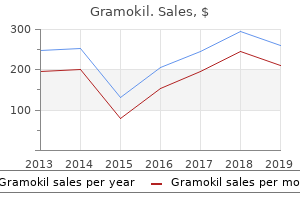
"Best purchase for gramokil, antibiotics for nasal sinus infection."By: Danielle Marie Brander, MD - Assistant Professor of Medicine
- Member of the Duke Cancer Institute
 https://medicine.duke.edu/faculty/danielle-marie-brander-md
Purchase gramokil american expressThe excessive density of actin filaments and the extensive cross-linking sample imparts rigidity and stiffness to the shaft of the stereocilium. The shaft tapers at its proximal finish near the apical surface of the cell, where the core filaments of each stereocilium are anchored throughout the terminal internet (cuticular plate). When stereocilia are deflected, they pivot at their proximal ends like stiff rods. Transmission electron microscope examination of the distal free finish of the stereocilium reveals an electron-dense plaque on the cytoplasmic website of the plasma membrane. The molecular constructions of the transduction K channels and tip hyperlinks are as but unknown. Individual stereocilia are also connected by a variety of fibrillar extracellular cross-links. A mutation that disrupts the gene that produces espin causes cochlear and vestibular symptoms in experimental mice. They lose their hearing early in life; these animals additionally spend most of their time strolling or spinning in circles. All hair cells of the internal ear seem to operate by transferring (pivoting) their rigid stereocilia. Mechanoelectric transduction occurs in stereocilia that are deflected towards its tallest edge (toward the kinocilium, if present). This movement exerts pressure on the fibrillar tip links, and the generated pressure is used to open mechanically gated ion channels close to the tip of the stereocilium. This depolarization ends in the opening of voltage-gated Ca2 channels in the basolateral surface of the hair cells and the secretion of a neurotransmitter that generates an action potential in afferent nerve endings. The means by which stereocilia are deflected varies from receptor to receptor; these are mentioned within the sections describing every receptor area. Hair cells communicate with afferent nerve fibers by way of ribbon synapses, a specialised type of chemical synapse. Deflection of the stereocilia on hair cells generates a excessive price of prolonged impulses that are shortly transmitted to the afferent nerve fibers. To secure speedy release of the glutamate neurotransmitter from synaptic vesicles, hair cells possess specialized ribbon synapses that comprise unique organelles known as ribbons. In electron microscopy, ribbons appear as ovoid, 30-nm-thick, electron-dense plates which might be anchored to the presynaptic membrane by electron-dense structures. This allows the ribbons to float just above the presynaptic plate like balloons on a short leash. The ribbons tether a massive number of synaptic vesicles on their floor which are primed for fusion with the presynaptic membrane, which contains a high density of voltage-gated Ca2 channels. After activation of the Ca2 channels, the ribbon serves as a fast-moving conveyor belt, delivering the vesicles to the presynaptic membrane for fusion. The tethered pool of synaptic vesicles is roughly fivefold greater than the pool of the remaining vesicles. These ribbon synapses are additionally discovered within the photoreceptors and bipolar cells of the retina. Diagram on the left reveals a sort I hair cell with a quantity of ribbon synapses which might be specialized for transmitting long-lasting and high-volume impulses to the afferent nerve cell endings (yellow). The surface of the ribbon serves because the tethering platform for a number of synaptic vesicles. Note the presence of voltage-sensitive Ca2 channels in the presynaptic membrane next to the attachment of the ribbon. Upon inflow of Ca2, the ribbon accelerates movement of the attached vesicles toward the presynaptic membrane for fusion (similar to the action of a fast-moving conveyor belt). This electron micrograph of a ribbon synapse from a mouse cochlear hair cell reveals the ribbon protein advanced with hooked up synaptic vesicles. The maculae of the saccule and utricle are sensors of gravity and linear acceleration. Sensory Receptors of the Membranous Labyrinth Cristae ampullaris are sensors of angular movements of the head. Each ampulla of the semicircular duct contains a crista ampullaris, which is a sensory receptor for angular movements of the top. A gelatinous protein�polysaccharide mass, generally known as the cupula, is connected to the hair cells of every crista. During rotational motion of the head, the partitions of the semicircular canal and the membranous semicircular ducts transfer, but the endolymph contained inside the ducts tends to lag behind because of inertia. The cupula, projecting into the endolymph, is swayed by the motion differential between the crista fixed to the wall of the duct and the endolymph. Deflection the maculae of the saccule and utricle are innervated sensory thickenings of the epithelium that face the endolymph of the saccule and utricle. The maculae of the utricle and saccule are oriented at proper angles to each one other. When a person is standing, the macula of the utricle is in a horizontal aircraft, and the macula of the saccule is in a vertical airplane. Hair cells are polarized with respect to the striola, an imaginary airplane that curves via the middle of each macula. On each side of the striola, the kinocilia of the hair cells are oriented in opposite instructions, facing towards the striola within the utricle and turning away from the striola within the saccule. Due to polarization of the hair cells, the maculae of the saccule and utricle are sensitive to multiple instructions of linear accelerations. The gelatinous polysaccharide materials that overlies the maculae is recognized as the otolithic membrane. As proven on this drawing, the crista ampullaris functions as the sensor for angular motion of the head. For example, when the pinnacle of the individual shown on this diagram rotates towards the left aspect, the bony labyrinth also rotates on the similar velocity together with the head. Because the crista ampullaris is attached to the wall of the bony labyrinth, it goes to be swayed by the lagging endolymph in the reverse direction to the movement of the pinnacle. The structure of the crista ampullaris contains sensory epithelium and huge cupula made from a gelatinous protein�polysaccharide mass that initiatives towards the nonsensory wall of the ampulla. Note that the membranous ampulla is filled with endolymph and is surrounded by perilymph. Their mechanical deflection opens the K channels, inflicting depolarization of the cell. This low-magnification view of a horizontal section of the temporal bone reveals several areas of the interior ear. The outstanding cochlea accommodates a well-preserved cochlear duct with a cochlear nerve rising from the base of the modiolus. The central cavity of the slide represents the vestibule that accommodates three components of the membranous labyrinth: the utricle, saccule, and ampulla of the anterior semicircular canal. The places of sensory receptors (macula of utricle, macula of saccule, and crista ampullaris) are enclosed inside the rectangles. This high-magnification view of the crista ampullaris from the anterior semicircular canal shows a thick sensory epithelium that accommodates two kinds of cells: the hair cells within the upper layer and the supporting cells within the basal layer.
Buy gramokil 250mg low costEach cavity or chamber communicates anteriorly with the exterior setting through the anterior nares (nostrils); posteriorly with the nasopharynx through the choanae; and laterally with the paranasal sinuses and nasolacrimal duct, which drains tears from the attention into the nasal cavity. Larynx that may be a hollow tubular organ containing the cartilaginous framework liable for producing sounds. It serves as a conduit for air, and in the mediastinum, it bifurcates into paired major bronchi. Within the lungs, the main bronchi bear extensive branching to give rise ultimately to the distributing bronchioles. Collectively, the internal bronchi and the bronchioles represent the bronchial tree. The respiratory portion is that part of the respiratory tract in which gasoline trade occurs. Sequentially, it contains these: � � � Nasal vestibule, which is a dilated house of the nasal cavity simply inside the nostrils and is lined by pores and skin Respiratory region, which is the largest half (inferior two-thirds) of the nasal cavities and is lined by respiratory mucosa Olfactory region, which is situated on the apex (upper one-third) of every nasal cavity and is lined by specialized olfactory mucosa � � � � Vestibule of the Nasal Cavity the nasal vestibule forms a half of the exterior nose and communicates anteriorly with the exterior environment. Sebaceous glands are also current, and their secretions help within the entrapment Respiratory bronchioles which may be concerned in both air conduction and gasoline change. Alveolar ducts that are elongated airways shaped from the confluence openings to alveoli. It is situated posterior to the nasal and oral cavities and extends inferiorly past the larynx. This midsagittal part additionally transects the cartilages forming the skeleton of the larynx. Note the ventricular and vocal folds in the course of the larynx, approximately on the degree of the thyroid cartilage. This part of the larynx represents the narrowest portion of the respiratory system and is responsible for producing sound by audible vibration of the vocal folds. Posteriorly, the place the vestibule ends, the stratified squamous epithelium turns into thinner and undergoes a transition to the pseudostratified epithelium that characterizes the respiratory area. It is lined by the respiratory mucosa that accommodates a ciliated, pseudostratified columnar epithelium on its floor. The underlying lamina propria is firmly connected to the periosteum and perichondrium of the adjacent bone or cartilage. The medial wall of the respiratory region, the nasal septum, is smooth, however the lateral partitions are thrown into folds by the presence of three shelf-like, bony projections called conchae or turbinates. The conchae divide each nasal cavity into separate air chambers and play a twin position. They increase floor area and cause turbulence in airflow to enable more environment friendly conditioning of inspired air. The ciliated, pseudostratified columnar epithelium of the respiratory mucosa consists of 5 cell sorts: the epithelium of the respiratory region of the nasal cavity is actually the identical as the epithelium lining a lot of the parts that follow in the conducting system. Because the respiratory epithelium of the trachea is studied and examined in preference to that of the nasal cavity, the above cell varieties are mentioned within the part on the trachea (page 670). The association of the vessels allows the inhaled air to be warmed by blood flowing through the part of the loop closest to the surface. The capillaries that reside close to the floor are arranged in rows; the blood flows perpendicular to the airflow, a lot as one would discover in a mechanical heatexchange system. These similar vessels may turn out to be engorged and leaky throughout allergic reactions or viral infections such because the widespread chilly. The lamina propria then becomes distended with fluid, leading to marked swelling of the mucous membrane with consequent restriction of the air passage, making breathing troublesome. Their secretions supplement that of the goblet cells within the respiratory epithelium. By increasing surface space, the conchae (turbinates) enhance the effectivity with which the inspired air is warmed. The turbinates additionally enhance the efficiency of filtration of impressed air via the process of turbulent precipitation. Particulate matter suspended in the air stream is thrown out of the stream and adheres to the mucus-covered wall of the nasal cavity. Particles trapped in this layer of mucus are transported to the pharynx by the use of coordinated sweeping movements of cilia and are then swallowed. The lamina propria of the olfactory mucosa is directly contiguous with the periosteum of the underlying bone (Plate 69, page 688). This connective tissue incorporates numerous blood and lymphatic vessels, unmyelinated olfactory nerves, myelinated nerves, and olfactory glands. The olfactory epithelium, like the epithelium of the respiratory region, is also pseudostratified, but it accommodates very completely different cell sorts. In dwelling tissue, this mucosa is distinguished by its slight yellowish brown shade brought on by pigment in the olfactory epithelium and the related olfactory glands. In people, the entire floor space of the olfactory mucosa is just about 10 cm2; in animals with an acute sense of odor, the total floor space of the olfactory mucosa is � � � � Olfactory receptor cells are bipolar olfactory neurons that span the thickness of the epithelium and enter the central nervous system. Supporting or sustentacular cells are columnar cells which might be much like neuroglia cells and supply mechanical and metabolic assist to the olfactory receptor cells. Basal cells are stem cells from which new olfactory receptor cells and supporting cells differentiate. This diagram reveals the three major cell types positioned inside the olfactory epithelium: the olfactory cell, supporting (sustentacular) cell, and basal cell. The olfactory cell is the receptor cell; it has an apical enlargement, the olfactory vesicle, from which long, nonmotile cilia lengthen. At its basal surface, it extends an axon into the connective tissue that joins with axons of different olfactory cells to kind an olfactory nerve. The supporting cells, in contrast, are columnar and extend the total thickness of the epithelium; their nuclei are located within the upper portion of the cell. Note that the ducts of the olfactory glands lengthen from the secretory portion of the gland to the epithelial surface. Supporting cells provide mechanical and metabolic assist for the olfactory receptor cells. A number of lengthy, thin cilia (10 to 23) with typical basal our bodies arise from the olfactory vesicle and prolong radially in a airplane parallel to the epithelial floor. The cilia are often up to 200 m long and may overlap with cilia of adjacent olfactory receptor cells. The cilia are thought to be nonmotile, although some research means that they might have restricted motility. The basal domain of the cell gives rise to an unmyelinated axonal process that leaves the epithelial compartment. The collections of axons from olfactory receptor cells form the olfactory nerve (cranial nerve I).
Best purchase for gramokilThe solely growth of the ovary that produces uterine haemorrhage is the granulosa-cell tumour and will occur at almost any age (see Ovarian swellings). In girls with postmenopausal bleeding, ultrasound scanning to measure the endometrial thickness may be a helpful approach to triage these patients. If the endometrial thickness is 5 mm or much less, then no additional action is needed unless the bleeding continues. However, breakthrough bleeding can occur owing to gastrointestinal upset, absorption and metabolism problems due to other medications. When this is accompanied by lower abdominal ache (mittelschmerz), the analysis is simple. Bleeding due to granulosa-cell tumour When irregular bleeding occurs in the presence of an ovarian swelling, the potential for a granulosa-cell tumour arises. The secretory or luteal section is the time from ovulation to menstruation, which is usually fixed at 14 days. There are several situations that result in oligomenorrhoea, and these range from regular circumstances (for a particular woman) to the same conditions that cause amenorrhoea (see Menstrual durations, absent). Some frequent causes are: Polycystic ovarian syndrome, which accounts for about 90 per cent of cases of oligomenorrhoea compared with solely 33 per cent of amenorrhoea. In this case, the menstrual intervals are normally mild and the lady may not ovulate (anovulation). It typically occurs in adolescent girls or at the time of menarche, and in older women within the perimenopausal section. Clinically, oligomenorrhoea should be thought of in the same method as amenorrhoea for the purpose of investigations and additional management. This section ought to be read in conjunction with Menstrual intervals, heavy and/or irregular. Primary dysmenorrhoea occurs when the durations are painful and no organic or psychological trigger could be discovered. It often happens initially of reproductive life when the woman begins ovulating, approximately 6�12 months after menarche. The ache starts with the onset of menstruation and is mostly associated with ovulatory cycles. There is an abnormally excessive production of endometrial prostaglandins, which causes extreme uterine contractions. Examination findings are normally regular, and further investigation may be essential provided that treatment fails to alleviate the signs. Secondary dysmenorrhoea occurs when the girl experiences painful intervals where an organic or psychosexual trigger may be discovered. It is a symptom advanced which incorporates cramping lower abdominal ache radiating to the again and legs, and is often related to gastrointestinal upset, malaise, and headaches. By simple statistical extrapolation, the possibility of a woman having three sporadic miscarriages in a row is 0. On the opposite hand, early miscarriages may be coupled with a late fetal demise in patients with either congenital or acquired thrombophilia. A previous history of cone biopsy or other excision procedures for cervical intraepithelial neoplasia may recommend the chance of cervical stenosis, which may require dilatation of the cervix. An ultrasound scan may be useful, especially if vaginal examination is troublesome or painful. In many cases, laparoscopy may be indicated to exclude a selected pathology, particularly endometriosis. If no pelvic pathology is discovered, the remedy may be as for major dysmenorrhoea. If adhesions, endometriosis, or intrauterine pathology is discovered, hormonal preparations or surgery, or both, may be required. Miscellaneous Laboratory criteria include detection of both lupus anticoagulant or anticardiolipin antibodies or both. The autosomal trisomies generally encountered are those of chromosomes 3, 4, 9, 13�16, 19, 21, and 22. Antibodies are directed against negatively charged phospholipids, that are the most important constituents of trophoblasts. There is an ultrasound affirmation of a viable pregnancy previous to the being pregnant loss in most first trimester losses. Dicentric and ring chromosomes are mitotically unstable, so the possibilities of offspring acquiring these anomalies are very small. In men with balanced translocations, the reproductive potential is simply barely diminished. In unbalanced translocations in men, not only is the reproductive efficiency significantly decreased, but in addition the danger of irregular offspring is elevated. Polycystic ovarian syndrome is likely one of the commonest endocrinal abnormalities affecting feminine reproductive efficiency. Besides infertility, it presents higher risks of first- and second-trimester miscarriages. Women with poorly managed type 1 (insulindependent) diabetes mellitus with glycosylated haemoglobin levels larger than eight standard deviations above the mean have the next being pregnant loss rate. Abnormal maternal thyroid capabilities have been implicated as a cause of recurrent miscarriage. Although uncommon, the affected person with an untreated adrenal hyperplasia might have an increased chance of recurrent miscarriage owing to hyperandrogenism. Premature ovarian failure remains an essential factor liable for recurrent miscarriage, owing to declining ovarian perform and poor quality oocytes. They cause insufficient placental circulation owing to thrombosis within the placental vasculature, and lead to opposed pregnancy outcomes corresponding to recurrent miscarriage, fetal dying, and placental abruption. Pregnancy in a rhesus-sensitised lady with a excessive titre of anti-D antibodies will also end in recurrent pregnancy losses. Systemic infections similar to syphilis, had been an essential reason for recurrent miscarriage prior to now. An estimated 15 per cent of couples (one in six) with recurrent miscarriage have an anatomic abnormality of their uterus as the first cause. An irregular cytokine setting may be responsible for a few of the hitherto unexplained recurrent miscarriages. Genital infections Genitourinary tuberculosis is classically associated with infertility however latent an infection can also cause recurrent ectopic being pregnant as properly as recurrent miscarriages. Bacterial vaginosis is now implicated in recurrent miscarriages, recurrent preterm labour, and preterm untimely rupture of membranes. Obstetric implications of antiphospholipid antibodies: being pregnant loss and different problems. Retrospective and potential epidemiological studies of 1500 karyotyped spontaneous human abortions.
Buy gramokil 500mg amexHowever, no less than 50 per cent could have a less dramatic onset with a progressive, severe, unremitting headache. This is caused by the rupture of either an arteriovenous malformation or a saccular or berry aneurysm. It is a broadly held belief that subarachnoid haemorrhage is more widespread in being pregnant, but that is unlikely. Subarachnoid haemorrhage accounts for 50 per cent of cerebral haemorrhages in pregnancy, occurring in 1 in 10,000 pregnancies with a 50 per cent maternal mortality. It also presents with sudden, extreme headache, typically accompanied by quickly progressive neurological signs. However, the deteriorating medical state of the mom usually requires speedy neurosurgical intervention and supply of Tension-type complications In comparison to migraines, tension-type headaches have few attribute features. Postpartum headache About forty per cent of ladies develop headache within the first week postpartum. Another major cause of postpartum headache is inadvertent dural puncture, which occurs in about 1�2 per cent of ladies throughout lumbar epidural insertion. About 15 per cent of women may also complain of headache following obstetric spinal anaesthesia. The headache is comparable in each and is normally tolerable when the girl is mendacity down. The dramatic impact of posture in the context of a historical past of spinal or epidural anaesthesia/analgesia often makes the analysis straightforward. Cerebral venous thrombosis Although rare, the danger of stroke in younger ladies increases 13-fold in being pregnant with the most typical trigger being cerebral venous thrombosis. It is thought to be extra frequent in hypercoagulable states such as underlying thrombophilia and preeclampsia. The usual presentation is with focal neurological signs and indicators, but thrombosis of the superior sagittal sinus is reported to cause extreme progressive headache without focal indicators. It may be associated with the development of hypertension, which can delay the analysis as a outcome of the neurological condition is incorrectly attributed to pre-eclampsia. Benign intracranial hypertension Benign intracranial hypertension is 10 occasions extra common in obese ladies of childbearing age in comparison with the final population. Women may already have the situation after they turn into pregnant, or it could develop anew during pregnancy. It may be due to increased manufacturing or impaired resorption of cerebrospinal fluid. It presents with a global headache that might be worse lying down, and with progressive diplopia and visual loss if untreated. On testing, diplopia and papilloedema shall be present, and there may be impairment of visual fields and acuity. If the prognosis continues to be not clear, lumbar puncture might be necessary to reveal an abnormally raised opening strain. Systemic and other conditions Headache can occur in a wide range of different medical conditions in pregnancy. Examples embody hypoglycaemia with the therapy of diabetes and fever due to any intercurrent an infection. Headaches are also seen with using, and withdrawal from, illicit medicine corresponding to amphetamines, cocaine, barbiturates, and opiates. Daily headaches attributed to treatment overuse could be the prognosis, if a drug is used for signs most days, and in the absence of any worrying options and with a traditional examination. This could be particularly problematic when the girl has problem in sleeping owing to her increasing abdominal size and discomfort or the presence of other young children in the household. The scenario is compounded by the rising measurement of the gravid uterus causing strain on the abdomen, thus symptoms often worsen in the third trimester of being pregnant. The majority of women presenting with these signs may be confidently recognized with out want for particular investigations. This can embody utilizing an additional pillow at night time, avoiding large meals and spicy food particularly late at night time, carrying unfastened becoming garments, and avoiding stooping. Cabbage, broccoli, and lettuce are all excessive in raffinose, a sugar that produces gasoline in the abdomen, which may aggravate symptoms and may only be taken carefully. Many women find rest strategies, natural medicines, acupuncture, acupressure, aromatherapy, and homeopathy useful. Use of the smallest dose to obtain symptom control is the therapeutic aim; subsequently, in contrast to the non-pregnant girl, the drug treatment in pregnancy ought to comply with a step-up algorithm. Antacids and sucralfate (an aluminium-containing compound) are thought-about the first-line drug remedy. However, utilizing them too typically and for too lengthy can cause constipation (if they comprise aluminium) or diarrhoea (if they contain magnesium). Women must be suggested to take antacids at a unique time from once they take oral iron dietary supplements, as hydrochloric acid is required for iron absorption. Sucralfate is also poorly absorbed, inhibits pepsin and regionally protects towards ulcers. Alginates are used for the symptomatic remedy of heartburn and oesophagitis, and seem to act by a novel mechanism, which differs from traditional antacids. Gaviscon is an alginate, which within the presence of gastric acid precipitates to type a gel. Both in vitro and in vivo studies have demonstrated that alginate-based rafts can entrap carbon dioxide, thus providing a comparatively pH-neutral barrier. Metoclopramide acts by growing the pressure within the region of the lower oesophageal sphincter in addition to rising clearance from each the oesophagus and the stomach. No teratogenic unwanted facet effects have been reported with this drug, which has been used extra generally within the therapy of hyperemesis gravidarum. Histamine-2 receptor antagonists include cimetidine, famotidine, and nizatidine along with ranitidine. Ranitidine is the only drug that has been specifically studied for use in the pregnant girl. It is related to vital symptom rating enchancment and no particular teratogenic unwanted facet effects. Of this group, lansoprazole may be most popular due to its security profile in animals and case reviews of safety in human pregnancies. Most drugs are excreted in breast milk, and only the histamine-2 receptor antagonists (with the exception of nizatidine) are secure to use in lactation. Androgens, notably testosterone, initiate growth and improve the diameter and pigmentation of hair. Oestrogens basically act within the opposite approach to androgens, and progestins have minimal direct effects on hair. Once the transformation from vellus to terminal hair happens, the terminal growth pattern persists, even if the increased androgen levels stop. The concentration of hair follicles laid down per unit area of facial skin differs little between women and men, but does differ between races and ethnic teams.
Diseases - Otoonychoperoneal syndrome
- Deafness skeletal dysplasia lip granuloma
- 47, XYY syndrome
- Meningeal angiomatosis cleft hypoplastic left heart
- Papilloma of choroid plexus
- Chromosome 16, trisomy 16q
- Fitz-Hugh Curtis syndrome
- Cousin Walbraum Cegarra syndrome
Generic gramokil 250 mg with visaThis larger magnification photomicrograph shows viral particles stained purple throughout the nuclei of contaminated cells. Lactation is under the neurohormonal control of the adenohypophysis and hypothalamus. Immediately after start, nonetheless, the sudden loss of estrogen and progesterone secretion from the placenta and corpus luteum permits prolactin to assume its lactogenic function. Production of milk additionally requires adequate secretion of development hormone, adrenal glucocorticoids, and parathyroid hormones. The act of suckling throughout breast-feeding initiates sensory impulses from receptors in the nipple to the hypothalamus. The impulses inhibit the release of prolactin-inhibiting issue, and prolactin is then launched from the adenohypophysis. Oxytocin stimulates the myoepithelial cells that encompass the base of the alveolar secretory cells and the bottom of the cells within the bigger ducts, inflicting them to contract and eject the milk from the alveoli and the ducts. Ovulation usually resumes after 6 months or earlier with a lower in suckling frequency. In cultures in which breast-feeding might continue for 2 to three years, lactational amenorrhea is the principal means of birth control. In the absence of suckling, secretion of milk ceases, and the mammary glands begin to regress and atrophy. Female Reproductive System Involution of the Mammary Gland the mammary gland atrophies or its specialised stroma involutes after menopause. The connective tissue additionally demonstrates degenerative changes, marked by a decrease within the number of fibroblasts and collagen fibers, and lack of elastic fibers. Branches of the vessels cross primarily alongside the path of the alveolar ducts as they attain capillary beds surrounding the alveoli. Veins basically observe the path of the arteries as they return to the axillary and internal thoracic veins. Lymphatic capillaries are positioned within the connective tissue surrounding the alveoli. The larger lymphatic vessels drain into axillary, supraclavicular, or parasternal lymph nodes. Innervation the nerves that provide the breast are anterior and lateral cutaneous branches from the second to sixth intercostal nerves. The secretory perform is primarily under hormonal management, but afferent impulses related to suckling are involved within the reflex secretion of prolactin and oxytocin. Ovaries have a medulla in their heart that incorporates free A rising follicle that contains a single fluid cavity (antrum) is called the secondary (antral) follicle. It nonetheless connective tissue, nerves, blood and lymphatic vessels, and a cortex on their periphery that contains numerous ovarian follicles that present a microenvironment for developing oocytes. The surface of the ovary is covered by germinal epithelium, which is a single cuboidal epithelium that overlies a dense layer of connective tissue referred to as tunica albuginea. There are three fundamental developmental stages of an ovarian follicle: primordial, rising (both major and secondary), and mature (Graafian) follicle. After puberty following cyclic hormonal adjustments, a particular cohort of primary follicles develops into rising follicles. Follicular cells surrounding the oocyte become cuboidal and bear additional stratification to form the first follicle. As granulosa cells proliferate, they turn into involved in steroid hormone metabolism (conversion of androgens produced by theca interna into estrogens) and are actively secreting follicular fluid that accumulates in cavities between the granulosa cells. The mature (Graafian) follicle has a large antrum and a distinguished, steroid-producing theca interna layer. All different follicles in the creating cohort undergo follicular atresia, a means of degeneration involving apoptosis. During ovulation, a secondary oocyte is launched from the ruptured Graafian follicle. At ovulation, the follicular wall, composed of the remaining granulosa and thecal cells, is reworked into the corpus luteum. The corpus luteum of menstruation is shaped within the absence of fertilization; it degenerates 10 to 12 days after ovulation to become the corpus albicans. During capacitation, the mature spermatozoa acquire the flexibility to fertilize the oocyte within the feminine reproductive tract. After capacitation, the spermatozoa bind to the zona pellucida receptors, which trigger the acrosome reaction. Enzymes launched from the acrosome permit a single spermatozoon to penetrate the zona pellucida and impregnate the oocyte. During impregnation, the entire spermatozoon, apart from the tail cytoplasm, becomes incorporated into the ooplasm, which triggers resumption of the second meiotic division (transforms the secondary oocyte right into a mature oocyte). The sperm head inside the oocyte cytoplasm undergoes modifications to form the male pronucleus, which fuses with the female pronucleus to kind a diploid zygote. Each uterine tube has four segments: infundibulum (a funnel-shaped finish surrounded by fimbriae adjacent to the ovary), ampulla (common web site of fertilization), isthmus (narrow segment adjacent to the uterus), and intramural part (traversing the uterine wall). The uterine tube wall consists of three layers: exterior serosa, thick muscularis, and highly folded mucosa. The mucosal lining is straightforward columnar epithelium composed of two cell types: ciliated and nonciliated (peg) cells. The oocyte (and zygote after fertilization) is propelled into the uterine cavity by a coordinated motion of cilia on the floor of mucosa and peristaltic muscular contractions of the uterine tube. The uterine wall is composed of endometrium (lining mucosa of the uterus), myometrium (smooth muscular layer), and perimetrium (a serous layer of visceral peritoneum). The endometrium is lined by easy columnar epithelium that invaginates into the underlying lamina propria (endometrial stroma), forming uterine glands. The endometrium consists of stratum basale and stratum functionale, which undergoes cyclic adjustments as a result of fluctuat- ing levels of estrogens and progesterone during the menstrual cycle. The thickness of the endometrium, its glandular exercise, and its vascular sample are distinctive for each of the three phases (proliferative, secretory, and menstrual) of the menstrual cycle, which lasts a median of 28 days. If the embryo implants successfully, the endometrium undergoes decidualization (the process of conversion to decidua) and along with the trophoblastic cells from the embryo initiate improvement of the placenta. The a half of the cervix projecting into the vagina has a transformation zone where easy columnar epithelium of the cervix modifications abruptly into stratified squamous epithelium of the vagina. Fetal and maternal blood is separated by the placental barrier, which develops in the tertiary chorionic villi (projections of chorion containing syncytiotrophoblast, cytotrophoblast, mesenchymal connective tissue, and fetal blood vessels). Villi are immersed in the maternal blood that fills vascular areas in the placenta (cotyledons). The placenta is a significant endocrine organ that supports improvement of the fetus; it produces each steroid hormones (mainly progesterone) and protein hormones. Female exterior genitalia (vulva) include the mons pubis (formed by underlying adipose tissue), labia majora (longitudinal folds of skin containing adipose tissue, a thin layer of clean muscle, and sebaceous and sweat glands), labia minora (core of connective tissue devoid of adipose tissue but contains large sebaceous glands), clitoris (erectile tissue homologous to the penis), and vestibule (lined with stratified squamous epithelium with quite a few small mucous glands). The morphology of the secretory portion of the inactive mammary gland varies with the menstrual cycle. Mammary glands bear dramatic proliferation and development during pregnancy in preparation for lactation underneath the affect of estrogen (proliferation of duct components) and progesterone (growth of alveoli).
Buy generic gramokil on lineConductive listening to loss outcomes when sound waves are mechanically impeded from reaching the auditory sensory receptors within the inside ear. This type of hearing loss principally involves the external ear or constructions of the middle ear. Conductive listening to loss is the second commonest sort of loss after sensorineural listening to loss, and it usually includes a discount in sound stage or the lack to hear faint sounds. A conductive listening to loss may be attributable to otitis media (ear infection); actually, this is the most typical explanation for momentary listening to loss in children. Fluid that collects in the tympanic cavity also can trigger important hearing issues in kids. Other frequent causes of conductive listening to loss include excess wax or international bodies within the external acoustic meatus or illnesses that have an effect on the ossicles in the middle ear (otosclerosis; see additionally Folder 25. In many cases, conductive listening to loss can be treated either medically or surgically and will not be everlasting. Causes of acquired sensorineural hearing loss embrace infections of the membranous labyrinth. Sensorineural hearing loss not solely entails a reduction in sound degree but additionally impacts the power to hear clearly or to distinguish speech. A lack of the sensory hair cells or related nerve fibers begins within the basal flip of the cochlea and progresses apically over time. The attribute impairment is a high-frequency listening to loss termed presbycusis (see presbyopia, page 922). In chosen sufferers, the use of a cochlear implant can partially restore some listening to operate. The cochlear implant is an electronic system consisting of an exterior microphone, amplifier, and speech processor linked to a receiver implanted underneath the pores and skin of the mastoid area. The receiver is related to the multielectrode intracochlear implant inserted along the wall of the cochlear canal. This larger magnification photomicrograph of the cochlear duct exhibits the structure of the spiral organ of Corti. Relate this structure to the inset, which labels the structural options of the spiral organ. The sensory cells are divided into an internal row of sensory hair cells and three rows of outer sensory hair cells. The tectorial membrane extends from the spiral limbus over the cells of the spiral organ of Corti. The phalangeal cells associated with the inside hair cells surround the cells completely. The phalangeal cells related to the outer hair cells surround only the basal portion of the hair cell utterly and ship apical processes towards the endolymphatic area. These processes flatten near the apical ends of the hair cells and collectively type an entire plate surrounding each hair cell. The apical ends of the phalangeal cells are tightly sure to each other and to the hair cells by elaborate tight junctions. These junctions type the reticular lamina that seals the endolymphatic compartment from the true intercellular spaces of the organ of Corti. Its composition is just like that of different extracellular fluids and to perilymph. Pillar cells have broad apical and basal surfaces that type plates and a narrowed cytoplasm. The inside pillar cells relaxation on the tympanic lip of the spiral lamina; the outer pillar cells rest on the basilar membrane. Its lateral free edge tasks over and attaches to the organ of Corti by the stereocilia of the hair cells. Glycoproteins unique to the internal ear, referred to as otogelin and tectorin, are related to the collagen bundles. These proteins are also present in the otolithic membranes overlying the maculae of the utricle and saccule in addition to within the cupulae of the cristae in the semicircular canals. Sound Perception As described on page 937, sound waves striking the tympanic membrane are translated into easy mechanical vibrations. In the internal ear, the vibrations of the ossicles are transformed into waves in the perilymph. Movement of the stapes in the oval window of the vestibule units up vibrations or traveling waves within the perilymph of the scala vestibuli. Movement of the stereocilia of the hair cells within the cochlea initiates neuronal transduction. Hair cells are attached by way of the phalangeal cells to the basilar membrane, which vibrates throughout sound reception. The stereocilia of these hair cells are, in turn, connected to the tectorial membrane, which additionally vibrates. Thus, a shearing impact happens between the basilar membrane (and the cells hooked up to it) and the tectorial membrane when sound vibrations impinge on the inner ear. The shearing effect between the basilar membrane and the tectorial membrane deflects the stereocilia and thus the apical portion of the hair cells. Ear Innervation of the Internal Ear the vestibular nerve originates from the sensory receptors related to the vestibular labyrinth. This electron micrograph illustrates the configuration of stereocilia on the apical surfaces of the inside row and three outer rows of the cochlear sensory hair cells. Pressure adjustments in this closed perilymphatic�endolymphatic system are mirrored in movements of the membrane that covers the spherical window within the base of the cochlea. As a result of sound vibrations entering the internal ear, a traveling wave is set up within the basilar membrane. A sound of specified frequency causes displacement of a relatively lengthy section of the basilar membrane, but the area of maximal displacement is slender. The level of maximal displacement of the basilar membrane is specified for a given frequency of sound and is the morphologic basis of frequency discrimination. High-frequency sounds cause maximal vibration of the basilar membrane close to the bottom of the cochlea; low-frequency sounds cause maximal displacement nearer the apex. The vestibular nerve is associated with equilibrium and carries impulses from the sensory receptors situated within the vestibular labyrinth. The cochlear nerve is associated with hearing and conveys impulses from the sensory receptors throughout the cochlear labyrinth. The cell our bodies of the bipolar neurons of the vestibular nerve are positioned within the vestibular ganglion (of Scarpa) within the inside acoustic meatus. Dendritic processes of the vestibular ganglion cells originate in the cristae ampullaris of the three semicircular ducts, the macula of the utricle, and the macula of the saccule.
Purchase 500mg gramokilThe thyroid is unique among endocrine glands as a result of it shops large amounts of its secretory product extracellularly. The synthesis of the two main thyroid hormones, thyroxine (T4) and triiodothyronine (T3), takes place within the thyroid follicle in a series of discrete steps. From here, iodide ions are transported to the lumen of the follicle by the 86 kDa iodide/chloride transporter referred to as pendrin located within the apical cell membrane. One or two iodine atoms are then added to the precise tyrosine residues of thyroglobulin. The thyroid hormones are fashioned by oxidative coupling reactions of two iodinated tyrosine residues in shut proximity. After endocytosis, thyroglobulin follows no much less than two completely different intracellular pathways. In the lysosomal pathway, thyroglobulin is internalized and transported within endocytotic vesicles to early endosomes. Resorption of thyroglobulin at this stage may be confirmed by the presence of enormous endocytic vesicles known as colloidal resorption droplets within the apical area of the follicular cells. In the transepithelial pathway, thyroglobulin is transported intact from the apical to the basolateral surface of follicular cells. This diagram depicts two follicular cells: one within the means of thyroglobulin synthesis (on the left with pink pathways) and the opposite in the strategy of thyroglobulin resorption (on the right with blue pathways). Megalin is a transmembrane protein expressed on the apical surface of follicular epithelial cells instantly going through colloid. This pathway may scale back the extent of T4 and T3 launch by diverting thyroglobulin away from the lysosomal pathway. The majority of T4 and T3 are liberated from thyroglobulin in the lysosomal pathway, and only negligible quantities of T4 and T3 are released bound to thyroglobulin. Both T4 and T3 cross the basal membrane and enter the blood and lymphatic capillaries. Approximately less than 10% of launched hormones are sure to a nonspecific fraction of albumin, leaving only small quantities (1%) of free circulating hormones that are metabolically energetic. The free circulating hormones additionally function in the suggestions system that regulates the secretory exercise of the thyroid. The follicular cells of the thyroid gland predominately produce about 20 occasions extra T4 than T3; nevertheless, T4 is converted within the peripheral organs. Approximately 99% of T4 and T3 launched from the thyroid gland into circulation bind to specific plasma proteins. The remaining free (unbound) T4 and T3 exert adverse feedback on the system and inhibit additional launch of T4 and T3. This inhibition happens on the level of the anterior lobe of the pituitary gland and the hypothalamus. After crossing the blood�brain barrier, T4 and T3 are transferred into neighboring astrocytes, the place T4 is converted to T3. T4 and T3 are additionally secreted into the cerebrospinal fluid and are taken up by the tanycytes (specialized ependymal cells) and astrocytes, where T4 is transformed to T3. The feedback system is activated in response to low thyroid hormone levels within the blood or metabolic wants. T3 is 5 instances more potent than T4 and is principally answerable for organic activity by binding to the thyroid nuclear receptors in the goal cells. Transport across the cell membrane is essential for thyroid hormone action and metabolism. Adult hypothyroidism, previously referred to as myxedema (due to the puffy look of the skin), is characterised by mental and bodily sluggishness. The edema that happens in the severe levels of hypothyroidism is attributable to the buildup of large quantities of hyaluronan in the extracellular matrix of the connective tissue of the dermis. However, under such stimulation the thyroid gland undergoes hypertrophy, and the thyroid hormone is secreted at abnormally excessive charges, causing increased metabolism. Most of the scientific futures are associated with elevated metabolic price and elevated sympathetic nerve activities. Noticeable options embody protrusion of the eyeballs and retraction of the eyelids, resulting from elevated sympathetic exercise and elevated deposition of extracellular matrix within the adipose tissue located behind the eyeball. Microscopic options embrace the presence of columnar follicular cells lining the thyroid follicles. Because of the excessive utilization of colloid, the follicle tends to be depleted in the areas of contact with the apical floor of follicular cells. Note the enlarged mass on the neck and the standard ocular symptoms generally identified as exophthalmos. The triiodothyronine (T3) hormone is more biologically active than thyroxine (T4). T3 binds to nuclear receptors much quicker and with greater affinity than T4, thus T3 is more quickly and biologically active than T4. Therefore, biological activity and metabolic impact of the thyroid hormone is basically decided by the intracellular concentration of T3. These embody serum concentration of circulating T3, which is dependent upon the conversion price of T4 to T3 in the peripheral organs; transport of thyroid hormones across the cell membrane by specialised thyroid hormone transporters; and presence of iodothyronine deiodinase enzymes, which activate or inactivate thyroid hormones. Structurally, every parathyroid gland is surrounded by a thin connective tissue capsule that separates it from the thyroid. Septa lengthen from the capsule into the gland to divide it into poorly defined lobules and to separate the densely packed cords of cells. The connective tissue is more evident within the adult, with the event of fats cells that improve with age and in the end represent as a lot as 60% to 70% of the glandular mass. The glands receive their blood provide from the inferior thyroid arteries or from anastomoses between the superior and inferior thyroid arteries. Typical of endocrine glands, rich networks of fenestrated blood capillaries and lymphatic capillaries surround the parenchyma of the parathyroids. Parathyroid glands develop from the endodermal cells derived from the third and fourth pharyngeal pouches. Endocrine Organs Embryologically, the inferior parathyroid glands (and the thymus) are derived from the third pharyngeal pouch; the superior parathyroid glands (and ultimobranchial body) are derived from the fourth pharyngeal pouch. Initially, the inferior parathyroid glands, which derive from the superiorly positioned third pharyngeal pouch, descend with the thymus. Later, the inferior parathyroid glands separate from the thymus and come to lie beneath the superior parathyroid glands. Failure of those constructions to separate leads to the atypical association of the parathyroid glands with the thymus in the adult. The principal (chief) cells differentiate throughout embryonic growth and are functionally lively in regulating fetal calcium metabolism. Principal cells and oxyphil cells constitute the epithelial cells of the parathyroid gland. In regular being pregnant, each T3 and T4 cross the placental barrier and are crucial within the early levels of mind development.
Generic gramokil 250mg amexBottom, the multitude of inflammatory cells (macrophages, eosinophils, mast cells, neutrophils) and neurotransmitters implicated in asthma pathophysiology. In this mannequin, antigens, similar to ragweed pollen or house mite dust, sensitize people by eliciting the production of antibodies of the immunoglobulin (Ig) E sort. If the individual is reexposed to the same antigen days to months later, the resulting antigen�antibody reaction on lung mast cells will set off the discharge of histamine and the cysteinyl leukotrienes, brokers that produce bronchoconstriction, mucus secretion, and pulmonary edema. Mast cells also release a selection of chemotactic mediators, similar to leukotriene B4 and cytokines. These agents recruit and activate additional inflammatory cells, notably eosinophils and alveolar macrophages, each of that are additionally wealthy sources of leukotrienes and cytokines. Ultimately, repeated exposure to antigen establishes a chronic inflammatory state within the asthmatic airway. Pharmacotherapy of bronchial asthma is managed in a stepwise trend based on the severity of the illness. Recommendations for the stepwise remedy of asthma in adults and youngsters older than 5 years of age are proven in Table 39. Bronchodilators can produce a substantial increase in pulmonary operate by relaxing bronchial smooth muscle, thus dilating the airways. Consequently, the overall objectives of antiasthma remedy are to return lung operate to as close to regular as attainable and to forestall acute exacerbations of the disease. For quality of life, the best routine permits regular activities, including exercise, with minimal or no side effects. The main classes of drugs used to deal with asthma are bronchodilators and antiinflammatory agents. Bronchodilators embody theophylline, a variety of adrenomimetic amines, and ipratropium bromide. These agents include the leukotriene modulators, cromolyn sodium, and nedocromil sodium. Bronchodilators are used both in upkeep therapy and as wanted to reverse acute attacks. Based on the underlying pathophysiology of the illness, antiinflammatory remedy should be used in conjunction with bronchodilators in all however the mildest asthmatics. Antiinflammatory agents are additionally referred to as controllers because they provide long-term stabilization of signs. In addition to drug remedy, all treatment regimens ought to embrace affected person schooling Adrenomimetic Agents Adrenergic medicine (Table 39. These brokers are used both as wanted to reverse acute episodes of bronchospasm and prophylactically to maintain airway patency over the long run. Basic Pharmacology the final pharmacological actions of adrenomimetics are described in detail in Chapter 10. The principal pharmacological effects that might be observed in people handled for bronchospasm are bronchodilation, tachycardia, anxiety, and tremor. Stimulating 2-adrenoceptors produces all of these results both instantly or not directly. Much-improved selectivity is offered by brokers corresponding to albuterol, terbutaline, and salmeterol. These compounds have the next affinity for 2-adrenoceptors, the predominant subtype within the airway, than for 1adrenoceptors. Department of Health and Human Service, National Institutes of Health, National Heart, Lung and Blood Institute; July 1997. Metaproterenol (Alupent), another adrenomimetic used as a bronchodilator, is much less selective for 2-adrenoceptors than is albuterol or terbutaline. Epinephrine administered subcutaneously is used to manage extreme acute episodes of bronchospasm and status asthmaticus. In addition to its bronchodilator exercise by way of -adrenoceptor stimulation, a portion of the therapeutic utility of epinephrine in these acute settings could also be due to a discount in pulmonary edema because of pulmonary vasoconstriction, the latter effect resulting from -adrenoceptor stimulation. The characteristic cardiovascular effects seen at therapeutic doses of epinephrine embody elevated coronary heart rate, increased cardiac output, elevated stroke volume, an elevation of systolic pressure and reduce in diastolic strain, and a lower in systemic vascular resistance. The cardiovascular response to epinephrine represents the algebraic sum of both - and -adrenoceptor stimulation. A lower in diastolic blood strain and a decrease in systemic vascular resistance are reflections of vasodilation, a 2-adrenoceptor response. The improve in coronary heart price and systolic strain is the end result of either a direct effect of epinephrine on the myocardium, primarily a 1 effect, or a reflex action provoked by a lower in peripheral resistance, mean arterial stress, or both. Isoproterenol is administered nearly solely by inhalation from metered-dose inhalers or from nebulizers. The response to inhaled isoproterenol and different inhaled adrenomimetics is instantaneous. The motion of isoproterenol is short-lived, though an objective measurement of pulmonary function has proven an effective length of as much as 3 hours. Terbutaline and albuterol are administered either orally or by inhalation, whereas salmeterol is given by inhalation only. All three brokers are comparatively selective for 2-adrenoceptors and theoretically are able to producing bronchodilation with minimal cardiac stimulation. However, the time period 2-selectivity is a pharmacological classification based mostly primarily on the relative efficiency of a person adrenomimetic to stimulate the pulmonary or the cardiovascular system. Indeed, 2agonists invariably produce a level of tachycardia at giant doses, both by activating sympathetic reflex pathways as a consequence of systemic vasodilation or by instantly stimulating cardiac 1-adrenoceptors. In addition, a major variety of 2-adrenoceptors are present in the human heart, and stimulation of these receptors could contribute to the cardiac results of 2adrenoceptor agonists. Inhaled salmeterol has a pharmacological half-life in extra of 12 hours, much longer than both albuterol or terbutaline. The likely basis for this long half-life is that the long lipophilic tail of salmeterol promotes retention of the molecule within the cell membrane. Its lengthy period of motion makes salmeterol notably suitable for prophylactic use, such as in stopping nocturnal symptoms of asthma. This process is triggered by the interplay of the adrenomimetics with 2-adrenoceptors on airway clean muscle. Isoproterenol is used principally by inhalation for the management of bronchospasm. Terbutaline, albuterol, salmeterol and other 2adrenoceptor agonists are used primarily in the administration of asthma. Terbutaline and albuterol have very rapid onset of action and are indicated for acute symptom reduction. Salmeterol, in contrast, has a sluggish onset of action but a protracted period of action. Salmeterol is thus used as prophylactic remedy solely, not to reverse acute symptoms.
References - Dahlof, C. et al. (2001). Dose finding, placebo-controlled study of oral almotriptan in the acute treatment of migraine. Neurology, 57, 1811n1817.
- Patel RC, Newman RC: Ureteroscopic management of ureteral and ureteroenteral strictures, Urol Clin North Am 31(1):107n113, 2004.
- Mosaku KS, Ukpong DI: Erectile dysfunction in a sample of patients attending a psychiatric outpatient department, Int J Impot Res 21(4):235n239, 2009.
- Avni FE, Guissard G, Hall M, et al: Hereditary polycystic kidney diseases in children, Pediatr Radiol 32:169n174, 2002.
- Klamt B, Koziell A, Poulat F, et al: Frasier syndrome is caused by defective alternative splicing of WT1 leading to an altered ratio of WT1/KTS splice isoforms, Hum Mol Genet 7:709n714, 1998.
|
|