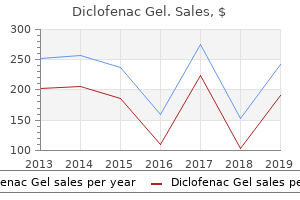
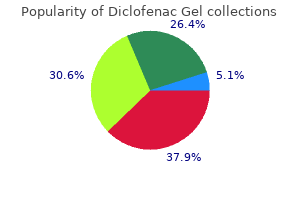
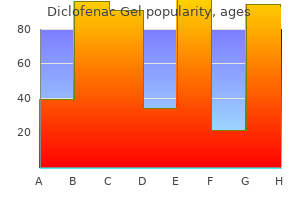
"Diclofenac gel 20gm free shipping, arthritis treatment bangalore."By: Peter Bartlett Bressler, MD - Associate Professor of Medicine
 https://medicine.duke.edu/faculty/peter-bartlett-bressler-md
Generic diclofenac gel 20 gm without a prescriptionIt involves deep delicate tissues of the lower limbs/limb girdles adopted by the trunk and upper limbs and infrequently the top and neck (including the salivary gland and mouth) and bone. Small blood vessels with surrounding fibrosis are sometimes present and tumor cells might concentrate around vascular channels. Claudin 1 is also usually constructive and this, coupled with positivity for eMa, might result in a misdiagnosis of perineurioma. Benign fibrohistiocytic tumors 1643 differential prognosis Distinction from myxofibrosarcoma relies on the presence of curvilinear blood vessels and no less than focal prominent cytological atypia with mitotic activity in the latter tumor. Lesions with related options occur within the tongue and are referred to as solitary oral fibromas. Variants with granular cell change, clear cell change and epithelioid cells have been described. It is essentially composed of interlacing fascicles of slender spindled cells, sometimes in a focal storiform arrangement, set within a free collagenous or (less often) myxoid stroma. Foci of persistent inflammatory cells, together with lymphocytes and plasma cells, and hemosiderin deposition are incessantly seen. Long-standing lesions present progressive hyalinization and decreased cellularity and are normally referred to as sclerosing or atrophic dermatofibroma. It has been instructed that epidermal progress issue could play a task within the pathogenesis of the epidermal hyperplasia. Changes simulating seborrheic keratosis are frequent, adopted by proliferation of clear cells mimicking a transparent cell acanthoma, and proliferation of immature hair follicle-like structures intently resembling a trichoblastoma, and induction of sebaceous glands typically in a reticulate pattern. D2�40 is diffusely constructive in dermatofibromas and solely very focally positive or unfavorable in dermatofibrosarcoma protuberans. Cellular fibrous histiocytoma Cellular benign fibrous histiocytoma accounts for nearly 5% of cutaneous fibrous histiocytomas. Metastasis to regional lymph nodes and lungs has been reported in a handful of cases. It is larger than the standard type and seems more mobile and mitotically lively. Aneurysmal fibrous histiocytoma aneurysmal benign fibrous histiocytoma represents less than 2% of fibrous histiocytomas and presents as a blue�brown nodule on the limbs of middleaged adults, especially females. Aneurysmal fibrous histiocytoma: the hemorrhagic areas are devoid of an endothelial lining. Epithelioid fibrous histiocytoma epithelioid fibrous histiocytoma is uncommon, has a wide age and anatomical distribution (with predilection for the proximal lower limb), and sometimes presents as a polypoid red nodule, which is usually confused with a pyogenic granuloma. Distinction from a cutaneous perineurioma with epithelioid cell change is made by the presence of diffuse eMa and claudin-1 positivity within the latter tumor. Atypical (pseudosarcomatous) fibrous histiocytoma atypical (pseudosarcomatous) fibrous histiocytoma is also called dermatofibroma with monster cells. Lesions are normally papular or nodular however could also be polypoid, and rare tumors measure up to several centimeters. In some areas, the tumor shows the options of a more typical fibrous histiocytoma. Clear cell fibrous histiocytoma it is a very rare variant with no distinctive medical options and with huge clear cell change throughout the lesion. It is most likely going that tumors beforehand described as clear cell fibrous histiocytoma represent the entity extra recently reported as dermal clear cell mesenchymal neoplasm. Atrophic dermatofibroma atrophic dermatofibroma probably represents the top stage of many dermatofibromas and is characterised clinically by an space of despair or retraction, typically resembling a scar or even anetoderma. Rare variants Very sometimes, tumors can present distinguished osteoclast-like giant cells (occasionally with ossification), granular cell change, ldl cholesterol deposition, focal easy muscle proliferation, marked myxoid change, keloidal change, balloon cell change and signet-ring change. Up to 42% of circumstances show a hemangiopericytoma-like pattern and stromal hyalinization is present in 39% of cases. Diffuse-type lesions could be distinguished from synovial sarcoma by the absence of an epithelial lining in the clefts and negativity for epithelial markers. No histological features enable prediction of which tumors will recur or metastasize. Angiomatoid fibrous histiocytoma scientific options angiomatoid fibrous histiocytoma (previously often recognized as angiomatoid malignant fibrous histiocytoma) is a uncommon tumor. Immunohistochemically, tumor cells are optimistic in about 50% of circumstances for desmin and for muscle actin (hhF-35), however not for clean muscle actin. It is feasible, combining morphology with immunophenotype, that these lesions show myoid (probably myofibroblastic) differentiation, although the mixture of eMa and desmin is uncommon. Distinction from aneurysmal fibrous histiocytoma is mentioned underneath the latter entity. Low-grade malignant fibrohistiocytic lesions 1657 plexiform fibrous histiocytoma clinical features plexiform fibrous histiocytoma (plexiform fibrohistiocytic tumor) is a rare however distinctive neoplasm that mostly presents on the limbs of youngsters and young adults (more than 50% of sufferers are younger than 20 years) and has a slight predilection for females. Local lymph node metastasis has been reported in three circumstances and in one of these unfold to the lungs was also seen. Cytogenetic research have been carried out in two instances with differing clonal chromosomal abnormalities. Varying numbers of osteoclast-like large cells are additionally present, primarily in the histiocytic variant. Often, the fibroblastic fascicles seem to radiate from a more strong central space. Fibrous hamartoma of infancy has a typical organoid progress pattern and lacks histiocytic nodules with osteoclast-like large cells. Dermal and deep benign fibrous histiocytomas normally have a extra cohesive progress pattern and polymorphism is seen all through the lesion. Occasional circumstances display outstanding sclerosis and even regression (focal or extensive). Moreover, the existence of a pleomorphic subtype (by far the most common tumor in the group) as an unbiased entity has been challenged. Most true pleomorphic sarcomas in the pores and skin symbolize extension from tumors arising in deeper gentle tissues. Features which may be unacceptable in the prognosis of atypical fibroxanthoma embrace areas of necrosis and vascular or perineural invasion. If current, they point out an alternate analysis corresponding to spindle cell squamous cell carcinoma, melanoma or a superficial pleomorphic sarcoma. Immunocytochemical stains for S-100 protein, keratin and desmin expression ought to always be undertaken to exclude melanoma, spindle cell squamous cell carcinoma, an unusual metastasis or a leiomyosarcoma. Malignant fibrous histiocytoma/undifferentiated pleomorphic sarcoma 1663 myxofibrosarcoma scientific features Myxofibrosarcoma (myxoid malignant fibrous histiocytoma) commonly presents in the limbs of the aged and reveals a slight predilection for males. In our expertise, using immunohistochemistry, at least a proportion of circumstances with the options described correspond to lymphoreticular malignancies together with t-cell lymphomas. Reactive lesions 1665 Infiltrative subcutaneous malignant fibrous histiocytoma this form of malignant fibrous histiocytoma is extraordinarily infiltrative and related to extensive involvement of fibrous septae by atypical spindled and pleomorphic cells in the subcutis and sometimes muscle. It can normally be distinguished from atypical lipomatous tumor/well-differentiated liposarcoma by the dearth of scattered atypical cells involving the lobules in contrast to the septa of the subcutaneous fat. Multiple recurrences of cutaneous carcinoma as a outcome of native tumor spread alongside the nerves of a traumatic neuroma have been reported. If excision is undertaken, a localized, somewhat fusiform, enlargement of one of the plantar digital nerves is seen.
Generic diclofenac gel 20gm with visaBullous pemphigoid antibodies are capable of complement fixation in as many as 75% of sufferers. In some stories, patients show positive direct immunofluorescence for IgG and C3 on the epidermodermal junction and a optimistic indirect immunofluo- 125. By direct immunoelectron microscopy, the immunoreactants (IgG and C3) are seen to be situated within the hemidesmosomal plaque and upper lamina lucida. More just lately, two patients with a nonscarring, bullous pemphigoid-like illness characterized by neutrophil-rich subepidermal blisters resembling dermatitis herpetiformis and antibodies to a novel 105-kD protein � so-called anti-p105 pemphigoid � have been documented. Transmembranous area Cell membrane Between 50% and 90% of patients with generalized bullous pemphigoid have antibodies that react with Bp230 and 35�50% have antibodies that react with Bp180 that are readily detected by immunoblotting. In some kids a minimum of, the IgG subclasses differ from grownup disease, consisting of all IgG subclasses or IgG2 in isolation. More lately, a case arising within the setting of radiation therapy has also been noted, perhaps suggesting a role for tissue harm within the pathogenesis of this disease. Following antibody� antigen interplay and complement fixation, varied chemotactic agents including C3a and C4a are produced. By direct cytotoxic motion (eosinophils are able to antibody-dependent cellular cytotoxicity) or by way of released proteases, particularly elastase, harm on the basement membrane region results in the event of a vesicle. Lymphocytes elaborate histamine-releasing issue (hrF), which increases mast cell degranulation and perpetuates the process. Bullous pemphigoid is due to this fact a real autoimmune disease in which antigen�antibody reaction and complement fixation results in a characteristic and reproducible practice of events, which is inevitably accompanied by the development of subepidermal blister formation. It may be exacerbated by way of oral contraceptives and barely complicates hydatidiform mole and gestational (but not nongestational) choriocarcinoma. Bullous lesions lasted solely 5 weeks in those that breast-fed in comparison with 24 weeks in those that bottle-fed. Other than pruritus, signs are usually delicate, with stinging, burning, and pain being comparatively infrequent. Pemphigoid gestationis: early erythematous lesion showing marked edema of the papillary dermis and conspicuous eosinophils. Occasionally, the presence of target or iris lesions might mimic erythema multiforme. Kolodney due to this fact thought of that there was no proof of an elevated incidence of stillbirths or abortions; nonetheless, his report predates the immunofluorescence era. More lately, evidence has been introduced that patients with pemphigoid gestationis are liable to ship low weight and small-fordates infants, prematurely. Pathogenesis and histological features the histopathologic options seen in biopsies from patients with pemphigoid gestationis are variable, relying upon whether or not early erythematous lesions, urticarial papular lesions, or totally established vesicles and bullae are studied. Occasionally the infiltrate of lymphocytes, histiocytes, and eosinophils is present in a linear distribution along the dermoepidermal junction. Leukocytoclasis and eosinophil dermal papillary microabscesses are only rarely identified. Complement pathway components including properdin and properdin factor-B can also be identified. Lesions significantly develop round abdominal striae, and periumbilical sparing is a attribute feature. Lichen planus pemphigoides Clinical features Lichen planus (lichen ruber) pemphigoides (Kaposi) must be distinguished from the vesicles occasionally seen in lichen planus as a consequence of severe hydropic degeneration (lichen planus vesiculosis). Clinically, the pemphigoid-like lesions are often preceded by typical lichen planus although not often the blisters could develop first. Pathogenesis and histological features the lichenoid lesions show the standard histopathological and immunofluorescent changes of lichen planus, but the bullae have options extra suggestive of bullous pemphigoid. Immunofluorescent examination of biopsies from peribullous pores and skin reveals linear deposition of IgG and complement. With NaCl-split pores and skin, the antibody typically labels the roof of the blister cavity. Ultrastructural investigations have shown that the level of separation is usually by way of the lamina lucida. By immunoelectron microscopy, the immunoreactants usually localize to the hemidesmosome and lamina lucida. In these cases related to antibodies to Bp180, epitope mapping might make the distinction. Mucous membrane pemphigoid (cicatricial pemphigoid) 133 Mucous membrane pemphigoid (cicatricial pemphigoid) Mucous membrane pemphigoid represents a spectrum of diseases. Nasal lesions, which can occur in as much as 15% of sufferers, lead to obstruction and occasionally cicatricial stenoses and septal perforation. Ocular lesions, which occur in roughly 64% of sufferers, are a supply of considerable morbidity. In males, genital lesions most frequently have an effect on the prepuce and the glans penis and are often complicated by urethral stricture formation. In late lesions all that may be noticed is a band of scarring in the superficial dermis with or without a subepidermal cut up. More commonly, however, the options seen are these of erosions or ulcers lined by granulation tissue or fibrous tissue and showing non-specific acute or chronic inflammation. The overlying pannus exhibits squamous metaplasia, chronic inflammation, and neovascularization. Conjunctival vesicles or bullae are very hardly ever seen in ocular cicatricial pemphigoid. Laryngeal, pharyngeal and esophageal lesions often present subepithelial bullae, erosions, ulcers, inflammatory changes, and fibrosis usually tend to be seen. In some sufferers, the break up is within the lamina lucida with the lamina densa lining the ground of the blister cavity whereas in others, lamina densa is found along the roof of the blister, and occasionally the lamina densa may be split, lining the roof and the floor. Epidermolysis bullosa acquisita (dermolytic pemphigoid) in from 50% to one hundred pc of instances with energetic disease. IgG and C3 could additionally be localized to the lower lamina lucida and lamina densa or else identified overlying the hemidesmosome. In the Brunsting-perry variant of localized continual pemphigoid the immunoreactants are localized within the lamina lucida and on the undersurface of basal keratinocytes. It is suggested that this latter discovering may account for the scarring attribute of this illness course of. For now, for the rationale that clinical features are extra uniform than those seen in the pores and skin, these mucosal instances are considered collectively. Epidermolysis bullosa acquisita (dermolytic pemphigoid) epidermolysis bullosa acquisita (dermolytic pemphigoid) is a rare, persistent blistering illness, which is characterised by variable scientific presentations and which can subsequently be mistaken for a number of other blistering disorders together with congenital epidermolysis bullosa and the opposite acquired autoimmune bullous dermatoses. More just lately, however, sufferers have been described in whom the illness has presented as a generalized inflammatory bullous dermatosis. In addition to the mechanobullous classical form of eBa, inflammatory variants, including bullous pemphigoid-like, mucous membrane pemphigoidlike, and linear Iga disease-like variants, can also be encountered. Milia are frequently conspicuous, and nail changes, including distal onycholysis, dystrophy, and anonychia with nail bed scarring, are widespread complications. More widespread involvement may resemble dominant or more often recessive dystrophic. Epidermolysis bullosa acquisita (dermolytic pemphigoid) 139 Mucous membrane pemphigoid-like variant Some patients present with a mucous membrane pemphigoid-like variant, characterised by mucous membrane involvement.
Diclofenac gel 20gm free shippingPhytophotodermatitis: this variant represents an allergic response to a plant chemical. Many drug reactions are photodynamic, whereas psoralen represents a nonphotodynamic reaction. The blister cavity is cell-free and the dermal papillae are preserved (festooning). It is assumed to end result from an lack of ability to detoxify arene oxide anticonvulsant metabolites as a outcome of absence, probably genetically determined, of particular hydrolases. There is pseudoepitheliomatous hyperplasia and a dense upper dermal lymphohistiocytic infiltrate. Pathogenesis and histological features the mucous membranes could additionally be affected, both alone or in association with cutaneous manifestations. Occasionally, the eruption is generalized and resembles toxic epidermal necrolysis. Some staff discovered that following problem, grafted normal pores and skin was unaffected, whereas transplanted beforehand affected skin developed erythema and became symptomatic. While some authors have documented in vivo certain immunoglobulin and complement within the intercellular area of the epidermis or at its basement membrane, the majority of investigations have been adverse. On initial publicity, the drug seems to bind to the epidermal keratinocytes (thereby functioning as a hapten) and is offered by Langerhans cells to lymphocytes inside the dermis or in local lymph nodes. Drug-induced hyperpigmentation 601 erythema multiforme although infectious brokers (herpes simplex virus, Mycoplasma species) are the most typical cause of erythema multiforme (eM), medications, or a combination of medicines and viral infections, are implicated in a subset of patients. Drugs with the strongest association embody antibiotics, anticonvulsants, and nonsteroidal antiinflammatory brokers. Other causative antibiotics embody aminopenicillins, quinolones, cephalosporins, and tetracyclines. It may outcome from increased melanin synthesis or deposition of the drug or its metabolite within the pores and skin. Drug-induced hyperpigmentation 603 Pathogenesis and histological features the histological options of minocycline pigmentation are variable. It is believed to represent minocycline or its breakdown product chelated with hemosiderin, ferritin or iron. One research also described green�gray nonrefractile globules inside macrophages in the fat. In mepacrine (quinacrine) pigmentation, yellow�brown pigment is discovered inside the cytoplasm of histiocytes all through the dermis. Ultrastructurally, histiocytes include melanosomes in addition to lysosomal-bound electron-dense granules. Discrete granulomata can also be recognized and granulomatous vasculitis has been documented. Purpuric drug reactions clinical options purpura may be a manifestation of an opposed drug reaction. Some cause alopecia in all people whereas others have an effect on only a minority of sufferers. Systemic disease-associated granulomatous dermatitis is usually associated with vasculitic and/or thrombotic phenomena. When elastophagocytosis is marked, granulomatous slack skin or an elastolytic granuloma may be necessary diagnostic issues. Bullous drug reactions heparin and warfarin and dextran sulfate, cause telogen effluvium in as much as 50% of sufferers. Many alleged drug reactions are single case reviews, notably in sufferers taking a number of medications. It is usually tough to determine which associations are therefore coincidental and that are real. In occasional stories, recrudescence following reexposure to the offending agent has been documented. In some patients there appears to be overlap between bullous pemphigoid and pemphigus vulgaris. More just lately imatinib (tyrosine kinase inhibitor) and voriconazole have been implicated. Split pores and skin oblique immunofluorescence in the former patient labeled the floor of the blister cavity and by immunoelectron microscopy the deposits were localized to the lamina densa and the sublamina densa region. Linear deposition of C3, IgG and IgM are seen on direct immunofluorescence, and IgG labels to the bottom of the blister on salt-spilt direct immunofluorescence. Many of those might characterize examples of drug-induced epidermolysis bullosa acquisita. By immunofluorescence, immunoglobulin (most commonly IgG) is current on the dermoepidermal junction and likewise outlining the superficial dermal vasculature. Histological options the histological features overlap lichen simplex chronicus and psoriasis. Histological options histologically, pityriasiform drug reactions are sometimes characterised by patchy parakeratosis, focal spongiosis with lymphocytic exocytosis, and a superficial perivascular lymphocytic infiltrate, sometimes related to purple cell extravasation. A perivascular persistent inflammatory cell infiltrate surrounds the superficial vasculature. Pustular drug reactions clinical features Drug-induced pustules are a manifestation of reactions to corticosteroids, anabolic steroids, oral contraceptives, isoniazid, haloperidol, and lithium therapy. B-cell lymphomatoid drug reaction is rare however has been described in association with fluoxetine hydrochloride and amitriptyline hydrochloride. Studies present that medicines implicated in drug-induced pseudolymphoma can induce proliferation of t cells and inhibit suppressor t cells, each in vivo and in vitro. Giant cells, collections of histiocytes, and epithelioid granulomata may also be evident. Blasts are sometimes current and lymphoid follicles with germinal centers may be evident. Kappa and lambda immunohistochemistry invariably show no evidence of light chain restriction. For a few years (as a consequence of its use as an insecticide) it was an ingredient in cigarette tobacco. Features that favor a drug-induced process over mycosis fungoides include vacuolar alteration, keratinocyte necrosis, spongiosis, and papillary dermal edema. If cutaneous pseudolymphoma is suspected, the most effective method to make the excellence Specific drug reactions progress to exfoliative dermatitis. Pathogenesis and histological options the mechanism of arsenic carcinogenesis is multifactorial. Skin cancers arising because of arsenic publicity present no distinguishing options histologically and are described elsewhere. It is commonly included in expectorants/bronchodilators and is used for therapy of thyroid illness and as a radiocontrast medium. Iododerma is related to a quantity of myeloma, polyarteritis nodosa, lymphoma, and glomerulonephritis. Pathogenesis and histological options although delayed hypersensitivity is believed to symbolize the underlying pathogenesis, the exact mechanism is unknown.
Purchase 20 gm diclofenac gel overnight deliveryIn cases of suspected cutaneous infective vasculitis, especially in immunosuppressed sufferers, an in depth medical historical past is important and the considered use of special stains is extremely advisable. Candidiasis, aspergillosis, cryptococcosis, and mucormycosis are of particular significance. Lepra bacilli are very generally seen in endothelial and vascular smooth muscle cells in lepromatous leprosy. Vasculitis in the setting of leprosy (erythema nodosum leprosum) is a common cause of vasculitis in areas of the world the place this disease is endemic. Vascular lesions in the pores and skin accompany a wide range of rickettsial infections together with epidemic typhus, scrub typhus, and rocky Mountain noticed Isolated granulomatous vasculitis of the central nervous system Kawasaki illness Reproduced with permission from Mader, R. Leukocytoclastic vasculitis is the most common sample of vasculitis associated with Table sixteen. Of curiosity, vasculitis could be present on the time of preliminary prognosis and in addition herald the onset of relapse. Cutaneous manifestations embrace maculopapular eruptions, purpura, urticaria, peripheral ulcers, and gangrene. Leukocytoclastic, polyarteritis nodosa-like, and lymphocytic types of paraneoplastic vasculitis have all been described and present histological options just like their nonparaneoplastic counterparts. Frank necrotizing vasculitis reveals infiltration of the vessel wall by neoplastic cells associated with necrosis and fibrin deposition in a pattern that resembles polyarteritis nodosa. Furthermore, you will need to distinguish lymphocytic from neutrophilic vasculitides. If strict standards are used � requiring vascular necrosis or important fibrinoid change for a prognosis of vasculitis � frank necrotizing lymphocytic vasculitis is an uncommon condition. Other uncommon associations of lymphocytic vasculitis embrace leukemia and the tumor necrosis factor receptor-associated periodic syndrome. Pathogenesis and histological features the pathogenesis of palisaded neutrophilic and granulomatous dermatitis doubtless is dependent upon the associated/underlying illness. When present, vasculitis normally reveals the features of leukocytoclastic vasculitis. More vital than the nosological nuances is rendering a report that alerts the clinician to the chance that the affected person may have underlying systemic disease, and when such lesions are encountered applicable scientific evaluation is important. Lymphocytic vasculitis Lymphocytic vasculitis is typically identified in circumstances during which a perivascular lymphocytic infiltrate is related to vascular harm. In many instances, the vascular modifications are delicate and minimal, including solely endothelial swelling and extravasated blood cells and sometimes focal fibrin deposition. Not surprisingly, the concept of lymphocytic vasculitis is considerably controversial. Kossard has defined lymphocytic vasculitis as an overlapping spectrum of changes varying from angiodestruction to endovasculitis and together with a pattern defined as lichenoid lymphocytic vasculitis. With progression, they develop a characteristic appearance: discrete small patches composed of a central zone with a depressed white, porcelain-like look and a nice scale, surrounded by a slender red or violaceous rim associated with fine telangiectasia. Laparoscopy often reveals characteristic subserosal white, yellow or pinkish plaques, typically slightly depressed and several centimeters in diameter. Of great significance, some sufferers develop small intestinal perforation with resultant peritonitis. For example, hemi- and quadriplegias, sensory losses, and cranial nerve lesions may all be encountered. Usually, however not invariably, an endovasculitis could be demonstrated in the blood vessels at the apex of the lesion: this consists of endothelial cell hyperplasia, typically sophisticated by thrombosis. Vascular modifications have included gross intimal thickening with consequent extreme diminution within the lumen diameter, thrombosis, and acute vasculitis. Atrophie blanche Clinical options atrophie blanche (livedo vasculitis, livedoid vasculitis, segmental hyalinizing vasculitis) is a typical dermatosis that often happens in the elderly, significantly females. Ulcerative lesions of two types may precede it: � small (1�5 mm diameter), very painful erythematous purpuric areas that ulcerate and heal slowly, � continual large areas of ulceration as a lot as 5 cm in diameter, which, after a long time period, heal to kind in depth areas of atrophic plaque. Lesions recur at periodic intervals and are predominantly located on the lower legs, ankles, and the dorsal surfaces of the feet. Variable degrees of red cell extravasation are evident and hemosiderin pigment is usually current. In the fully established atrophic plaque, along with the vascular changes, the dermis is atrophic and the dermis reveals dense scleroderma-like scarring. Differential prognosis the histological features in the acceptable scientific setting are diagnostic. Coagulopathies are associated with intraluminal fibrinoid plugs but not intensive fibrinoid change of the vessel wall. Dermatological manifestations of ldl cholesterol crystal embolism and embolism from atrial myxoma Clinical options Cholesterol crystal embolism is a illness of the elderly and sometimes happens in males (4:1), thereby reflecting the demographics of atherosclerosis. Necrotizing vasculitis has been described following cholesterol crystal embolization. Cutaneous manifestations are common and embody: � livedo reticularis, typically bilateral, affecting the toes and legs and sometimes extending up to involve the trunk,6 � gangrene of the toes. Cutaneous signs embody erythematous macules and papules predominantly of acral websites, digital cyanosis, petechiae, splinter hemorrhages, telangiectasia, and livedo reticularis. Diagnosis relies upon upon the identification of typical biconvex cleft- or needle-shaped empty spaces (representing evanescent cholesterol crystals dissolved during tissue processing) usually associated with atheromatous particles or luminal thrombosis. Multiple ranges also needs to be examined because emboli are most likely to be patchily distributed and are sometimes tough to detect. Due to vascular occlusion, this is accompanied by fibrin deposition and a reactive vascular proliferation. Demonstration of the myxoid substance is usually troublesome and generally requires examination of a quantity of ranges. Needle-shaped crystals are current in the lumen of an artery in the middle of the field. Malignant neoplasms (including carcinoma of the abdomen, breast and colon, small cell carcinoma of the lung, brain, and pancreas) and hematological malignancies have additionally been related to this situation. It develops as a complication of a prodromal infectious illness, mostly meningococcemia, scarlet fever, viral higher respiratory tract infection, chickenpox, rubella, and different exanthemata. Children develop giant confluent ecchymoses, which significantly have an result on the buttocks, legs, and feet, and generally seem on the upper limbs and abdomen. Clotting components could additionally be consumed at a price that exceeds the power of the liver for synthesis. Differential analysis the differential diagnosis contains other causes of coagulopathy or leukocytoclastic vasculitis. Serological evaluation for issues of coagulation is required to help the analysis. In patients with purpura fulminans, the thrombi are associated with diffuse and in depth hemorrhage. Older lesions are sometimes characterised by epidermal necrosis and subepidermal blood-filled bullae. Immunofluorescence studies for immunoglobulins and complement are uniformly unfavorable. Cryoglobulinemia Cryoglobulins are immunoglobulins that precipitate at low temperatures (4�C) and which redissolve on warming.
Cheap diclofenac gel 20gm without a prescriptionIn general the findings outcome from a mix of inflammatory adjustments and scarring. If examination of the scalp is performed at a late stage of the illness, overlap with other scarring alopecias is widespread, notably pseudop�lade of Brocq. Basal follicular keratinocytes in the concerned space turn out to be squamotized with larger dimension, distinguished eosinophilic cytoplasm, and cytoplasmic angulation. B In the late phases, the hair follicle is completely destroyed and replaced by a sclerotic collagenous follicular scar with loss of sebaceous glands. Other types of scarring alopecia (including pseudop�lade of Brocq and discoid lupus erythematosus) share this end-stage histological appearance. In order to highlight the presence of scarring tissue special stains to delineate elastic fibers are particularly helpful. In the histopathologic study, hair follicle miniaturization with a lymphocytic inflammatory cell infiltrate within the area of the isthmus and the infundibulum has been observed. Late lesions are characterized by perifollicular lamellar fibrosis and fibrosed follicular tracts. In one other variant of scarring alopecia thought of as a variant of lichen planus, frontal fibrosing alopecia, a similar etiopathogenesis and histopathology has been described. In discoid lupus erythematosus, the typical findings embrace a superficial and deep perivascular lymphohistiocytic infiltrate, dermal mucin, and vacuolar interphase change affecting not solely the follicles but additionally the intervening dermoepidermal junction. Lichen planopilaris: mucinous perifollicular fibroplasia; in active lesions focal accumulation of mucin surrounds the hair follicle. It is possible that pseudop�lade of Brocq represents a late stage of varied forms of scarring alopecia, together with lichen planopilaris. In the top stage it could be impossible to differentiate lichen planopilaris from pseudop�lade of Brocq and discoid lupus erythematosus. Sometimes perifollicular erythema, follicular keratinization, and extension onto the temporal and parietal zones could additionally be observed. There is an infiltrate on the interface between the hair infundibulum and the dermis; (B) high-power view. Note the artifactual cleft between the stellae and the encircling dermis (left), and melanin pigment granules in the scar. The histological appearances are those of lichen planopilaris with compromise of the superior follicular phase and an inflammatory cell infiltrate. The pores and skin seems mildly scarred with erythema across the hair follicles; (B) close-up view. The skin appears mildly scarred with prominence of the follicles and inflammation. In alopecia areata a noninflammatory alopecic band with preservation of follicular orifices and presence of exclamation mark hairs is noticed. Dermoscopy could be a helpful diagnostic software as the yellow dots usually seen in alopecia areata are absent in frontal fibrosing alopecia. Differential prognosis crucial differential diagnosis is keratosis follicularis spinulosa decalvans. Keratosis follicularis is regularly familial, starting in infancy and impacts atopic people. When the disease stabilizes, confluent plaques of alopecia with a shiny white porcelain-like floor are seen. In basic, inflammation is minimal and, if it is prominent, the illness is most unlikely to characterize pseudop�lade. Basic fibroblastic growth factor-type fibrogenic cytokines and transforming development factor-beta-type fibrogenic cytokines were extra strongly expressed in idiopathic pseudop�lade of Brocq in a current research. With progressive architectural distortion, the follicular channel becomes eccentric and typically adjoining hairs fuse, resulting in multiple shafts being current within a single channel (polytrichia). In distinction to the follicular stellae usually present beneath telogen follicles, in pseudop�lade these bands of fibrosis lengthen above and beneath the insertion of the arrector pili muscle. In pseudop�lade, the elastic fibers are preserved and dense elastic tissues are seen around the decrease a part of the follicle. In lichen planopilaris and discoid lupus erythematosus the elastic fibers are decreased or absent. Direct immunofluorescence is often unfavorable although often deposits of IgM are found along the basement membrane area. Borrelia burgdorferi has been detected within the scarred plaques of a quantity of patients, suggesting that it may be of etiological significance in no much less than a subset of instances. Pseudop�lade of Brocq: notice the insertion of the pili arrector muscle into a fibrotic scar. Biopsies from the central sclerotic area are prone to be equivalent no matter whether or not they come from a patient with pseudop�lade, discoid lupus erythematosus or lichen planopilaris. Other patients have a more progressive course with scaling, crusting, intense erythema, and pustules. Such variability could replicate superimposed bacterial an infection and differences in the inflammatory response to follicular harm. Isolated areas of alopecia show partial or full lack of hair follicles and the diploma of inflammation is variable. Central centrifugal scarring alopecia is the most common variant of scarring alopecia in patients of african heritage. It have to be obtained from a nonetheless active peripheral space which incorporates remnants of hair follicles. Desquamation in the follicular degeneration syndrome takes place deep to the isthmus and could also be noticed alongside the whole length of the hair shaft. Subsequent features embrace Scarring alopecias 1025 Differential analysis the differential analysis could also be troublesome as central centrifugal cicatricial alopecia shares comparable scientific and histological options with different types of scarring alopecias and nonscarring alopecias including pseudop�lade of Brocq, androgenetic alopecia, traction alopecia, and trichotillomania. In classic pseudop�lade of Brocq, histological distinction may be inconceivable in scarring lesions with solely a light inflammatory component, and close clinicopathological correlation is required to attain a analysis. In traction alopecia and trichotillomania, the scientific history of traction and notably the biopsy with findings of numerous hair follicles in catagen and telogen in addition to the presence of pigmented casts allows the analysis. In lesions with prominent irritation and an active border, the differential analysis consists of dissecting cellulitis, mycotic and bacterial infections, lichen planopilaris, and discoid lupus. Dissecting cellulitis is characterized by fluctuating nodules with a purulent discharge. Biopsy, cultures, and particular stains for microorganisms might exclude infectious processes involving the scalp, although an affiliation between central centrifugal cicatricial alopecia and fungal infection has been reported. In late lesions the hair is changed by fibrosing columns and the few remaining hair follicles fuse together. In its preliminary section it is very symptomatic with pain, pruritus, and a burning sensation in the scalp.
Pyridoxamine (Pyridoxine (Vitamin B6)). Diclofenac Gel. - Preventing reblockage of blood vessels after angioplasty, boosting the immune system, muscle cramps, eye problems, kidney problems, night leg cramps, arthritis, allergies, asthma, attention deficit-hyperactivity disorder (ADHD), Lyme disease, and other conditions.
- Are there any interactions with medications?
- What other names is Pyridoxine (vitamin B6) known by?
- Treatment and prevention of pyridoxine deficiency.
- Reducing elevated blood levels of homocysteine, a substance thought to be involved in heart disease.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96897
Diclofenac gel 20 gm onlineMaking the preliminary move with a thicker cutting needle to the level of the interspinal ligament, adopted by removing and advancement of a noncutting needle in the same delicate tissue tract, may be useful. If diameter have been the only consideration, as small a needle as potential would be used. A 2014 randomized crossover trial in contrast the use of 22-gauge and 25-gauge needles in kids and located no distinction within the incidence of post-puncture headache, however the 25-gauge needles have been found to be flimsy and difficult to use, with fluid assortment taking for a lot longer. Studies of the affect of directives corresponding to strict bed relaxation on post-puncture headache have yielded contradictory results, with no consensus on any particular preventive intervention forthcoming concerning the worsening of, improvement in, or impact on the incidence. Theonnissen and coworkers concluded that there was no proof that longer mattress relaxation after lumbar puncture was better than quick mobilization or short mattress relaxation in decreasing the incidence of headache. One advised routine is 500 mg of caffeine (sodium benzoate) diluted in one thousand mL of normal saline infused over a 1- to 2-hour interval. If profitable, consumption of caffeinated drinks could additionally be continued as an outpatient. Most post-puncture headaches may be managed by bed rest with the pinnacle in the horizontal place. Although dehydration should be prevented, the role of fluid supplementation in the prevention of post�dural puncture headache stays unsure. A patient with a prolonged headache after spinal puncture ought to be reassessed to rule out structural causes. In abstract, as a outcome of most post�lumbar puncture complications are delicate and self-limited, conservative therapy for the primary 24 to forty eight hours is beneficial. Bed relaxation and oral analgesics, including opioids, are normally efficient, in addition to, maybe, oral caffeine drinks, however for those refractory to conservative measures, an epidural blood patch is really helpful. For sufferers with a prolonged low-pressure headache, placement of an epidural blood patch by skilled operators is extremely profitable and sometimes provides dramatic reduction. Epidural patches are much less likely to be effective if symptoms have been current for more than 2 weeks. Patch failures (15% to 20%) are believed to be attributable to improper needle placement, injection of an insufficient quantity of blood (after which a second patch is normally successful), or an incorrect analysis. Complications reported after placement of an epidural patch include back stiffness, paresthesia, radicular pain, subdural hematoma, adhesive arachnoiditis, and bacterial meningitis. Particularly in patients with supratentorial masses, there could also be a large pressure gradient between the cranial and lumbar compartments. When mind quantity is elevated due to a mass or edema, rostrocaudal displacement could happen after lumbar puncture if the skull is unbroken. Controversy nonetheless exists concerning the chance for brain herniation from lumbar puncture in patients with acute bacterial meningitis, and data proceed to be sparse. Brain herniation is normally deadly, and occurs in roughly 5% of sufferers with acute bacterial meningitis and accounts for about 30% of the deaths associated with the disease. The frequency with which lumbar puncture causes or accelerates transtentorial herniation is unknown as a result of herniation may need developed spontaneously in a significantly unwell affected person with out the procedure. The meningitis might be coincidental ("spontaneous") or could outcome from leakage of blood containing micro organism into the subarachnoid area after lumbar puncture ("induced"). A 2006 review concluded that nearly all of circumstances of post-puncture meningitis are in all probability brought on by contamination of the site with aerosolized bacteria from medical personnel, contamination from skin flora, or least commonly, direct or hematogenous unfold from an endogenous infectious site. Delay in analysis due to concern regarding the dangers related to lumbar puncture might be more critical than the chance of causing meningitis with the process. From Hasbun R, Abrahams J, Jekel J, et al: Computed tomography of the top before lumbar puncture in adults with suspected meningitis, N Engl J Med 345:1727, 2001. Its outcomes ought to contribute to the decision regarding the necessity for and the risk involved with spinal puncture. Findings that counsel unequal pressure include (1) lateral shift of midline buildings, (2) lack of the suprachiasmatic and perimesencephalic cisterns, (3) shift or obliteration of the fourth ventricle, and (4) failure to visualize the superior cerebellar and quadrigeminal plate cisterns with sparing of the ambient cisterns. This strategy correlates with the medical coverage promulgated by the American College of Emergency Physicians in 2002. The absence of abnormal findings suggests the affected person is an effective candidate for quick lumbar puncture as a result of the danger for mind herniation because of the process is low (see Box 60. Joffe argues that scientific indicators of impending herniation are the most acceptable standards on which to base choices regarding the timing of lumbar puncture in patients with acute bacterial meningitis. Appropriate cultures of blood and more easily accessible body fluids ought to be obtained earlier than the administration of antibiotics. Critically unwell patients with acute bacterial meningitis typically deteriorate quickly and experience deadly mind herniation, each shortly after lumbar puncture and within the absence of the process. A 2007 review recognized 22 case stories of rapid deterioration and herniation after lumbar puncture in adults and youngsters with acute bacterial meningitis. In critically unwell sufferers, particularly these with localizing neurologic indicators, An epidermoid tumor or cyst is a mass of desquamated cells containing keratin within a capsule of well-differentiated stratified squamous epithelium. Congenital lesions arise from epithelial tissue that turns into sequestered on the time of closure of the neural groove between the third and the fifth weeks of embryonic life, however such lesions are rare. Acquired intraspinal epidermoid tumors outcome from the implantation of epidermoid tissue into the spinal canal on the time of lumbar puncture carried out with needles with out stylets or with ill-fitting stylets. The scientific syndrome consists of ache in the again and lower extremities creating years after spinal puncture. Failure to use a stylet on needle withdrawal may also lead to aspiration of a nerve root into the epidural house. Backache and Radicular Symptoms Minor backache from the trauma of the spinal needle happens in 90% of sufferers. Frank disk herniation has been reported from passage of the needle past the subarachnoid space into the anulus fibrosus. Perforation of a large vessel with resultant cisterna magna hematoma or obstruction of vertebral artery circulate has been described. Puncture of the medulla oblongata could cause vomiting or apnea, and puncture of the twine may be associated with pain. Spinal Epidural Hemorrhage Rarely, critical bleeding resulting in spinal hematoma after lumbar puncture can produce spinal cord compromise and permanent significant neurologic deficits, corresponding to cauda equina syndrome. The bleeding is concealed and might be suspected only by persistent extreme backache or neurologic findings. Surgical intervention, together with laminectomy and evacuation of blood, may be required and should occur in a timely method to keep away from permanent lack of neurologic function. Those with delicate signs and progressive recovery may be managed conservatively with shut monitoring. If the lumbar puncture is being carried out with the affected person in a seated place, place the affected person in the lateral decubitus place earlier than a measurement is obtained. This could also be carried out initially, earlier than fluid is collected, or after fluid assortment, by which case a closing stress is obtained. By repositioning the affected person and measuring the strain after fluid is collected, the probability of the needle being displaced on account of the repositioning is minimized. Measurements from struggling or agitated patients will in all probability be inaccurate; in such instances, sedation could permit more correct readings to be obtained. Opening stress is taken promptly, thereby avoiding falsely low values caused by leakage through and around the needle. Pressure may be falsely elevated in a tense affected person when the pinnacle is elevated above the plane of the needle and, probably, in markedly overweight sufferers and those experiencing muscle contraction.
Buy generic diclofenac gel 20gmLichenoid and granulomatous dermatitis Clinical options these lesions were described in 2000 by Magro and Crowson to have features of both lichenoid and granulomatous dermatitis. Clinically, the lesions present as lichenoid papules Pathogenesis and histology Various etiologic brokers included drug, coexisting medical sicknesses, and infections have been implicated. Working on this foundation, the following definitions have been proposed:1 � Bullous erythema multiforme is characterised by < 10% detachment, typical goal lesions, and generally raised atypical goal lesions. It is self-limiting and generally recurrent (recurrent erythema multiforme), although not often continuous episodes of erythema multiforme have been described (persistent erythema multiforme). In many patients, episodes of erythema multiforme are recurrent, creating as usually as 5 occasions annually. In maintaining with the present considering on this advanced topic, such instances are actually included in the spectrum of Stevens-Johnson syndrome. Overlap Stevens-Johnson syndrome/toxic epidermal necrolysis is characterised by 10�30% detachment, atypical target lesions, and flat erythematous macules. Marked basal cell hydropic degeneration sometimes ends in subepidermal clefting or vesiculation. Intra- and intercellular intraepidermal edema is clear and spongiotic vesiculation is normally a function. In biopsies from early lesions, the modifications could also be predominantly dermal with marked edema of the papillary dermis accompanied by a continual inflammatory cell infiltrate and pink cell extravasation. In erythema multiforme, nonetheless, there are commonly extra marked inflammatory modifications than seen in Stevens-Johnson syndrome and poisonous epidermal necrolysis by which the epidermal changes of widespread apoptosis are the predominant function. None of the findings is taken into account completely pathognomonic of any entity and clinicopathological correlation will most often guarantee their distinction with ease. Toxic epidermal necrolysis and Stevens-Johnson syndrome the unique description of poisonous epidermal necrolysis included two unrelated circumstances:1 � the scalded skin syndrome seen in infants and young children and as a result of staphylococcal infection with toxin production, � a drug hypersensitivity response, predominantly affecting adults, now regarded as the sole representative of this entity. Pathogenesis and histological options poisonous epidermal necrolysis/Stevens-Johnson syndrome almost at all times represents an adverse drug reaction. When the protein is injected into the skin of mice, blisters carefully simulating those seen in toxic epidermal necrolysis/ Stevens-Johnson syndrome develop. Marked lymphocytic exocytosis, apoptosis predominantly affecting the lower epidermis, intense, lichenoid dermal continual irritation with extension along the superficial and deep vascular plexuses, and prominent erythrocyte extravasation are extra in favor of erythema multiforme. Toxic epidermal necrolysis: medium-power view showing necrosis of the complete thickness of the roof of the blister. In addition to the standard features of poikiloderma, solar elastosis is often very marked. Paraneoplastic pemphigus erythema multiforme-like histological features are an integral function of paraneoplastic pemphigus. Rothmund-Thomson syndrome Clinical features this uncommon syndrome, which has been described in asians and blacks as well as Caucasians, has an autosomal recessive mode of inheritance. In distinction to the sooner finding of an equal sex incidence, the newer literature suggests a predilection for males (2:1). Caf�-au-lait spots are a common manifestation and discrete areas of hypopigmentation are ordinary. It represents a genetically homogenous single locus illness unassociated with any obvious heterogeneity. It is a multisystem disease related to untimely getting older and particularly impacts the pores and skin, enamel, eyes, skeleton, and central nervous system. Kyphosis, ankylosis, and flexion contractures are frequent issues, and dental abnormalities embrace malocclusions and caries. Involvement of the central nervous system presents as microcephaly, regular pressure hydrocephalus, psychological subnormality, ataxia, choreoathetosis, spasticity, myoclonus, and gait disturbance. Iron-laden neurons, neurofibrillary tangles, and big, bizarre astrocytes have also been reported. It has a predominantly X-linked recessive mode of inheritance and happens mainly in males (6:1), although each autosomal dominant and recessive variants are additionally recognized. Interface dermatoses the grave outlook of dyskeratosis congenita relates significantly to the development of infections complicating aplastic anemia, malignancy, and pulmonary complications. Biopsies of the mucosal lesions show an acanthotic epithelium with or with out dysplastic changes. In the latter case, nice care must be taken to exclude the presence of squamous cell carcinoma. It develops when transplanted immunocompetent donor t lymphocytes are activated, proliferate, and respond to international host major histocompatibility advanced (MhC)-histoincompatible antigens in a background of recipient immunosuppression. It often impacts a big floor space, exhibits mucosal involvement, and is associated with severe liver and gastrointestinal lesions. Lymphocytic exocytosis is invariably current and spongiosis is sometimes a feature. Follicular involvement is a typical characteristic and the hair bulge region is usually affected. Vascular adjustments include endothelial cell swelling with sloughing, and intimal and perivascular lymphocytic Interface dermatoses 253. The dermis incorporates dilated blood vessels and a lightweight perivascular continual inflammatory cell infiltrate. Viral infections also enter the differential analysis, as does an opposed drug response, for instance, to antibiotic remedy. Duration of the rash is kind of variable: though many patients are free of lesions by 3�6 months, others show nice persistence of the illness, usually for many years. Interface dermatoses majority of the infiltrate in pityriasis lichenoides acuta et varioliformis. Clonal t-cell receptor gene rearrangements have been described in small numbers of sufferers with pityriasis lichenoides acuta raising the potential for overlap with cutaneous t-cell lymphoma. In febrile ulceronecrotic Mucha-habermann illness, the features are these of very severe pityriasis lichenoides acuta and are often accompanied by the changes of leukocytoclastic vasculitis. Differential prognosis the histological options in continual superficial dermatitis are completely non-specific. In reality, the constellation of histological findings is among the most often encountered by the dermatopathologist. Delayed-type hypersensitivity reactions are more commonly associated with these histological appearances. Many different ailments equally trigger such non-specific biopsy findings including viral exanthems and connective tissue disease. Loss of t-cell expression might help a diagnosis of mycosis fungoides offered there are histological features in favor of the diagnosis and if the scientific context is suitable. Occasionally, only careful evaluate of the medical information, taken in conjunction with the histological features of earlier biopsies (if available) allows for definitive analysis. It is essential to observe that some investigators have demonstrated circumstances of continual superficial dermatitis with clonal t-cell gene rearrangements by polymerase chain response (pCr). In the previous, others have concluded that chronic superficial dermatitis is mycosis fungoides. Toxic erythema toxic erythema, annular erythema, and gyrate erythema are terms used by dermatologists to describe numerous ailments that share widespread clinical and histological appearances.

Order diclofenac gel 20 gm with mastercardMany of these peptides have antimicrobial action against micro organism, viruses, and fungi. Skin immunity is also offered by a distinct population of antigen presenting cells in the dermis often recognized as Langerhans cells. Langerhans cells then depart the dermis and migrate by way of lymphatics to regional lymph nodes. Besides antigen detection and the processing function by epidermal Langerhans cells, cutaneous immune surveillance can additionally be carried out within the dermis by an array of macrophages, t cells and dendritic cells. Can modify scientific expression of different diseases / Are implicated in growth of systemic allergy symptoms . Indeed, there are roughly 2 � 1010 resident t cells, which is twice the number of t cells within the circulating blood. Dermal immune sentinels are able to buying an antigen-presenting mode, a migratory mode or a tissue resident phagocytic mode. Ultrastructurally, melanocytes have pale cytoplasm and are devoid of tonofilaments and desmosomes. Dendritic processes are evident, (B) typical rod varieties with the characteristic trilaminar construction. The cytoplasmic vacuolation is a fixation artifact; (B) melanocytes can be highlighted with S100-protein immunohistochemistry. Melanin is transferred from melanocytes in melanosomes to neighboring keratinocytes in the epidermis and into the growing shaft in hair follicles and could be recognized by silver strategies such because the Masson-Fontana reaction. In heavily pigmented skin and darkish hair, melanosomes remain solitary and are longer than these seen in melanogenesis in paler races. Other cells that will comprise compound melanosomes include macrophages (melanophages), melanoma cells and, occasionally, Langerhans cells, the opposite kind of epidermal dendritic cell. Macromelanosomes (giant melanosomes) measure a number of microns in diameter and due to this fact are readily visible in hematoxylin and eosin stained sections. Normal dermis: this section of black skin has been stained by the Masson� Fontana response for melanin. Note the heavy pigmentation, which is current in each melanocytes and keratinocytes. Melanin protects the mitotically energetic basal epidermal cells from the injurious results of ultraviolet mild, which accounts for people with less pigmentation (fair-haired and light-skinned) having a much larger danger of sunburn and developing cutaneous malignancies (squamous cell and basal cell carcinomas, and melanoma). Other functions of melanin embody control of vitamin D3 synthesis and local thermoregulation. In pores and skin and hair, two types of melanin pigment are produced; eumelanin and pheomelanin. Notably, Notch transcription factor signaling in melanocytes is crucial for the maintenance of correct hair pigmentation, including regeneration of the melanocyte inhabitants throughout hair follicle cycling. Mature melanosomes of eumelanin are ellipsoidal in shape, while pheomelanin-producing melanosomes are spherical. V Merkel cells Merkel cells are postmitotic cells scattered all through the dermis of vertebrates and constitute zero. Ultrastructurally, Merkel cells appear oval with an extended axis of 15 m oriented parallel to the basement membrane. Merkel cells comprise numerous neurosecretory granules, every 50 nm to one hundred sixty nm across; these are discovered opposing the junctions with the sensory nerve ending. Merkel cells contain keratin filaments, notably keratin filament varieties eight, 18, 19, and 20, that are attribute of easy epithelium and fetal epidermis. Some of these include Merkel cells which form the Merkel cell�neurite advanced, while others are free nerve endings. In furry skin, Merkel cells also cluster within the rete ridges and in the outer root sheath of the hair follicle the place the arrector pili muscular tissues connect. Desmosomes are discovered in the dermis, myocardium, meninges and cortex of lymph nodes. Ultrastructurally, desmosomes include plaques of electron-dense material working alongside the cytoplasm parallel to the junctional area, in which three bands could be distinguished: an electron-dense band subsequent to the plasma membrane, a less dense band, and then a fibrillar space. The keratin filament community of two keratinocytes is linked by a series of desmosomal plaque proteins and transmembranous molecules to create a structural and signaling bridge between the cells. Cell signaling via -catenin can activate a number of pathways linked to morphogenesis and cell fate willpower. Inherited gene mutations of the adherens junction proteins plakoglobin and p-cadherin have been reported. Gap junction communication is important for cell synchronization, differentiation, cell progress and metabolic coordination of avascular organs, including dermis. Mutations in the 4 low molecular weight connexins shown at the high of the diagram are associated with a spectrum of skin pathology, as highlighted. Nondermatologic issues can also come up from mutations in some larger molecular weight connexins (Cx32, forty, 43, forty six and 50). Inherited gene mutations in claudin 1 have been reported in one pedigree with diffuse ichthyosis, hypotrichosis, scarring alopecia and sclerosing cholangitis. Mutations in hair keratin genes have been discovered to cause autosomal dominant forms of the human illness monilethrix. More common hair variants, such as curly hair, could also be explained by dynamic changes during hair growth. Normal vulva: sebaceous glands are conspicuous, however arise independently of a hair follicle and open directly onto the surface epithelium. Sebaceous glands consist of a quantity of lipid-containing lobules, normally linked to a hair follicle. Ultrastructurally, the mature sebaceous gland shows gradual accumulation of variably sized, nonmembrane-bound, lipid inclusions in differentiating cells. Its operate contains waterproofing, management of epidermal water loss, and a protecting operate, inhibiting the growth of fungi and micro organism. Secreted sebum undergoes significant modifications because of the presence of Propionibacterium acnes (triglyceride hydrolysis) inside the pilosebaceous canal and Staphylococcus epidermidis (cholesterol ester formation) on the perifollicular skin. The epithelium of the duct is more darkly stained than that of the glandular component. Eccrine glands human sweat glands are typically divided into two types: eccrine and apocrine. Sometimes the secretory lobules present putting clear cell change due to glycogen accumulation. On the basis of their expression of keratin filaments, they appear to be of ectodermal somewhat than mesenchymal derivation. Myoepithelial cells therefore develop from the epithelial cells of the tip of the secretory coil and never, as could be anticipated, from adjacent mesenchymal cells.
References - Pamies RJ. Crawford DR: Tumour markers, an update. Med Clin North Am 80: 185, 1996.
- Soygur T, Arikan N, Tokatli Z, et al: The role of video-urodynamic studies in managing nonneurogenic voiding dysfunction in children, BJU Int 93(6):841-843, 2004.
- Bazeed MA, Thuroff JW, Schmidt RA, et al: Histochemical study of urethral striated musculature in the dog, J Urol 128(2):406n410, 1982.
- Verze P, Margreiter M, Esposito K, et al: The link between cigarette smoking and erectile dysfunction: a systematic review, Eur Urol Focus 1(1):39n46, 2015.
|
|