"Order 100mg solian fast delivery, treatment juvenile arthritis."By: Carlos A Pardo-Villamizar, M.D.
 https://www.hopkinsmedicine.org/profiles/results/directory/profile/0008959/carlos-pardo-villamizar
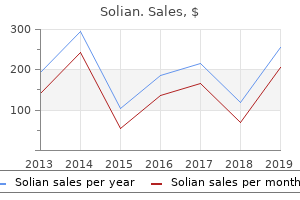
Solian 50mg with amexReabsorption occurs primarily (70%) within the ascending loop of Henle through passive mechanisms with a small quantity occurring in both the proximal tubule by way of passive mechanisms and distal convoluted tubules through active mechanisms. Role of Magnesium Magnesium performs a key role in plenty of biologic processes including protein synthesis, neuromuscular operate, and nucleic acid stability. It has been used to reduce anesthetic requirements and attenuate cardiovascular results of laryngoscopy and intubation. Magnesium has been proven to vasodilate blood vessels in lots of vascular beds (mesenteric, skeletal muscle, uterine, cerebral, coronary, and the aorta). It also decreases blood�brain barrier disruption and limits cerebral edema formation after mind injury. Hypomagnesemia Hypomagnesemia could end result from dietary defi iency (as seen in continual alcoholism), gastrointestinal malabsorption or secretion (diarrhea, vomiting, laxative use), renal losses (medication results, nephrotoxic brokers, endocrine illness, diabetic nephropathy), and chelation (citrate binding within the case of massive transfusion). Hypermagnesemia Hypermagnesemia is uncommon and mostly happens with excessive administration of magnesium for therapeutic purposes. Preeclampsia Magnesium seems to enhance the scientific signs of preeclampsia by causing systemic, vertebral, and uterine vasodilation by way of direct results on vessels in addition to by increasing concentrations of endogenous vasodilators (endothelium-derived enjoyable issue and calcitonin gene�related peptide) and attenuating endogenous vasoconstrictors (endothelin-1). Serum monitoring of magnesium ranges must be carried out for signs of toxicity or renal impairment. Magnesium crosses the placenta and should result in neonatal lethargy, hypotension, and respiratory melancholy if administered for prolonged duration (more than forty eight hours). Arrhythmias associated with hypomagnesemia are often29 accompanied by hypokalemia. Data to support the use of magnesium as an analgesic or for preventative analgesia at this level is conflicting. Total plasma calcium consists of calcium certain to albumin and proteins (40%), calcium complexed with citrate and phosphorus ions (9%), and freely diffusible ionized calcium (51%). The ionized concentration of calcium is dependent upon arterial pH, with acidosis growing and alkalosis decreasing the concentration. Additionally, plasma albumin binds nonionized calcium, thus, in low albumin states, less nonionized calcium is protein sure making extra out there to return to storage websites, such as bone and teeth. Thus, nonionized plasma calcium ranges must be interpreted with data of the plasma albumin focus and can be corrected according to the following formula: corrected Ca11 (mg/dL) 5 measured Ca11 (mg/dL) 1 [0. In cardiac myocytes, calcium regulates contraction, leisure, and electrical indicators that determine rhythm and triggers hypertrophy through calcineurin mechanisms. Symptoms of hypocalcemia embody neuromuscular excitability, including muscle twitching, spasms, tingling, numbness, carpopedal spasm, tetany, seizures, and cardiac dysrhythmias. Hypercalcemia Hyperparathyroidism is an important cause of hypercalcemia and may be major from parathyroid adenoma (85%), parathyroid hyperplasia (10%) which can be related to a quantity of endocrine neoplasia syndromes, or, rarely (,1%), parathyroid carcinoma. Secondary hyperparathyroidism outcomes from abnormal suggestions loops current in renal failure and tertiary hyperparathyroidism from overactive responses to regular negative suggestions mechanisms. Malignancies, such as squamous cell lung, breast, prostate, colon, grownup T-cell, and a quantity of myeloma, might lead to launch of parathyroid hormone� related peptide from tumor cells, resulting in inappropriate hypercalcemia. Hypercalcemia can additionally be related to granulomatous illnesses similar to sarcoidosis, tuberculosis, leprosy, coccidioidomycosis, and histoplasmosis and may outcome from extreme dietary supplement or medicine unwanted facet effects because of diuretic or lithium administration. Medications contributing to hypercalcemia should be discontinued and parathyroidectomy carried out if indicated. Corticosteroids can be used to decrease excessive calcium ranges by inhibiting the effects of vitamin D, decreasing intestinal absorption, and growing renal excretion. The natural matrix is greater than 90% collagen fibers, and the rest is a homogeneous material referred to as floor substance. Ground substance is composed of proteoglycans that embrace chondroitin sulfate and hyaluronic acid. Salts deposited in the organic matrix of bone are composed principally of calcium and phosphate ions in a mix known as hydroxyapatites. The preliminary stage of bone production is the secretion by osteoclasts of collagen and ground substance. Calcium salts precipitate on the surfaces of collagen fibers, forming nidi that grow into hydroxyapatite crystals. Bone is continually being deposited by osteoblasts and is constantly being absorbed where osteoclasts are energetic. Except in rising bones, the rate of bone deposition and absorption are equal, so the total mass of bone remains constant. Because physical stress stimulates new bone formation, calcium is deposited by the osteoblasts in proportion to the compression load that the bone must carry. The deposition of bone at factors of compression could additionally be attributable to small electrical currents induced by stress, known as the piezoelectric effect, stimulating osteoblastic exercise on the unfavorable finish of present flow. Osteoblasts are maximally activated at a bone fracture, the ensuing bulge of osteoblastic tissue and new bone matrix being generally recognized as callus. Alkaline phosphatase concentrations are additionally increased by any disease process that causes destruction of bone. A notable exception, however, is atherosclerosis, in which calcium precipitates in the walls of huge arteries. Calcium salts are also regularly deposited in degenerating tissues or in old blood clots. The phosphate groups of bisphosphonates, like inorganic pyrophosphate, bind hydroxyapatite crystals and turn into incorporated into websites of lively bone transforming, thus inhibiting calcification. Second- and third-generation bisphosphonates (alendronate, risedronate, ibandronate, pamidronate, and zoledronic acid) include nitrogen or amino teams in this position, which will increase the antiresorptive efficiency by binding and inhibiting farnesyl pyrophosphate synthase, resulting in osteoclast apoptosis. Duration of impact is a function of potency for mineral matrix binding, with zolendronic acid suppressing biochemical markers of bone resorption for up to 1 yr in ladies with postmenopausal osteoporosis. Clinical Uses Bisphosphonates are useful in treating scientific conditions characterized by increased osteoclast-mediated bone resorption, for example: osteoporosis, Paget disease of bone, osteogenesis imperfecta, hypercalcemia, and malignant bony metastasis. About 50% of the absorbed drug is retained within the skeleton, depending on renal perform, fee of bone turnover, and binding web site availability, and the rest of drug is eliminated unchanged within the urine. The incidence of this reaction decreases with every subsequent infusion; pretreatment with antihistamines and antipyretics44 can reduce the incidence and severity of signs. The condition is uncommon for oral remedy of osteoporosis (1 in 10,000 to 1 in one hundred,000). Serious atrial fibrillation (life-threatening or resulting in hospitalization or disability) occurred extra usually in sufferers treated with zoledronic acid than placebo (1. Approximately 3,500 mEq of potassium are current within the physique of a 70-kg patient (40 t o 50 mE q/kg). Because of this large difference in concentration, estimation of total physique potassium content from serum potassium values is inaccurate, despite the actual fact that the vast majority of potassium (90%) is instantly exchangeable between the intra- and extracellular compartments. Role of Potassium Potassium has an important affect on the control of osmotic pressure and is a catalyst of numerous enzymatic reactions. It is concerned in the operate of excitable cell membranes (nerves, skeletal muscles, cardiac muscle) and is instantly involved in the function of the kidneys. In cardiac cells, potassium decreases motion potential period, electrical inhomogeneity, and threat of digoxin toxicity. Potassium is an endothelial-dependent vasodilator; it decreases vascular easy muscle cell proliferation and inhibits thrombus formation and platelet activation. This is totally different from most different electrolytes, that are regulated by management of reabsorption in the distal tubule.
Cheap solian online amexPlasma concentrations are comparatively low after a single oral dose, which indicates first-pass hepatic extraction. Clinical Uses H1-receptor antagonists are among the most widely used of all medicines. In contrast to their role in the therapy of allergic rhinitis, H1-receptor antagonists provide little profit in the therapy of upper respiratory tract infections and are of no benefit within the administration of otitis media. Depend- ing on the H1-receptor antagonist selected and its dose, pretreatment might present some protection in opposition to bronchospasm induced by numerous stimuli (histamine, exercise, cold dry air). In patients with continual urticaria, H1-receptor antagonists relieve pruritus and decrease the number, dimension, and period of urticarial lesions. In some sufferers with refractory urticaria, concurrent treatment with an H2-receptor antagonist (cimetidine, ranitidine) could enhance aid of pruritus. The second-generation H1-receptor antagonists (cetirizine, fexofenadine, loratadine, desloratadine, azelastine) are supplanting fi st-generation medication (diphenhydramine, chlorpheniramine, cyproheptadine) within the remedy of allergic rhinoconjunctivitis and continual urticarial. Their greater value could be justified because of a more favorable risk-benefit ratio. For example, the first-generation H1-receptor antagonists have sedating results that end in delayed response instances. Diphenhydramine is prescribed as a sedative, an antipruritic, and as an antiemetic. When administered alone, it modestly stimulates ventilation by augmenting the interaction of hypoxic and hypercarbic ventilatory drives. Use of antihistamines in the acute therapy of anaphylactic reactions is directed at blocking additional histamine-mediated vasodilation and resulting homodynamic instability, in addition to decreasing respiratory and different systemic issues. As such, the administration of H1-receptor antagonists plus the administration of epinephrine is indicated in the remedy of acute anaphylaxis. H1-receptor antagonists are also useful within the ancillary remedy of pruritus, urticaria, and angioedema. These drugs can also be administered prophylactically for anaphylactoid reactions to radiocontrast dyes. The addition of H2-receptor antagonists to H1-receptor antagonists in the therapy of anaphylaxis speeds the resolution of symptoms. Dimenhydrinate has been used to treat movement illness in addition to postoperative nausea and vomiting. Manipulation of the extraocular muscle tissue as in strabismus surgical procedure may trigger an "oculoemetic" refle much like the well-described oculocardiac refle. If the afferent arc of this reflex can be depending on the integrity of the vestibular nuclei apparatus, then dimenhydrinate might attenuate or block this reflex and decrease the incidence of postoperative nausea and vomiting. Administration of these drugs at bedtime is typically beneficial as a result of drug-related somnolence is of no concern during the night time. Enhancement of the consequences of diazepam or alcohol is unlikely by second-generation medicine. Antihistamine intoxication is just like anticholinergic poisoning and may be related to seizures and cardiac conduction abnormalities resembling tricyclic antidepressant overdose. H2-Receptor Antagonists Cimetidine, ranitidine, famotidine, and nizatidine are H2-receptor antagonists that produce selective and reversible inhibition of H2 receptor�mediated secretion of hydrogen ions by parietal cells within the abdomen. Despite the presence of H2 receptors throughout the physique, inhibition of histamine binding to the receptors on gastric parietal cells is the main useful effect of H2-receptor antagonists. None of the four H2-receptor antagonists have produced any consistent results on decrease esophageal sphincter function or the rate of gastric emptying. Chapter 35 � Gastrointestinal Motility Drugs 705 Discontinuation of continual H2-receptor antagonist therapy is followed by rebound hypersecretion of gastric acid. Pharmacokinetics the absorption of cimetidine, ranitidine, and famotidine is fast after oral administration. Because of extensive fi st-pass hepatic metabolism, nevertheless, the bioavailability of these medicine is roughly 50% (see Table 35-2). The average time to peak plasma concentrations of the four H2-receptor antagonists ranges from 1 to three hours after oral administration. Approximately 70% of the total body content material of cimetidine is found in skeletal muscular tissues. All 4 medication are present in breast milk and can cross the placenta and blood�brain barrier. The presence of cimetidine in cerebrospinal fluid is increased in patients with extreme hepatic disease. The dose of cimetidine could must be decreased to keep away from psychological confusion in patients with extreme liver disease. The quantity of distribution of cimetidine can be decreased about 40% i n elderly sufferers, presumably reflecting the decrease in skeletal muscle mass associated with getting older. Hepatic metabolism is the principal mechanism for clearance from the plasma of oral doses of cimetidine, ranitidine, and famotidine, and renal excretion is the principal pathway for clearance from the plasma of an oral dose of nizatidine. Only nizatidine seems to have an lively metabolite (N-2-monodesmethyl-nizatidine), possessing about 60% of the activity of the father or mother drug. Hepatic metabolism of cimetidine occurs primarily by conversion of its side-chain to a thioether or sulfoxide, and these inactive merchandise seem within the urine as 5-hydroxymethyl and/or sulfoxide metabolites. The renal clearance of all 4 H2receptor antagonists is usually two to 3 occasions higher than creatinine clearance, reflecting in depth renal tubular secretion. Renal failure will increase the elimination halflife of all four medication, with the best impact on nizatidine and famotidine. Decreases within the doses of all 4 medicine are recommended for patients with renal dysfunction. Doses of H2-receptor antagonists can also need to be decreased in sufferers with acute burns. Only 10% to 20% of complete physique cimetidine or ranitidine is cleared by hemodialysis. Increasing age have to be thought of when figuring out the dose of H2-receptor antagonists. For instance, cimetidine clearance decreases 75% in patients between the ages of 20 years and 70 years. The elimination half-life of ranitidine and famotidine may be increased as much as twofold in aged patients. Clinical Uses H2-receptor antagonists are most commonly administered for the treatment of duodenal ulcer illness associated with hypersecretion of gastric hydrogen ions. In the preoperative period, H2-receptor antagonists have been administered as chemoprophylaxis to increase the pH of gastric fluid earlier than induction of anesthesia. The other H2-receptor antagonists have a profile to much like that of cimetidine with respect to placental switch. A corticosteroid administered no much less than 24 hours earlier is usually added to this regimen. Furthermore, H2receptor exercise might have desirable effects during allergic reactions, together with increased myocardial contractility and coronary artery vasodilation. In truth, drug-induced histamine release could additionally be exaggerated in sufferers pretreated with solely H2-receptor antagonists. Side Effects the frequency of severe unwanted effects is low with all 4 H2-receptor antagonists (Table 35-3).
Order 100mg solian fast deliveryFurthermore, absence of b-adrenergic blockade permits maximum expression of cardiac stimulation from norepinephrine, typically resulting in tachycardia. These unwanted facet effects prevent the usage of nonselective a-adrenergic antagonists in the administration of ambulatory important hypertension. Mechanism of Action Phentolamine, prazosin, and yohimbine are competitive (reversible binding with receptors) a-adrenergic antagonists. In contrast, phenoxybenzamine binds covalently to a-adrenergic receptors to provide an irreversible and insurmountable sort of a receptor blockade. Once a blockade has been established with phenoxybenzamine, even massive doses of sympathomimetics are ineffective till the impact of phenoxybenzamine is terminated by metabolism. Pharmacokinetics Absorption of phenoxybenzamine from the gastrointestinal tract is incomplete. The elimination half-time of phenoxybenzamine is about 24 hours, emphasizing the likelihood of cumulative effects with repeated doses. Cardiovascular Effects Phenoxybenzamine administered to a supine, normovolemic affected person in the absence of elevated sympathetic nervous system exercise produces little change in systemic blood stress. In addition, impairment of compensatory vasoconstriction ends in exaggerated blood strain decreases in response to blood loss or vasodilating medicine corresponding to volatile anesthetics. Nasal stuffiness is as a end result of of unopposed vasodilation in mucous membranes within the presence of a-adrenergic blockade. Excessive vasoconstriction with associated tissue ischemia, as accompanies hemorrhagic shock, could also be reversed by phenoxybenzamine but solely after intravascular fluid quantity has been replenished. As a result, this drug may be helpful in the therapy of the rare patient suffering from idiopathic orthostatic hypotension. In the previous, impotence had been efficiently treated with yohimbine in male sufferers with vascular, diabetic, and psychogenic origins. Yohimbine readily crosses the blood�brain barrier and could also be associated with elevated skeletal muscle activity and tremor. Excessive doses of yohimbine could produce tachycardia, hypertension, rhinorrhea, paresthesias, and dissociative states. Doxazosin Doxazosin is accredited for each therapy of hypertension and benign prostatic hypertrophy. Peak ranges of doxazosin are seen 2 to three h ours following oral administration and effectively relaxes prostatic and vascular easy muscle. The terminal elimination life of doxazosin is 22 hours and is really helpful as a single every day dose in the morning. Prazosin Prazosin is a selective postsynaptic a1 receptor antagonist that leaves intact the inhibiting effect of a2 receptor activity on norepinephrine release from nerve endings. As a outcome, prazosin is less likely than nonselective a-adrenergic antagonists to evoke reflex tachycardia. Following oral administration, the onset of motion is roughly half-hour and the duration of action is about four to 6 hours. Terazosin a Blocker remedy of benign prostatic hypertrophy relies on a1-mediated innervation of prostatic easy muscle that controls contraction of the prostate and obstruction of the bladder outlet. Terazosin is a long-acting orally effective a1-adrenergic antagonist that may be helpful within the therapy of benign prostatic hyperplasia by advantage of its capacity to relax prostatic clean muscle. Tolazoline Tolazoline is a competitive nonselective a-adrenergic receptor antagonist. This drug has been used to deal with persistent pulmonary hypertension of the new child but its use for this objective has been largely replaced by nitric oxide. Side results of tolazoline embrace systemic hypotension with refle tachycardia, cardiac dysrhythmias, and pulmonary and gastrointestinal hemorrhages. Mechanism of Action a2-Adrenergic receptor agonists have selective affinity for a2-adrenergic receptors and act competitively. Withdrawal after even short-term use can lead to a rebound impact with a dramatic increase in sympathetic outflow inflicting elevations in heart price and hypertension to even dangerous ranges. Clonidine Administration leads to dose-dependent decreases in coronary heart fee and blood strain and is used clinically to deal with resistant hypertension and tremors from central stimulant drugs. Clonidine is a partial agonist of a2 receptors with a four hundred:1 a2:a1 receptor desire. Clonidine is on the market in an intravenous, oral, and transdermal preparation and is metabolized in the liver however is excreted mostly unchanged in the urine and to a lesser extent in the bile and feces. Terminal half-life is approximately 12 to sixteen hours however could be extremely variable with any liver or kidney dysfunction. Dexmedetomidine Dexmedetomidine is a selective a2 agonist with a 1,600:1 preference for a2 receptors. Most typically, this a2 agonist is used within the intensive care and operating room settings as a sedative and analgesic because of its central sympatholytic results. Dexmedetomidine undergoes extensive biotransformation within the liver and is excreted largely in the urine; liver impairment can dramatically enhance plasma levels and length of action as a result of signifi antly decreased metabolism during infusion. Most a2 receptors are discovered within the central nervous system especially in the brainstem and the locus ceruleus. Peripherial inhibition of a2 receptors can lead to inhibition of insulin launch and induction of glucagon from the pancreas. Clinical pharmacologic effects embody hypotension, bradycardia, and central sedation with some delicate effects of analgesia all associated to the sympatholytic effects. Drug-induced b-adrenergic blockade prevents the effects of catecholamines and sympathomimetics on the center and clean muscle tissue of the airways and blood vessels. Chapter 19 � Sympatholytics 477 Propranolol is the usual b-adrenergic antagonist drug to which all other b-adrenergic antagonists are compared. Mechanism of Action b-Adrenergic receptor antagonists exhibit selective affinity for b-adrenergic receptors, where they act by competitive inhibition. Binding of antagonist medicine to b-adrenergic receptors is reversible such that the drug could be displaced from the occupied receptors if sufficiently large quantities of agonist turn into available. Chronic administration of b-adrenergic antagonists is associated with a rise in the number of b-adrenergic receptors. The net impact of badrenergic stimulation within the coronary heart is to provide constructive chronotropic, inotropic, and dromotropic results and these are the responses which are blunted by b-adrenergic receptor antagonists. It is estimated that about 75% of b receptors in the myocardium are b1, whereas b2 receptors account for about 20% of b receptors. Structure�Activity Relationships b-Adrenergic antagonists are derivatives of the b agonist drug isoproterenol. Substitutions on the benzene ring determine whether the drug acts on b-adrenergic receptors as an antagonist or agonist. The levorotatory forms of b antagonists and agonists are stronger than the dextrorotatory types. For example, the dextrorotatory isomer of propranolol has less than 1% o f the potency of the levorotatory isomer for blocking b-adrenergic receptors. Classification b-Adrenergic receptor antagonists are categorised as nonselective for b1 and b2 receptors (propranolol, nadolol, timolol, pindolol) and cardioselective (metoprolol, atenolol, acebutolol, betaxolol, esmolol, bisoprolol) for b1 receptors (Tables 19-1 and 19-2). It is important to acknowledge that b receptor selectivity is dose dependent and is misplaced when giant doses of the antagonist are administered. Drugs that exhibit cardiac selectivity for b1 receptors (cardioselective) are higher suited for administration to sufferers with asthma and reactive airway disease.

Discount 50 mg solian free shippingIn addition, obstructive sleep apnea doubles the chance for postoperative delirium within the elderly. It is most likely going that the upper proportion of body fats and lower surface area-to-mass ratio in females is liable for this difference. The attenuated cold stress responses of the elderly are additional diminished by general and regional anesthesia. Perioperative hypothermia may be very probably in the elderly affected person unless active measures are taken to keep up normothermia. Gastrointestinal Function in the Elderly Liver Although growing older is associated with a lower in liver mass and hepatic blood move, hepatocellular metabolic operate seems to be relatively well preserved all through life. Protein synthetic perform could additionally be diminished in some aged individuals, significantly these with poor dietary intake. On the opposite hand, the focus of one other essential drug-binding protein, a-1-acid glycoprotein, is usually elevated in the elderly. Hepatic synthesis of plasma cholinesterase may be diminished, significantly in men. There is proof of a rise in the duration of mivacurium exercise however not succinylcholine with age. Resting Core Temperature Aging is related to a greater variability in core temperature. The ordinary physiologic response to chilly stress is to lower heat loss by peripheral vasoconstriction and to increase heat production by way of shivering and nonshivering thermogenesis. The inability to effectively preserve heat in the elderly is exacerbated by the agerelated decrease in skeletal muscle mass. Loss of skeletal muscle mass is responsible for the age-related decline in basal warmth manufacturing. It is estimated that resting warmth production declines by 20% b etween the ages of 30 and 70 years. Mortality throughout chilly climate is greater in men compared to age-matched Gastroesophageal Physiology Gastric emptying of stable materials appears to be relatively regular within the healthy elderly population. However, gastric emptying of liquids could also be delayed in comparability with younger individuals. Dysphagia, vomiting, respiratory symptoms, weight loss, and anemia are extra common presenting signs within the aged. Table 46-4 Factors Associated with Reduced Resting Core Temperatures in the Elderly Neurologic illness Diabetes Low physique weight Lack of self-sufficiency Consumption of lower than two meals per day Smoking Alcohol consumption Chapter forty six � Physiology and Pharmacology of the Elderly 869 Table 46-5 Factors that Predispose to the Increased Incidence of Gastroesophageal Reflux Disease in the Elderly Increased prevalence of sliding hiatal hernia Shortened intraabdominal section of the decrease esophageal sphincter Impaired clearance of refluxed acid Use of medicines that scale back lower esophageal sphincter stress Decreased esophageal peristalsis pressure Renal Function within the Elderly Aging is accompanied by a lower in the cortical nephron population and a reduction in renal mass. This value decreases by approximately 1 mL/min/yr after the age of 40 years as a result of the decline in nephron inhabitants and hyalinization of cortical afferent arterioles. The medullary nephron inhabitants is relatively preserved, and age-related vascular modifications within the medulla are minimal. However, the renal response to frequent perioperative stresses may be inadequate to maintain homeostasis. Urine concentrating capability is critically dependent upon the presence of a hypertonic renal medulla. This suboptimal renal response to dehydration is compounded by age-related deficiencies in thirst mechanisms. This is particularly related as a outcome of the perioperative neuroendocrine stress response is related to arginine vasopressin (antidiuretic hormone) release and water retention. When combined with iatrogenic hypotonic fluid administration, these factors make the elderly affected person particularly vulnerable to perioperative free water overload and hyponatremia. Skeletal Muscle Mass and Aging Aging is associated with a major decline in neuromuscular efficiency. Loss of neuromuscular operate causes practical disability and loss of independence. Neuromuscular decline results predominantly from lack of skeletal muscle mass, which declines by approximately 40% between the ages of 20 and 60 years (sarcopenia). However, power losses with aging may be attenuated by continued bodily activity, significantly resistance training. Diminished skeletal muscle mass has important implications for the elderly patient within the perioperative interval (Table 46-8). Pain and Aging Pain is part of every day life for many elderly patients, with about 50% of patients older than the age of 70 years reporting continual ache. However, older sufferers appear to additionally require a higher depth of noxious stimulation earlier than fi st reporting ache. Chakour and colleagues46 demonstrated that pain transmission through C fibers was unchanged in young versus aged topics. Thus, the relative perceptions of ache in elderly subjects versus youthful subjects had been influenced by the extent of pain transmission via Ad fibers. Electroencephalographic studies of subjects treated with fentanyl, alfentanil, sufentanil, and remifentanil help a 50% d ose reduction for elderly patients. In contrast, morphine and meperidine have active metabolites, which accumulate within the elderly. However, with chronic administration, the levels of morphine-6-glucuronide will rise to pharmacologically lively concentrations. Thus, morphine-6-glucuronide will accumulate more in aged patients, necessitating a reduction in dose of chronically administered morphine. Of course, if the patient has renal insufficiency, it might be better to choose out an opioid without an energetic metabolite. Elderly sufferers have reduced meperidine clearance, leading to an extended half-life for meperidine. Meperidine Neurophysiology of Aging the aged show elevated sensitivity to benzodiazepines, opioids, and unstable anesthetic medicine. However, a neuroinflammatory response exacerbated by a faulty blood�brain barrier is thought to be mechanistically necessary. As the population ages and requires more surgical intervention, the Chapter 46 � Physiology and Pharmacology of the Elderly 871 will accumulate in aged topics with repeated administration. The alterations in physiology and pharmacology discussed earlier make the anesthetic administration of aged sufferers more challenging. The rising elderly population requiring surgery makes knowledge of these elements critical. With careful drug titration and pre- and postoperative management, even the intense aged can safely undergo surgical procedure to be able to enhance the standard of their lives. The frequency of adverse drug reactions as dependent upon age, sex and length of hospitalization. Arterial and cardiac getting older: main shareholders in cardiovascular disease enterprises. The prevalence of preoperative diastolic filling abnormalities in geriatric surgical patients. Age-related attenuation of isoflurane preconditioning in human atrial cardiomyocytes: roles for mitochondrial respiration and sarcolemmal adenosine triphosphate-sensitive potassium channel exercise.
Solian 100 mg free shippingBoth molecules have a big molecular weight (594 and 358 Da) and counteract the transmembranous water shift to prevent mobile edema Table 44-2). Hydroxyethyl starch was additionally added as an oncotic substance to stop growth of the extracellular space. The answer has an intracellular sodium concentration (15 mmol/L) and slightly elevated extracellular potassium concentration (10 mmol/L) (see Table 44-1). This electrolyte constellation causes a decrease in cardiac electrical activity and at last ends in diastolic cardiac arrest. Mannitol was added as an osmotic membrane-impermeable macromolecule (182 Da) to prevent hypothermia-induced cell swelling (see Table 44-2). The ingredients -ketoglutarate and histidine function substrates for the cellular vitality metabolism, and tryptophan was added as a membrane-protective agent. Celsior makes use of an amino acid buffer with histidine to prevent cellular acidosis, and the amino acids histidine and glutamic acid function the cellular power metabolism substrate. The first efficient preservation options had been developed for kidney preservation by Collins86 and Marshall92 in the Nineteen Seventies. Although the Collins and Marshall solutions supplied protected preservation of kidneys for 24 to 36 hours, both allowed only a safe short-term preservation (4 to eight hours) for liver allografts. Animals subjected to 5 to 10 minutes of ischemia followed by 10 to quarter-hour of reperfusion before prolonged ischemia showed decreased liver damage and improved survival. Preconditioning applies to pharmacological interventions within the donor or in the allograft earlier than implantation/reperfusion, whereas postconditioning intervenes through the time of reperfusion. Ten of 40 patients treated underneath this protocol donated their liver for transplantation. In this series one allograft developed major nonfunction and one other hepatic artery thrombosis. The principle of hypothermic oxygenated protection is based on the deactivation of mitochondrial respiration and decreased manufacturing of reactive oxygen species. The comparability of this group to a matched cold storage group revealed significantly lower rates of allograft dysfunction (5% versus 25%) and shorter hospital stay (10. This methodology, which uses supplemented blood as perfusate, allows real-time assessment of viable liver function by measuring oxygen consumption, bile move, and urea synthesis. Steatosis of the graft is a threat factor for posttransplantation biliary issues. Prediction of the outcome of transplantation in man by platelet adherence in donor liver allografts. Temperature effects on sodium pump phosphoenzyme distribution in human pink blood cells. Temperature adaptation of enzymes: roles of the free vitality, the enthalpy, and the entropy of activation. Biology of cell survival within the chilly: the basis for biopreservation of tissue and organs. Alterations in phospholipid metabolism in the globally ischemic rat coronary heart: emphasis on phosphoinositide particular phospholipase C exercise. Apoptosis and regeneration of sinusoidal endothelial cells after extended chilly preservation and transplantation of rat liver. Mitochondrial dysfunction and cytoskeletal disruption throughout chemical hypoxia to cultured rat hepatic sinusoidal endothelial cells: the pH paradox and cytoprotection by glucose, acidotic pH, and glycine. Pearls and Pitfalls · Graft injury is manifested on reperfusion however is the results of accumulated organ damage acquired in prepreservation, preservation, and rewarming periods. Livers from donation after cardiac death donors expertise heat ischemia as a half of the prepreservation damage. Cold prompts the sinusoidal endothelial floor, which makes it adherent for platelets and leukocytes. When a known threat factor similar to steatosis is present, all different adjustable risk factors such as chilly preservation time and rewarming time ought to be minimized. Critical preservation damage in rat fatty liver is to hepatocytes, not sinusoidal lining cells. Use of severely steatotic grafts in liver transplantation: a matched case-control examine. The effect of consecutively bigger doses of L-arginine on hepatic microcirculation and tissue oxygenation in hepatic steatosis. Impairment of hepatic mitochondrial respiratory function following storage and orthotopic transplantation of rat livers. Cold-induced apoptosis of rat liver endothelial cells: involvement of the proteasome. Evidence for the detrimental position of proteolysis throughout liver preservation in people. Evidence of a job for matrix metalloproteinases in chilly preservation injury of the liver in humans and in the rat. Inhibition of glycan shedding and leukocyte-endothelial adhesion in postcapillary venules by suppression of matrix metalloproteinase exercise with doxycycline. Calpain is a mediator of preservation-reperfusion damage in rat liver transplantation. Synergistic effect of cold and heat ischemia time on postoperative graft end result in human liver transplantation. Hepatic leukostasis and hypoxic stress in adhesion molecule-deficient mice after gut ischemia/reperfusion. Oxidative inactivation of key mitochondrial proteins leads to dysfunction and injury in hepatic ischemia reperfusion. Mechanism of cell demise during heat hepatic ischemia-reperfusion in rats: apoptosis or necrosis? A mechanism for matrix metalloproteinase activation and atherosclerotic plaque rupture by myeloperoxidase. Activation of human neutrophil procollagenase by nitrogen dioxide and peroxynitrite: a novel mechanism for procollagenase activation involving nitric oxide. Reactive oxygen species mediate modification of glycocalyx throughout ischemia-reperfusion damage. P-selectin mediates platelet-endothelial cell interactions and reperfusion harm within the mouse liver in vivo. Platelet adherence to isolated rat hepatic sinusoidal endothelial cells after cold preservation. The expression of von Willebrand factor, soluble thrombomodulin, and soluble p-selectin throughout orthotopic liver transplantation. Time course of coronary vascular endothelial adhesion molecule expression throughout reperfusion of the ischemic feline myocardium. Induction of adhesion molecule expression in liver ischaemia-reperfusion harm is associated with impaired hepatic parenchymal microcirculation. Leukocyte adhesion and cell dying following orthotopic liver transplantation within the rat. Receptor-mediated monitoring of tissue well-being through detection of soluble heparan sulfate by Toll-like receptor 4. The matrix component biglycan is proinflammatory and alerts through Toll-like receptors 4 and 2 in macrophages.
Duckweed. Solian. - How does Duckweed work?
- Are there safety concerns?
- Dosing considerations for Duckweed.
- Lung problems, jaundice, and arthritis.
- What is Duckweed?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96437
Purchase 50 mg solian amexBecause of its dependence on renal excretion and hepatic metabolism for clearance from the physique, accumulation of quinidine or its metabolites might happen in the presence of impaired operate of those organs. Patients in normal sinus rhythm handled with quinidine could show a rise in coronary heart fee that might be a results of presumably either an anticholinergic motion and/or a reflex enhance in sympathetic nervous system activity. This atropine-like motion of quinidine opposes its direct depressant actions on the sinoatrial and atrioventricular nodes and is why digitalis is often given earlier than quinidine therapy is initiated. Discontinuation of quinidine results in return of the platelet depend to normal in 2 to 7 days. Symptoms of cinchonism embody tinnitus, decreased listening to acuity, blurring of imaginative and prescient, and gastrointestinal upset. Because quinidine is an a-adrenergic blocking drug, it could interact in an additive method with medication that cause vasodilation. Quinidine also interferes with normal neuromuscular transmission and will intensify the impact of neuromuscular blockings medicine. Recurrence of skeletal muscle paralysis within the instant postoperative period has been observed in affiliation with the administration of quinidine. When the cardiac arrhythmia is managed, a relentless price of infusion (2 to 6 mg per minute) is used to maintain a therapeutic concentration of procainamide. As a end result, paradoxical ventricular tachycardia is a uncommon characteristic of procainamide remedy. Metabolism and Excretion Procainamide is eradicated by renal excretion and hepatic metabolism. This metabolite is cardioactive and doubtless contributes to the antiarrhythmic effects of procainamide. The exercise of the N-acetyltransferase enzyme response for the acetylation of procainamide is genetically decided. Unlike its analogue, procaine, procainamide is very immune to hydrolysis by plasma cholinesterase. Evidence of this resistance is the truth that solely 2% to 10% of an administered dose of procainamide is recovered unchanged in the urine as paraaminobenzoic acid. Despite this restricted binding in plasma, procainamide is avidly sure to tissue proteins aside from the mind. Side Effects Similar to quinidine, use of procainamide has dramatically decreased due to its facet effect profile and availability of newer agents. Hypotension that results from procainamide is extra prone to be caused by direct myocardial depression than peripheral vasodilation. Ventricular asystole or fibrillation might occur when procainamide is administered in the presence of heart block, as related to digitalis toxicity. Direct myocardial depression that occurs at high plasma concentrations of procainamide is exaggerated by hyperkalemia. As with quinidine, ventricular arrhythmias might accompany extreme plasma concentrations of procainamide. Chronic administration of procainamide could additionally be related to a syndrome that resembles systemic lupus erythematosus. Patients with this lupus-like syndrome typically develop antinuclear antibodies (positive antinuclear antibody test). Slow acetylators are extra doubtless than fast acetylators to develop antinuclear antibodies. Although agranulocytosis is rare, leukopenia and thrombocytopenia may be seen after persistent use of procainamide, usually in affiliation with the lupus-like syndrome. Th most common early, noncardiac problems of procainamide are gastrointestinal disturbances, including nausea and vomiting. Absorption of oral disopyramide is type of full, resulting in peak blood ranges inside 2 hours of administration. As a outcome, the standard elimination half-time of eight to 12 hours is prolonged in the presence of renal dysfunction. For this cause, disopyramide should be administered cautiously if sufferers have known cardiac conduction results. Disopyramide has signifi ant myocardial depressant effects and can precipitate congestive heart failure and hypotension. The potential for direct myocardial depression, particularly in patients with preexisting left ventricular dysfunction, seems to be greater with this drug than with quinidine and procainamide. Moricizine Moricizine is a phenothiazine derivative with modest efficacy in the therapy of sustained ventricular arrhythmias. Moricizine decreases the fast inward sodium ion current and likewise decreases automaticity. Side Effects Proarrhythmic effects happen in 3% t o 15% o f patients treated chronically with moricizine. Patients with poor left ventricular perform tolerate moricizine and small will increase in systemic blood stress and heart fee might accompany therapy. Plasma concentrations of theophylline may improve in sufferers treated with moricizine. Disopyramide Disopyramide is similar to quinidine in effectively suppressing atrial and ventricular tachyarrhythmias Chapter 21 � Antiarrhythmic Drugs 523 Lidocaine Lidocaine is used principally for suppression of ventricular arrhythmias, having minimal if any effect on supraventricular tachyarrhythmias (see Chapter 10). This drug is particularly efficient in suppressing reentry cardiac arrhythmias, similar to premature ventricular contractions and ventricular tachycardia. The efficacy of prophylactic lidocaine therapy for stopping early ventricular fibrillation after acute myocardial infarction has not been documented and is now not beneficial (see earlier discussion). Decreased cardiac output and/or hepatic blood circulate, as produced by anesthesia, acute myocardial infarction, or congestive heart failure, might lower by 50% o r more of the initial dose and the rate of lidocaine infusion necessary to take care of therapeutic plasma ranges. Concomitant administration of drugs such as propranolol and cimetidine can end result in decreased hepatic clearance of lidocaine. Lidocaine can be nicely absorbed after oral administration however is topic to intensive hepatic first-pass metabolism. Mechanism of Action Lidocaine delays the speed of spontaneous part 4 depolarization by preventing or diminishing the gradual lower in potassium ion permeability that normally occurs throughout this section. The effectiveness of lidocaine in suppressing premature ventricular contractions displays its capability to lower the rate of spontaneous phase four depolarization. The ineff ctiveness of lidocaine in opposition to supraventricular tachyarrhythmias presumably reflects its inability to alter the speed of spontaneous section 4 d epolarization in atrial cardiac cells. In high doses, however, lidocaine can lower conduction in the atrioventricular node as properly as in the His�Purkinje system. Metabolism and Excretion Lidocaine is metabolized within the liver, and ensuing metabolites might possess cardiac antiarrhythmic activity. Lidocaine depresses cardiac contractility less than another antiarrhythmic drug used to suppress ventricular arrhythmias. The convulsive threshold for lidocaine is decreased throughout arterial hypoxemia, hyperkalemia, or acidosis, emphasizing the importance of monitoring these parameters during steady infusion of lidocaine to sufferers for suppression of ventricular arrhythmias. The addition of the amine aspect group permits mexiletine to avoid signifi ant hepatic first-pass metabolism that limits the effectiveness of orally administered lidocaine.
Syndromes - Poor appetite or overeating
- Urinalysis
- Skin rash or lesion
- Tube through the mouth into the stomach to wash out the stomach (gastric lavage)
- Throw away leftover formula after a feeding. Do not keep it and use again.
- The time it was swallowed
- Inflammatory nerve conditions (neuropathies)
- In a separate door refrigerator/freezer for up to 3 or 4 months
- Photodynamic therapy (PDT) uses a special laser device, called an esophageal balloon, along with a drug called Photofrin.
Purchase solian online from canadaA lower in the atrial fee throughout atrial flutter or fibrillation might mirror slowed conduction velocity, a p rolonged efficient refractory period within the atria, or each. Metabolism and Excretion Quinidine is hydroxylated in the liver to inactive metabolites, that are excreted in the urine. The concurrent administration of phenytoin, phenobarbital, or rifampin may decrease blood levels of quinidine by enhancing liver clearance. Toxic results may develop at plasma concentrations solely slightly above therapeutic ranges. The ability of some unstable anesthetics to depress the sinoatrial node is a consideration if administration of phenytoin during basic anesthesia is planned. Metabolism and Excretion Phenytoin is hydroxylated and then conjugated with glucuronic acid for excretion in the urine. Because phenytoin is metabolized by the liver, impaired hepatic perform may result in larger than regular blood levels of the drug. Blood levels of phenytoin could be lowered by medication, corresponding to barbiturates, that improve its fee of metabolism. Warfarin, phenylbutazone, and isoniazid might inhibit metabolism and enhance phenytoin blood ranges. Uremia will increase the unbound fraction of phenytoin relative to the plasmabound portion. Symptoms embody ataxia, nystagmus, vertigo, slurred speech, sedation, and mental confusion. Cerebellar signs correlate with phenytoin blood levels of higher than 18 mg/mL. Tocainide Tocainide, like mexiletine, is an orally effective amine analogue of lidocaine that was formerly used for the continual suppression of ventricular cardiac tachyarrhythmias, however is no longer available within the United States. Its unwanted facet effects resemble those of mexiletine, however in uncommon sufferers, this drug has brought on severe bone marrow depression (leukopenia, anemia, thrombocytopenia) and pulmonary fibrosis. As with mexiletine, the mix of tocainide with a b-adrenergic blocker or one other antiarrhythmic drug has a synergistic impact. Phenytoin Phenytoin is particularly efficient in suppression of ventricular arrhythmias associated with digitalis toxicity. Mechanism of Action the results of phenytoin on automaticity and velocity of conduction of cardiac impulses resemble these of lidocaine. Because it delays conduction in the bypass tracts, flecainide may be efficient for the therapy of tachyarrhythmias as a result of reentry mechanisms as related to the Wolff- arkinson-White syndrome. About 25% o f flecainide is excreted unchanged by the kidneys, and the rest appears as weakly lively metabolites. Elimination of flecainide is decreased in sufferers with congestive heart failure or renal failure. Flecainide competes with metabolic pathways used by different drugs and in consequence could improve the plasma concentrations of digoxin and propranolol. Coadministration of amiodarone and fl cainide can double plasma flecainide concentrations. Phenytoin and other drugs that stimulate hepatic P450 enzymes might pace the elimination of fl cainide. Flecainide has a average adverse inotropic impact and a proarrhythmic impact, especially in patients with preexisting decreased left ventricular operate. Vertigo and issue in visible accommodation are frequent dose-related side effects of fl cainide remedy. These adjustments recommend the potential for atrioventricular or infranodal conduction block of cardiac impulses. Flecainide could depress sinoatrial node perform as do b-adrenergic antagonists and calcium channel blockers. The commonest noncardiac adverse effect of fl cainide is dose-related blurred imaginative and prescient. Therefore, capture thresholds ought to be remeasured in individuals with pacemakers after the steadystate fl cainide dosage is modified. The principal metabolites in those that metabolize the drug rapidly are pharmacologically lively and equal in antiarrhythmic potency to the parent drug. Because of extensive metabolism, the supply of propafenone increases considerably in the presence of liver disease. Side Effects Proarrrhythmic effects usually have a tendency to occur in patients with preexisting ventricular arrhythmias. Propafenone depresses the myocardium and will cause conduction abnormalities corresponding to sinoatrial node slowing, atrioventricular block, and bundle-branch block. Small doses of quinidine inhibit the metabolism of propafenone, whereas propafenone interferes with the metabolism of propranolol and metoprolol leading to elevated plasma concentrations of those b blockers. Nausea and vomiting could occur, and, rarely, cholestatic hepatitis or worsening of bronchial asthma manifests. Propranolol and esmolol are eff ctive for controlling the speed of ventricular response in patients with atrial fibrillation and atrial flutter. Multifocal atrial tachycardia could reply to esmolol or metoprolol but is greatest handled with amiodarone. Acebutolol, propranolol, and metoprolol are permitted for prevention of sudden death following myocardial infarction. For instance, in contrast to class I antiarrhythmic medication, propranolol decreases sudden demise as properly as reinfarction rates within the first year after acute myocardial infarction. As a outcome, the speed of spontaneous phase 4 depolarization and sinoatrial node discharge is decreased. The price of Propafenone Propafenone, like flecainide, is an eff ctive oral antiarrhythmic drug for suppression of ventricular and atrial tachyarrhythmias. Propafenone may be proarrhythmic, especially in sufferers with poor left ventricular function and sustained ventricular tachycardia. Absorption after oral administration is superb, and peak plasma ranges happen in about three h ours. In addition to b-adrenergic blockade, these medicine trigger alterations within the electrical exercise of myocardial cells. This cell membrane effect is probably liable for some of the antidysrhythmic effects of badrenergic antagonists. Indeed, dextropropranolol, which lacks b-adrenergic antagonist activity, is an eff ctive cardiac antiarrhythmic. The traditional oral dose of propranolol for chronic suppression of ventricular arrhythmias is 10 to eighty mg every 6 to eight h ours. The whole every day dose is decided by the physiologic results of propranolol on the heart price and systemic blood pressure. Effective b blockade is usually achieved in an in any other case normal particular person when the resting coronary heart price is 55 to 60 beats per minute. Administration at 1-minute intervals is intended to attenuate the likelihood of excessive pharmacologic effects on the conduction of cardiac impulses.
Cheap solian onlineSodium polystyrene sulfonate (Kayexalate) is an orally or rectally administered sodium trade resin used to remove extracellular potassium in exchange for sodium within the large gut. Potassium removal from the physique also could also be achieved by loop diuretics or, most rapidly and effectively, hemodialysis. The majority (85%) of whole body phosphate is saved in the bone as hydroxyapatite crystals inside the organic matrix. Most of the remainder is stored in soft tissue as phosphate, with solely 1% located within the plasma. Phosphate is important in power metabolism, intracellular signaling (cyclic adenosine monophosphate and cyclic guanosine monophosphate), cell construction (phospholipids), oxygen delivery (2,3-disphosphoglycerate), regulation of the glycolytic pathway, the immune system, the coagulation cascade, and buffering to maintain normal acid�base steadiness. Phosphorous absorption from the gastrointestinal tract and reabsorption in the kidney proximal convoluted tubules is stimulated by Vitamin D, and renal reabsorption of phosphorous is inhibited by the effects of parathyroid hormone. Renal illness disrupts this regulation, and ectopic tissue calcification in addition to hyperphosphatemia may outcome. Profound skeletal muscle weakness sufficient to contribute to hypoventilation may be attributable to hypophosphatemia, as well as central nervous system dysfunction and peripheral neuropathy. Causes of hypophosphatemia embody alcohol abuse; prolonged parenteral vitamin; medicines corresponding to acetazolamide, catecholamines, and theophylline; paracetamol overdose; large burns; recovery from hypothermia; hemodialysis; salicylate poisoning; and gram-negative bacteremia. Approximately 80% of the iron in plasma enters the bone marrow to be incorporated into new erythrocytes. In addition to bone marrow, iron is incorporated into reticuloendothelial cells of the liver and spleen. Iron can additionally be a important part of many enzymes necessary for energy switch. Hemoglobin synthesis is the principal determinant of the plasma iron turnover price. When blood loss happens, hemoglobin focus is maintained by mobilization of tissue iron stores. Indeed, hemoglobin concentrations become chronically decreased only after these iron reserves are depleted. The infant, parturient, and menstruating female may have iron necessities exceeding quantities obtainable within the food regimen and develop iron-deficiency anemia. Absorption of iron from the gastrointestinal tract is elevated by ascorbic acid (vitamin C) or in the presence of iron deficiency. Iron Deficiency Iron deficiency is estimated to be present in 20% to 40% of menstruating females but solely about 5% of grownup males and postmenopausal females. Attempts to prevent this deficiency of iron in massive elements of the population embody the addition of iron to flour, use of iron-fortified formulation for infants, and the prescription of iron-containing vitamin supplements during being pregnant. Causes Causes of iron-defi iency anemia include inadequate dietary consumption of iron, elevated iron necessities as a outcome of being pregnant or blood loss, or interference with absorption from the gastrointestinal tract. Severe iron deficiency is often the results of blood loss, either from the gastrointestinal tract or, in females, from the uterus. Partial gastrectomy,50 malabsorptive bariatric surgery,51 and sprue are causes of insufficient iron absorption. Diagnosis Iron deficiency initially leads to a decrease in iron stores and a parallel decrease within the erythrocyte content material of iron. Depleted iron shops are indicated by decreased plasma concentrations of ferritin and the absence of reticuloendothelial hemosiderin in a bone marrow aspirate. Plasma ferritin concentrations of lower than 12 mg/dL are diagnostic of iron deficiency. Iron-deficiency anemia is outlined as depletion of whole body iron associated with a decreased red cell hemoglobin focus. The large physiologic variation in hemoglobin focus, however, makes it tough to reliably identify all individuals with iron-deficiency anemia. Because iron-deficiency anemia is so widespread in infants, menstruating females, and recent parturients, delicate anemia in these sufferers is often handled empirically with iron supplementation earlier than pursuing a extra exhaustive diagnostic workup. However, in males and postmenopausal females, iron deficiency is far less common so it is important to seek for a explanation for blood loss every time anemia is current. Treatment Prophylactic use of iron preparations should be reserved for individuals at excessive risk for creating iron deficiency, such as pregnant and lactating females, low-birth-weight infants, and females with heavy menses. The inappropriate prophylactic use of iron ought to be avoided in adults because excessive accumulation of iron might injury tissues. If the focus deficit of hemoglobin earlier than treatment is more than three g/dL, therapeutic doses of oral or parenteral iron should enhance the hemoglobin about zero. An increase of two g/dL or extra in the plasma concentration of hemoglobin inside 3 weeks is evidence of a optimistic response to iron. Oral Iron Ferrous sulfate administered orally is probably the most frequent alternative for the therapy of iron-deficiency anemia and is available as syrup, drugs, or tablets. Ferric salts are much less effectively absorbed than ferrous salts from the gastrointestinal tract. Although different salts of the ferrous type of iron can be found, they provide little or no benefit over sulfate preparations. The traditional therapeutic dose of iron for adults to deal with iron-deficiency anemia is 2 t o 3 m g/ kg (200 m g daily) in three divided doses. Prophylaxis and treatment of delicate nutritional iron deficiency may be achieved with modest dosages of iron, such as 15 t o 30 mg day by day. Nausea and higher abdominal ache are essentially the most frequent unwanted effects of oral iron therapy, notably if the dosage is greater than 200 mg every day. Fatal poisoning from overdose of iron is uncommon, however kids 1 to 2 years of age are Chapter 17 � Intravenous Fluids and Electrolytes 447 most weak. Symptoms of severe iron poisoning could occur within half-hour as vomiting, belly pain, and diarrhea. In addition, there may be sedation, hyperventilation due to acidosis, and cardiovascular collapse. Hemorrhagic gastroenteritis and hepatic damage are sometimes distinguished at autopsy in fatal iron toxicity. In addition, tissue iron shops could also be restored extra quickly with parenteral iron than oral remedy. After absorption, the iron should be cut up from the glucose molecule of dextran to become available to tissues. The principal major opposed effect of parenteral iron therapy is the rare incidence of a extreme allergic reaction, presumably because of the presence of dextran. Less extreme reactions embrace headache, fever, generalized lymphadenopathy, and arthralgias. Hemosiderosis is more more likely to occur with parenteral iron therapy because it bypasses gastrointestinal absorptive regulatory mechanisms. Severe zinc deficiency happens most often within the presence of malabsorption syndromes. Symptoms of zinc deficiency embody disturbances in style and smell, suboptimal development in kids, hepatosplenomegaly, alopecia, cutaneous rashes, glossitis, and stomatitis.
50mg solian with mastercardMyelination is incomplete at delivery and is often achieved earlier than the third yr of age. Sarcomere dimensions, pressure-volume curves, and geometry of the intact left ventricle of the immature canine heart. Sustained adverse inotropism mediated by alpha-adrenoceptors in grownup mouse myocardia: developmental conversion from constructive response within the neonate. Benefit of antenatal glucocorticoids based on the purpose for very untimely start. A evaluate of perinatal acute ache: treating perinatal ache to cut back adult chronic ache. An analysis of the results of sucrose on neonatal ache with 2 generally used circumcision strategies. This rate is likely to enhance within the face of bettering outcomes from fetal surgical procedure. Pregnancy causes important physiologic changes that enable for the metabolic calls for of the rising fetus. When attainable, surgical procedure is carried out during the second trimester of being pregnant to avoid aff cting major organogenesis in the course of the first trimester and to scale back the chance of preterm supply which is elevated within the third trimester. In contrast, throughout fetal surgery, anesthetics that cross the placenta are used when possible to supply fetal anesthesia and analgesia. Cardiovascular Changes Pregnancy-induced modifications in the maternal cardiovascular system embody elevated blood quantity and cardiac output, decreased vascular resistance, and supine hypotension. Intravascular Volumes and Hematology Maternal intravascular fluid volume begins to extend in the first trimester of pregnancy as the end result of elevated production of rennin, angiotensin, and aldosterone, which together promote sodium absorption and water retention. By term gestation, the plasma volume will increase approximately 50%, and the purple cell quantity increases about 25%. The larger increase in plasma volume is the cause of the "physiologic anemia of being pregnant". Maternal hemoglobin usually remains at eleven g/dL or larger even at term, and decrease values at any time throughout pregnancy characterize anemia. Following supply, uterine contraction creates an autotransfusion of blood often in extra of 500 mL t hat also compensates for the acute blood loss from delivery. Values of less than 1 symbolize incomplete switch and values greater than 1 characterize accumulation of drug. In the absence of other hematologic abnormalities, the cause for gestational thrombocytopenia is a analysis of exclusion. Cardiac Output By the tip of the first trimester, maternal cardiac output increases, on average, by 35% above prepregnancy values and continues to extend to 50% above nonpregnant values by the tip of the second trimester, remaining at similar, elevated levels throughout the third trimester. This increased cardiac output is the outcome of each will increase in stroke quantity and heart price. Increases above prelabor values of 10% to 25% are noted through the first stage of labor and a 40% increase happens in the course of the second stage. This large increase is secondary to the autotransfusion from the final uterine contraction, decreased vascular capacitance from loss of the placenta, and decreased lower extremity venous strain from release of the aortocaval compression. This huge improve in cardiac output represents a moment of distinctive threat for patients with cardiopulmonary illness, particularly those with valvular stenosis and pulmonary hypertension. Plasma volume increases all through the first and second trimester and reaches a plateau through the third trimester. It is crucial to monitor patients with cardiac illness intently in the postpartum interval. Systemic Vascular Resistance In spite of will increase in cardiac output and plasma volume, systemic blood pressure normally decreases secondary to a 20% discount in systemic vascular resistance by time period. Blood pressure decreases approximately 20% by 20 weeks gestational age and then will increase towards nonpregnant values because the pregnancy reaches term. Central venous stress and pulmonary capillary wedge strain are unchanged throughout regular being pregnant despite the rise in plasma quantity because of the concurrent increase in venous capacitance. Aortocaval Compression In the supine place, blood strain commonly decreases as the results of aortocaval compression by the gravid uterus. Supine hypotension is manifest by symptoms of diaphoresis, nausea, vomiting, and dizziness. Vena caval compression may exacerbate lower extremity venous stasis and thereby end in ankle edema, varices, and the danger of venous thromboembolism. Chapter 45 � Maternal and Fetal Physiology and Pharmacology 853 Compensatory adaptations mitigate supine hypotension due to aortocaval compression. One example is a reflexive increase in peripheral sympathetic nervous system activity. This enhanced sympathetic activity increases systemic vascular resistance and maintains systemic blood pressure regardless of decreased cardiac output. Reduced sympathetic tone ensuing from neuraxial or common anesthesia will impair this compensatory response and worsen the hypotensive response to supine positioning. A lateral tilt is used to keep away from the hypotension that can be related to supine positioning with neuraxial techniques for labor analgesia and operative deliveries. The earlier described cardiovascular adjustments of a being pregnant produce significant adjustments within the regular cardiac exam. Auscultation reveals an accentuated first heart sound (S1) with an increased splitting of the primary heart sound brought on by dissociated closure of the tricuspid and mitral valves. A third heart sound (S3) is commonly heard in the final trimester and a fourth heart sound (S4) can be heard in a minority of pregnant patients on account of increased quantity and turbulent move. A mild systolic ejection (grade 2/6) murmur is usually famous over the left sternal border and is secondary to mild regurgitation on the tricuspid valve from elevated cardiac volume. Airway edema may be significantly problematic within the setting of preeclampsia, upper respiratory tract infections, and after prolonged pushing because of the associated increases in venous strain. Minute Ventilation and Oxygenation In order to accommodate the elevated oxygen demand and carbon dioxide production of the growing placenta and fetus, minute ventilation is elevated 45% t o 50% above nonpregnant values during the first trimester and stays at this increased level for the rest of the being pregnant. Inhalation of 100 percent oxygen for 3 minutes or, in an emergency, four maximal breaths over the 30 seconds will significantly delay the interval between apnea and arterial oxygen desaturation. As a result, oxygen is extra easily off-loaded to fetal hemoglobin, which has a left-shifted hemoglobin oxygen dissociation curve. Increased progesterone and estrogen concentrations during being pregnant additionally contribute to lowered esophageal sphincter tone. Together, these modifications result in an elevated incidence of gastroesophageal reflux throughout pregnancy. An improve within the residual volume of gastric content can additional improve the chance of aspiration, which is already elevated during being pregnant. To cut back the chance of aspiration, administration of a nonparticulate antacid, speedy sequence induction with cricoid pressure, and placement of a cuffed endotracheal tube are all generally a routine part of induction of common anesthesia in pregnant girl past midgestation.
References - Turner, J. A., Hauge, S., Von Korff, M., Saunders, K., Lowe, M., & Berger, R. (2002). Primary care and urology patients with the male pelvic pain syndrome: symptoms and quality of life. Journal of Urology, 167 (4), 1768n1773.
- Jiang H, Huang D, Yao S, et al: Improving drainage after percutaneous nephrolithotomy based on health-related quality of life: a prospective randomized study, J Endourol 31:1131-1138, 2017.
- 7052012.
- Gupta R, Warren T, Wald A: Genital herpes, Lancet 370(9605):2127n2137, 2007.
|
|


