infarcted, and demise occurs in more than 70% of patients once cardiac shock develops. Therefore, much of the pumping pressure of the ventricle is dissipated by bulging of the area of nonfunctional cardiac muscle. When the heart becomes incapable of contracting with sufficient drive to pump enough blood into the peripheral arterial tree, cardiac failure and demise of peripheral tissues ensue as a end result of peripheral ischemia. This condition, referred to as coronary shock, cardiogenic shock, cardiac shock, or low cardiac output failure, is mentioned more totally in the next chapter. Damming of blood within the veins usually causes little problem during the first few hours after a myocardial infarction. Instead, symptoms develop a few days later as a outcome of the acutely diminished cardiac output results in diminished blood circulate to the kidneys. Then, for causes discussed in Chapter 22, the kidneys fail to excrete sufficient urine. This adds progressively to the entire blood quantity and, due to this fact, results in congestive signs. Consequently, many sufferers who seemingly are getting along well during the first few days after the onset of heart failure will all of a sudden expertise acute pulmonary edema and often will die within a couple of hours after the appearance of the preliminary pulmonary symptoms. In many people who die of coronary occlusion, dying occurs due to sudden ventricular fibrillation. The tendency for fibrillation to develop is particularly nice after a big infarction, but fibrillation can sometimes happen after small occlusions as properly. Some patients with continual coronary insufficiency die suddenly of fibrillation without having any acute infarction. Chapter 21 Muscle Blood Flow and Cardiac Output During Exercise Fibrillation is most probably to occur during two particularly dangerous durations after coronary infarction. Fibrillation can also happen many days after the infarct but is much less more doubtless to happen then. At least four factors are concerned within the tendency for the center to fibrillate, as follows: 1. Acute loss of blood supply to the cardiac muscle causes rapid depletion of potassium from the ischemic musculature. This additionally will increase the potassium focus within the extracellular fluids surrounding the cardiac muscle fibers. Experiments by which potassium has been injected into the coronary system have demonstrated that an elevated extracellular potassium concentration will increase the irritability of the cardiac musculature and, subsequently, its likelihood of fibrillating. Ischemia of the muscle causes an damage present, described in Chapter 12 in relation to electrocardiograms in sufferers with acute myocardial infarction. Therefore, electric present flows from this ischemic area of the guts to the normal space and might elicit irregular impulses, which might trigger fibrillation. The sympathetic stimulation additionally will increase irritability of the cardiac muscle and thereby predisposes to fibrillation. Cardiac muscle weak point caused by the myocardial infarction often causes the ventricle to dilate excessively. This extreme dilation increases the pathway size for impulse conduction in the heart and incessantly causes abnormal conduction pathways all the greatest way around the infarcted space of the cardiac muscle. When this occurs, the dead muscle bulges outward to a extreme diploma with each coronary heart contraction, and this systolic stretch turns into larger and larger until finally the center ruptures. When a ventricle does rupture, lack of blood into the pericardial space causes fast improvement of cardiac tamponade-that is, compression of the center from the outside by blood collecting within the pericardial cavity. When the realm of ischemia is small, little or no death of the muscle cells could happen, but part of the muscle often does turn into quickly nonfunctional because of inadequate diet to help muscle contraction. Immediately across the dead area is a nonfunctional space, with failure of contraction and usually failure of impulse conduction. Then, during the ensuing days, this area of lifeless fibers enlarges as a end result of many of the marginal fibers finally succumb to the extended ischemia. At the same time, because of the enlargement of collateral arterial channels supplying the outer rim of the infarcted area, a lot of the nonfunctional muscle recovers. After a number of days to 3 weeks, most of the nonfunctional muscle becomes useful once more or dies. In the meantime, fibrous tissue begins growing among the lifeless fibers because ischemia can stimulate progress of fibroblasts and promote improvement of greater than normal quantities of fibrous tissue. Finally, the normal areas of the guts progressively hypertrophy to compensate, at least partially, for the lost useless cardiac musculature. By these means, the center recovers partially or virtually completely within a quantity of months, relying on the severity of the infarction and cardiac tissue dying. Even when the cardiac reserve is lowered to as little as 100 percent, the individual can still perform most traditional daily actions but not strenuous train, which might overload the center. The excessive concentrations of these irregular merchandise then stimulate ache nerve endings in the cardiac muscle, sending ache impulses through sensory afferent nerve fibers into the central nervous system. In most individuals who degree of cardiac mobile death is determined by the degree of ischemia and workload on the center muscle. When the workload is tremendously elevated, such as throughout exercise, in severe emotional strain, or on account of fatigue, the center needs increased oxygen and different vitamins for sustaining its life. Furthermore, anastomotic blood vessels that supply blood to ischemic areas of the guts should additionally nonetheless provide the areas of the guts that they usually provide. When the guts becomes excessively active, the vessels of the normal musculature turn out to be greatly dilated. This dilation allows a lot of the blood flowing into the coronary vessels to flow via the conventional muscle tissue, thus leaving little blood to circulate by way of the small anastomotic channels into the ischemic area. As a outcome, the ischemic situation worsens, a situation called the coronary steal syndrome. Consequently, an important factor in the therapy of a patient with myocardial infarction is observance of absolute physique rest during the restoration process. In addition, the ache is often referred to distant floor areas of the body, usually to the left arm and left shoulder but additionally frequently to the neck and even to the side of the face. The cause for this distribution of pain is that in embryonic life, the guts originates within the neck, as do the arms. Therefore, each the heart and these surface areas of the body obtain ache nerve fibers from the identical spinal wire segments. Most individuals who have continual angina pectoris feel ache after they train or after they experience feelings that enhance metabolism of the heart or briefly constrict the coronary vessels because of sympathetic vasoconstrictor nerve signals.
Syndromes - Speech impairment
- Sick sinus syndrome
- Senile cardiac amyloid
- If traveling outside the United States, learn about the health care in the country you are visiting. If you can, find out where you would go if you needed medical help.
- Headache
- Diarrhea and other infections that last a long time, such as parasites
- Seizures
- Do NOT try to give anything by mouth.
Buy reminyl 8 mg lowest priceDuring heavy exercise or other conditions of excessive metabolic exercise, or when blood circulate via the tissues is sluggish, the decrease in pH within the tissue blood (and in the tissues themselves) can be as much as 0. In different phrases, when fat are metabolized, the respiratory quotient of the chemical reactions within the tissues is about 0. Geers C, Gros G: Carbon dioxide transport and carbonic anhydrase in blood and muscle. The bioengineering dilemma within the structural and useful design of the blood-gas barrier. That is: R= Rate of carbon dioxide output Rate of oxygen uptake the worth for R modifications under totally different metabolic situations. When a person is utilizing carbohydrates solely for body metabolism, R rises to 1. Conversely, when a person is utilizing fat solely for metabolic vitality, the R level falls to as low as zero. This article describes the function of this neurogenic system for regulation of respiration. Even when all of the peripheral nerves coming into the medulla have been sectioned, and the mind stem has been transected above and under the medulla, this group of neurons still emits repetitive bursts of inspiratory neuronal motion potentials. In primitive animals, neural networks have been discovered by which exercise of 1 set of neurons excites a second set, which in turn inhibits the first. Then, after a time period, the mechanism repeats itself, persevering with throughout the lifetime of the animal. Similar networks of neurons are present within the human being, situated completely inside the medulla; it in all probability entails not only the dorsal respiratory group but adjacent areas of the medulla as properly and is liable for the fundamental rhythm of respiration. It is divided into three main collections of neurons: (1) a dorsal respiratory group, situated within the dorsal portion of the medulla, which primarily causes inspiration; (2) a ventral respiratory group, positioned in the ventrolateral a half of the medulla, which mainly causes expiration; and (3) the pneumotaxic heart, situated dorsally in the superior portion of the pons, which primarily controls rate and depth of respiratory. Instead, it begins weakly and will increase steadily in a ramp manner for about 2 seconds in normal respiration. It then ceases abruptly for approximately the next 3 seconds, which turns off the excitation of the diaphragm and permits elastic recoil of the lungs and chest wall to trigger expiration. Next, the inspiratory sign begins again for another cycle; this cycle repeats many times, with expiration occurring in between. The obvious benefit of the ramp is that it causes a gradual increase in the volume of the lungs throughout inspiration, quite than inspiratory gasps. Control of the speed of improve of the ramp signal so that in heavy respiration, the ramp will increase rapidly and due to this fact fills the lungs rapidly. Control of the limiting level at which the ramp all of a sudden ceases, which is the similar old technique for controlling the rate of respiration. The primary effect of this heart is to management the "switch-off " point of the inspiratory ramp, thereby controlling the duration of the filling part of the lung cycle. The operate of the pneumotaxic center is primarily to limit inspiration, which has a secondary impact of increasing the speed of respiratory as a end result of limitation of inspiration also shortens expiration and the entire period of each respiration. A robust pneumotaxic signal can improve the rate of respiratory to 30 to 40 breaths/min, whereas a weak pneumotaxic sign may cut back the rate to only 3 to 5 breaths/min. When the respiratory drive for increased pulmonary ventilation becomes higher than normal, respiratory signals spill over into the ventral respiratory neurons from the basic oscillating mechanism of the dorsal respiratory area. As a consequence, the ventral respiratory space also contributes additional respiratory drive. Electrical stimulation of some of the neurons in the ventral group causes inspiration, whereas stimulation of others causes expiration. They are particularly important in providing the highly effective expiratory signals to the abdominal muscular tissues during very heavy expiration. Thus, this space operates roughly as an overdrive mechanism when high levels of pulmonary air flow are required, particularly during heavy exercise. Most importantly, located within the muscular portions of the walls of the bronchi and bronchioles all through the lungs are stretch receptors that transmit alerts via the vagi into the dorsal respiratory group of neurons when the lungs become overstretched. This reflex also will increase the speed of respiration, as is true for signals from the pneumotaxic heart. Therefore, this reflex seems to be mainly a protecting mechanism for stopping excess lung inflation somewhat than an essential consider normal management of air flow. The perform of this neuronal group differs from that of the dorsal respiratory group in several essential ways: 1. The neurons of the ventral respiratory group stay nearly totally inactive throughout normal quiet respiration. Therefore, regular quiet respiration is triggered solely by repetitive inspiratory alerts from the dorsal respiratory group transmitted mainly to the diaphragm, and expiration outcomes from elastic recoil of the lungs and thoracic cage. The main objective of the rest of this chapter is to talk about this control of ventilation in accord with the respiratory needs of the body. It is lucky, due to this fact, that respiratory activity is highly aware of modifications in each of those substances. Instead, it acts virtually entirely on peripheral chemoreceptors positioned in the carotid and aortic bodies, and these chemoreceptors in turn transmit applicable nervous indicators to the respiratory middle for management of respiration. Stimulation of the brain stem inspiratory space by indicators from the chemosensitive area positioned bilaterally in the medulla, lying solely a fraction of a millimeter beneath the ventral medullary surface. Note additionally that H+ stimulates the chemosensitive area, but carbon dioxide within the fluid provides rise to many of the H+. We have mainly discussed three areas of the respiratory center-the dorsal respiratory group of neurons, the ventral respiratory group, and the pneumotaxic center. This space is extremely sensitive to changes in either blood Pco2 or H+ focus, and it in turn excites the opposite portions of the respiratory center. Consequently, each time the blood Pco2 increases, so does the Pco2 of both the interstitial fluid of the medulla and the cerebrospinal fluid. Effects of elevated arterial blood Pco2 and decreased arterial pH (increased H+ concentration) on the speed of alveolar ventilation. Respiratory management by peripheral chemoreceptors in the carotid and aortic our bodies. By distinction, the change in respiration in the normal blood pH vary, which is between 7. Yet, for those special situations in which the tissues get into trouble for lack of O2, the body has a special mechanism for respiratory control situated in the peripheral chemoreceptors, outside the mind respiratory middle. This mechanism responds when the blood O2 falls too low, primarily under a Po2 of 70 mm Hg, as defined within the subsequent section. Special nervous chemical receptors, known as chemoreceptors, are situated in a number of areas outside the mind. The chemoreceptors transmit nervous indicators to the respiratory center in the mind to assist regulate respiratory exercise. The carotid our bodies are positioned bilaterally within the bifurcations of the frequent carotid arteries. Changes in O2 focus have nearly no direct effect on the respiratory middle itself to alter respiratory drive-although O2 modifications do have an indirect impact, appearing by way of the peripheral chemoreceptors, as defined in the next part. We learned in Chapter 41 that the hemoglobin-oxygen buffer system delivers virtually precisely regular quantities of O2 to the tissues, even when the pulmonary Po2 changes from a worth as low as 60 mm Hg as a lot as a worth as excessive as one thousand mm Hg. Therefore, besides underneath particular circumstances, adequate delivery of O2 can occur despite adjustments in lung air flow starting from slightly beneath half-normal to as excessive as 20 or more occasions normal.
Effective reminyl 4mgThe cerebellum appears to evaluate the "intentions" of the upper levels of the motor management system, as transmitted to the intermediate cerebellar zone by way of the corticopontocerebellar tract, with the "efficiency" by the respective parts of the body, as transmitted again to the cerebellum from the periphery. In fact, the ventral spinocerebellar tract even transmits back to the cerebellum an "efference" copy of the particular motor management indicators that reach the anterior motor neurons, and this information can be built-in with the signals arriving from the muscle spindles and other proprioceptor sensory organs, transmitted principally in the dorsal spinocerebellar tract. For motor control by the nervous system, the cerebellum supplies most of this damping perform. These movements are referred to as ballistic actions, which means that the whole motion is preplanned and set into movement to go a selected distance after which to stop. Another essential example is the saccadic movements of the eyes, by which the eyes jump from one place to the subsequent when reading or when taking a look at successive factors along a road as a person is shifting in a automotive. Therefore, in the absence of the cerebellar circuit, the motor cortex has to think further exhausting to turn ballistic actions on and off. Also, the built-in timing circuits of the cerebellar cortex are elementary to this particular capacity of the cerebellum. If overshooting occurs in a person whose cerebellum has been destroyed, the aware centers of the cerebrum finally recognize this error and provoke a motion within the reverse path to try and deliver the arm to its meant place. However, the arm, by advantage of its momentum, overshoots as soon as extra in the reverse direction, and appropriate corrective indicators should once more be instituted. Thus, the arm oscillates back and forth past its supposed point for a number of cycles before it finally fixes on its mark. If the cerebellum is intact, acceptable learned, subconscious indicators cease the movement exactly at the intended point, thereby stopping the overshoot and the tremor. All control methods regulating pendular components that have inertia must have damping circuits built 718 Cerebrocerebellum-Function of the Large Lateral Zone of the Cerebellar Hemisphere to Plan, Sequence, and Time Complex Movements In people the lateral zones of the two cerebellar hemispheres are highly developed and greatly enlarged. This characteristic goes together with human abilities to plan and carry out intricate sequential patterns of movement, particularly with the hands and fingers, and to converse. Even so, destruction of the lateral zones of the cerebellar hemispheres, along with their deep nuclei, the dentate nuclei, can lead to excessive incoordination of complex purposeful actions of the palms, fingers, and toes and of the speech equipment. However, experimental research suggest that these parts of the cerebellum are concerned with two other important but oblique elements of motor management: (1) planning of sequential actions and (2) "timing" of the sequential actions. The planning of sequential movements requires that the lateral zones of the hemispheres communicate with each the premotor and sensory parts of the cerebral cortex, and it requires two-way communication between these cerebral cortex areas with corresponding areas of the basal ganglia. It appears that the "plan" of sequential actions actually begins in the sensory and premotor areas of the cerebral cortex, and from there the plan is transmitted to the lateral zones of the cerebellar hemispheres. Then, amid a lot two-way visitors between the cerebellum and the cerebral cortex, applicable motor alerts provide transition from one sequence of movements to the next. Thus, the lateral cerebellar zones appear to be concerned not with what motion is happening at a given second but with what will be happening during the next sequential motion a fraction of a second or maybe even seconds later. In the absence of the massive lateral zones of the cerebellar hemispheres, this capability is significantly disturbed for fast movements. As an example, an individual can predict from the changing visible scene how rapidly he or she is approaching an object. A striking experiment that demonstrates the importance of the cerebellum on this ability is the effects of eradicating the big lateral portions of the cerebellum in monkeys. It is quite possible that the cerebellum provides a "time base," perhaps utilizing time-delay circuits, in opposition to which indicators from different parts of the central nervous system may be in contrast. It is commonly stated that the cerebellum is especially helpful in deciphering rapidly changing spatiotemporal relations in sensory info. Clinical Abnormalities of the Cerebellum Destruction of small parts of the lateral cerebellar cortex seldom causes detectable abnormalities in motor operate. Thus, the remaining portions of the motor management system are able to compensating to a great extent for lack of components of the cerebellum. To cause serious and continuing dysfunction of the cerebellum, the cerebellar lesion usually should involve a quantity of of the deep cerebellar nuclei-the dentate, interposed, or fastigial nuclei. In the absence of those cerebellar zones, one loses the unconscious ability to predict how far the different elements of the body will move in a given time. Without this timing functionality, the person becomes unable to determine when the following sequential motion needs to begin. As a result, the succeeding movement may start too early or, extra likely, too late. Therefore, lesions in the lateral zones of the cerebellum trigger complex actions. Such cerebellar lesions are mentioned to cause failure of clean progression of movements. The cerebrocerebellum (the giant lateral lobes) Two of crucial symptoms of cerebellar disease are dysmetria and ataxia. Therefore, the actions ordinarily overshoot their supposed mark; then, the aware portion of the brain overcompensates in the different way for the succeeding compensatory motion. This impact known as dysmetria, and it leads to uncoordinated actions which are referred to as ataxia. Dysmetria and ataxia can also end result from lesions in the spinocerebellar tracts as a end result of feedback information from the transferring parts of the body to the cerebellum is important for cerebellar timing of movement termination. Past Pointing Past pointing signifies that in the absence of the cerebellum, an individual ordinarily moves the hand or another shifting part of the body considerably past the point of intention. Failure of Progression Dysdiadochokinesia-Inability to Perform Rapid Alternating Movements. When the motor management system fails to additionally helps to "time" occasions other than movements of the physique. As a end result, the succeeding movement may begin much too early or much too late, so no orderly "progression of motion" can happen. One can demonstrate this impact readily by having a affected person with cerebellar damage flip one hand upward and downward at a fast rate. The affected person quickly "loses" all notion of the instantaneous position of the hand during any portion of the movement. As a end result, a collection of stalled tried however jumbled actions occurs instead of the conventional coordinate upward and downward motions. Another example in which failure of development occurs is in talking as a end result of the formation of phrases is dependent upon rapid and orderly succession of individual muscle movements within the larynx, mouth, and respiratory system. Cerebellar nystagmus is tremor of the eyeballs that normally occurs when one attempts to fixate the eyes on a scene to one facet of the head. Hypotonia-Decreased Tone of the Musculature cerebral cortex and spinal twine cross by way of the house that lies between the major plenty of the basal ganglia, the caudate nucleus and the putamen. It is important for our current discussion due to the intimate association between the basal ganglia and the corticospinal system for motor control. To the left is shown the motor cortex, thalamus, and related mind stem and cerebellar circuitry. To the best is the main circuitry of the basal ganglia system, displaying the tremendous interconnections among the many basal ganglia plus extensive input and output pathways between the other motor areas of the mind and the basal ganglia. In the following few sections we focus particularly on two main circuits, the putamen circuit and the caudate circuit. When the basal ganglia sustain serious injury, the cortical system of motor management can not provide these patterns.
Purchase reminyl 4mg onlineThus, active reabsorption of sodium is carefully coupled to passive reabsorption of chloride by the use of an electrical potential and a chloride concentration gradient. The most essential of the secondary lively transport processes for chloride reabsorption includes the co-transport of chloride with sodium across the luminal membrane. Urea is also passively reabsorbed from the tubule, however to a much lesser extent than chloride ions. In some elements of the nephron, particularly the inner medullary amassing duct, passive urea reabsorption is facilitated by particular urea transporters. The remaining urea passes into the urine, permitting the kidneys to excrete massive quantities of this waste product of metabolism. In mammals, more than 90% of waste nitrogen, primarily generated within the liver as a product of protein metabolism, is normally excreted by the kidneys as urea. Another waste product of metabolism, creatinine, is a fair bigger molecule than urea and is actually impermeant to the tubular membrane. The proximal tubules reabsorb about 65% of the filtered sodium, chloride, bicarbonate, and potassium and essentially all the filtered glucose and amino acids. The proximal tubules also secrete organic acids, bases, and hydrogen ions into the tubular lumen. With these generalizations in mind, we can now discuss the totally different traits of the person tubular segments that enable them to perform their specific features. Only the tubular transport functions that are quantitatively most important might be mentioned, particularly as they relate to the reabsorption of sodium, chloride, and water. In subsequent chapters, we focus on the reabsorption and secretion of other substances in numerous elements of the tubular system. These percentages may be elevated or decreased in several physiological situations, as mentioned later. The high capacity of the proxi- the extensive membrane floor of the epithelial brush border is also loaded with protein provider molecules that transport a large fraction of the sodium ions across the luminal membrane linked by way of the co-transport mechanism with a quantity of organic vitamins corresponding to amino acids and glucose. Additional sodium is transported from the tubular lumen into the cell by counter-transport mechanisms that reabsorb sodium while secreting other substances into the tubular lumen, particularly hydrogen ions. In the first half of the proximal tubule, sodium is reabsorbed by co-transport together with glucose, amino acids, and different solutes. However, in the second half of the proximal tubule, little glucose and few amino acids stay to be reabsorbed. The second half of the proximal tubule has a relatively excessive concentration of chloride (140 mEq/L) in contrast with the early proximal tubule (105 mEq/L) because when sodium is reabsorbed, it preferentially carries with it glucose, bicarbonate, and natural ions in the early proximal tubule, leaving behind an answer that has a higher focus of chloride. In the second half of the proximal tubule, the upper chloride focus favors diffusion of this ion from the tubule lumen via the intercellular junctions into the renal interstitial fluid. Smaller quantities of chloride can also be reabsorbed via particular chloride channels in the proximal tubular cell membrane. The proximal tubule epithelial cells are highly metabolic and have giant numbers of mitochondria to help powerful active transport processes. In addition, the proximal tubular cells have an in depth brush border on the luminal (apical) side of the membrane, in addition to an extensive labyrinth of intercellular and basal channels, all of which collectively present an in depth membrane floor space on the luminal and basolateral sides of the epithelium for rapid transport of sodium ions and other substances. Although the quantity of sodium within the tubular fluid decreases markedly alongside the proximal tubule, sodium concentration (and total osmolarity) stays comparatively fixed because water permeability of the proximal tubules is so nice that water reabsorption keeps tempo with sodium reabsorption. Certain organic solutes, corresponding to glucose, amino acids, and bicarbonate, are much more avidly reabsorbed than water, and their concentrations decrease markedly along the size of the proximal tubule. Other natural solutes which are much less permeant and not actively reabsorbed, similar to creatinine, improve their focus alongside the proximal tubule. The complete solute concentration, as mirrored by osmolarity, stays primarily the identical all along the proximal tubule because of the extremely excessive permeability of this part of the nephron to water. The proximal tubule can be an important website for secretion of organic acids and bases corresponding to bile salts, oxalate, urate, and catecholamines. Many of these substances are the tip products of metabolism and should be rapidly faraway from the physique. The secretion of these substances into the proximal tubule plus filtration into the proximal tubule by the glomerular capillaries and virtually total lack of reabsorption by the tubules, all mixed, contribute to fast excretion within the urine. In addition to the waste products of metabolism, the kidneys secrete many doubtlessly dangerous medicine or toxins into the tubules and rapidly clear these substances from the blood. In the case of sure drugs, such as penicillin and salicylates, the rapid clearance by the kidneys creates a challenge in maintaining a therapeutically effective drug focus. The descending part of the thin phase of the loop of Henle is very permeable to water and reasonably permeable to most solutes however has few mitochondria and little or no lively reabsorption. The thick ascending limb of the loop of Henle reabsorbs about 25% of the filtered a nice deal of sodium, chloride, and potassium, as properly as giant quantities of calcium, bicarbonate, and magnesium. The descending part of the skinny phase is highly permeable to water and reasonably permeable to most solutes, together with urea and sodium. The perform of this nephron section is especially to enable easy diffusion of gear by way of its partitions. About 20% of the filtered water is reabsorbed in the loop of Henle, and almost all of this occurs within the thin descending limb. About 25% of the filtered a nice deal of sodium, chloride, and potassium are reabsorbed within the loop of Henle, principally in the thick ascending limb. The 1-sodium, 2-chloride, 1-potassium co-transporter in the luminal membrane transports these three ions from the tubular lumen into the cells, using the potential vitality launched by the diffusion of sodium down an electrochemical gradient into the cells. Sodium is also transported into the tubular cell by sodium-hydrogen countertransport. The positive cost (+8 mV) of the tubular lumen relative to the interstitial fluid forces cations such as Mg2+ and Ca2+ to diffuse from the lumen to the interstitial fluid through the paracellular pathway. There is also significant paracellular reabsorption of cations, similar to Mg2+, Ca2+, Na+, and K+, in the thick ascending limb because of the slight constructive charge of the tubular lumen relative to the interstitial fluid. This positive charge forces cations corresponding to Mg2+ and Ca2+ to diffuse from the tubular lumen by way of the paracellular house and into the interstitial fluid. The thick phase of the ascending loop of Henle is virtually impermeable to water. Therefore, many of the water delivered to this segment stays within the tubule, regardless of reabsorption of large quantities of solute. The subsequent a half of the distal tubule is very convoluted and has lots of the same reabsorptive characteristics of the thick segment of the ascending limb of the loop of Henle. That is, it avidly reabsorbs most of the ions, including sodium, potassium, and chloride, however is virtually impermeable to water and urea. Approximately 5% of the filtered load of sodium chloride is reabsorbed within the early distal tubule. Chloride diffuses out of cell into the renal interstitial fluid by way of chloride channels in the basolateral membrane. The thiazide diuretics, which are broadly used to deal with issues similar to hypertension and heart failure, inhibit the sodium-chloride co-transporter. The low intracellular sodium concentration in flip supplies a positive gradient for movement of sodium from the tubular fluid into the cell. This co-transport protein within the luminal membrane makes use of the potential energy launched by downhill diffusion of sodium into the cell to drive the reabsorption of potassium into the cell in opposition to a focus gradient.
References - Mitra AP, Bartsch CC, Bartsch G, et al: Does presence of squamous and glandular differentiation in urothelial carcinoma of the bladder at cystectomy portend poor prognosis? An intensive case-control analysis, Urol Oncol 32:117n127, 2014.
- Lucas MG, Bosch RJ, Burkhard FC: at al; European Association of Urology. EAU guidelines on surgical treatment of urinary incontinence, Actas Urol Esp 37:459n472, 2013.
- Smit SG, Heyns CF: Management of radiation cystitis, Nat Rev Urol 7:206-214, 2010.
|
|