"Best cinalid 250 mg, virus attack."By: Peter Bartlett Bressler, MD - Associate Professor of Medicine
 https://medicine.duke.edu/faculty/peter-bartlett-bressler-md
Buy cinalid usThe Second-Order Regulation-The Dienchephalon and the Limbic System Structures within the dienchephalon and within the limbic system take control over brain stem regulation a couple of weeks after birth. The thalamus collects alerts from the body and the sensory organs and distributes them to limbic and neocortical areas, together with prefrontal cortex. The thalamus distributes impulses from the cerebellum to the basal ganglia and to the motor cortex. The hypothalamus acts as the central regulator of bodily responses to relevant environmental occasions. The basal ganglia in the diencephalon manage motor skills, and they regulate the acts which are going to be executed. The basal ganglia reply with motor activity to natural rewards and Brain Development and the Everlasting Process of Self-Regulation forty nine threatening stimuli, and their activation causes excitement. The basal ganglia are carefully linked to the prefrontal cortex and the limbic system. While the decrease buildings of the brain are hard-wired to management involuntary perception and action, the limbic system mediates studying and reminiscence. The info move from sensory input to motor outputs is slowed down in the limbic system so that responses may be fitted more accurately to the discovered aspects of conditions. This slowdown amplifies the that means of emotions in the center of development by mediating emotional states that orient consideration and motion to whatever is currently essential. Early Interaction Modimes Regulation At the start of life, an toddler shows unimaginable readiness to join to the social world. From start on, a baby is interacting with the social surroundings with creating sensory capacities, particularly with odor, taste, and contact (Trevarthen, 2011). However, visible stimuli are alleged to have much less impression on creating sensory systems and on equilibrium maintenance during first weeks of life. The activation of the mirror-neuron system is fundamental for the development of language, social capacities, and cognition. In spite of innate predispositions to be social, an toddler is extraordinarily susceptible and absolutely at the mercy of others for cover. The mind techniques that mediate the equilibrium upkeep are 50 Introduction to Neuropsychotherapy creating rapidly in infancy, and this development is immediately and significantly influenced by early interaction with protecting others. The infant makes use of its maturing motor and developing sensory capacities to work together more vividly with the social environment. Her challenges and capabilities to arrange new learning and to adapt to a rapidly changing setting are modified by interaction processes, that are constantly influencing the maturation of connections inside her limbic system. It has been proposed that limbic networks are fashioned via ontogenic plasticity, which suggests natural choice of these regulative connections that match the environmental stimuli. In different phrases, the kid learns to calibrate her organic reactivity to the context. The first two years of life are crucial for incorporating regulative abilities, as a outcome of limbic areas within the cortex and subcortex are quickly rising throughout this time (Cicchetti & Tucker, 1994). Limbic areas type an emotional circuit that consists of connections between cingulate gyrus, the hippocampus, the hypothalamus, and the thalamus. The circuit includes additionally components of the prefrontal cortex, the brain stem, the basal ganglia, and the amygdale. The emotional circuit mediates stress-coping capacities throughout the lifetime, thus, early stress-inducing and stress-regulative occasions have long-lasting results on brain development and rising capacities. The Importance of Gazing Numerous mind research have documented a developmental shift in mind features at about eight weeks of age. At this level, a speedy metabolic change happens in the primary visible cortex, and the significance of visual experiences in modifying synaptic connections grows. An infant seems to be intensively thinking about faces and the number of mutual gazing durations will increase. It has been mentioned that face- to face interactions are extremely arousing, affect-laden events that expose Brain Development and the Everlasting Process of Self-Regulation 51 infants to excessive levels of cognitive and social data (Feldman, 2006). Mutual gazing episodes are also constructing blocks for rising social play, which is thought to be important for integrative growth of considering, language, and social talents. Synchronized interplay amplifies limbic emotional circuits including cingulate gyrus, which is quickly maturing on the age of six to eight months. Cingulate gyrus is a fundamental structure in emotional notion, and its posterior part regulates social habits, attachment habits, and the capacity for play. Diminished or disorganized play habits is known to be a common feature in developmental issues like specific language disorder and a spotlight deficits (Sajaniemi, Suhonen, & Kontu, 2008; Farrant, Maybery, & Fletcher, 2011). Ability to play is important for developing social and cognitive abilities, and decreased play behavior signifies a threat for developmental problems (Naber et al. Paying consideration to the standard of adult�child interplay may be a simple and effective approach to prevent developmental problems. Consistent and synchronized feedback to emotional shifts has a significant effect on modification of synaptic connections in the maturing mind. The sequences of "something thrilling is going on" and "pleasure is reducing" are consolidated in to neural limbic circuits known as procedural, implicit memory, or physique reminiscence. Processes of reexperiencing optimistic emotions educate the kid that negativity may be endured and conquered (Schore & Schore, 2008). The repetitive nature of interactive occasions form neural networks, that are reactivated in situations which have options in common with previous ones. They are like inside working models that assist to navigate in advanced environments and that can create a sense of security. Children learn to do not overlook that emotional shifts are part of everyday life and that they are often handled. Emotional associations are robust and long lasting, as a outcome of the amygdale produces concern responses impartial of the cortex, or, in different phrases, without considering, reasoning, or deciphering. As a consequence, stimuli related to negative feelings can evoke arousal even in an objectively safe surroundings. In such circumstances, growth might be channeled toward growing stress reactivity when subcortical networks are activated independently of higher cognitive features. Sensitization for stressors amplifies tendency for chronic anxiousness and panic attacks, and dampens explorative behavior, thus jeopardizing balanced development. In addition, if youngsters are living in a disorganized and careless environment, the coherence of experiences is misplaced. These kids might need difficulties in forming stable inside representations to facilitate the event of self-regulative expertise. It has been revealed in a rising variety of research that the mirror-neuron system within the human mind has a fundamental position in social cognition, language acquisition, and mentalizing conduct. Very little is understood about the mirror-neuron system in youngsters, but some studies have suggested Brain Development and the Everlasting Process of Self-Regulation fifty three that some elements of the mirror-neuron system, such as imitation, are innate (Meltzoff & Decety, 2003; Rizzolatti 2004). Young infants are capable of imitate oral actions, such as protruding their tongue, when they see another person doing the identical. Imitation studies have also documented that infants are able to distinguish between joyful, unhappy, and surprised facial expressions (Toda & Fogel, 1993).
Syndromes - Coproporphyrin
- Feeling strong emotions
- Near drowning (fluid in the lungs)
- Bumps in the ribcage (rachitic rosary)
- Malaise lasts longer than one week, with or without other symptoms.
- Fever
- Increased protein breakdown in the body
- Ulcerative colitis
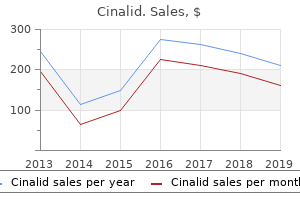
Discount 500mg cinalid fast deliveryHowever, a smaller number of such patients develop excessive sympathetic responses that have the potential to produce extra morbidity. There are currently at least 5 units of overlapping diagnostic standards used to describe the syndrome, the primary proposed in 1999 [5]. This sympathetic hyperactivity is accompanied by assorted forms of motor overactivity similar to decerebrate or decorticate posturing, dystonias, rigidity and spasticity. The pattern of posturing is most frequently asymmetrical and may not fit in to classical decorticate or decerebrate postures [6]. Minutely Heart Rate in an untreated dysautonomic topic (heart rates are minutely values derived from a 24 hour Holter monitor recording). While the subject had a number of episodes with coronary heart charges beneath eighty bpm (amounting to 11% of the day), heart charges above 140 bpm totaled 39% of the day. With growing time publish harm, paroxysms lower in length, frequency and magnitude. The discount in severity of paroxysms normally coincides with an observable improvement in neurological status [5,7], although whether or not this is causative or an epiphenomena has not been identified. As topics improve, paroxysms turn into rarer and resting blood stress, respiratory price, heart price and temperature trend towards normal values. These embody (in order of lowering frequency) extreme hypoxic brain injury, stroke (hemorrhagic stroke in particular), acute hydrocephalus and tumors. However, regardless of the big selection of etiologies associated with the disorder, the limited obtainable data means that the syndrome itself is equal irrespective of the causative situation. However, a quantity of attempts to both identify or deal with epilepsy in these sufferers have produced unfavorable outcomes (for instance [7,11-14] the restricted post-mortem and pathophysiological data counsel the syndrome outcomes from a relative disconnection of pathways at or across the degree of the midbrain (reviewed in [15]). Most disconnection theories recommend that paroxysms are driven by higher brainstem and diencephalon lesions, with medical options arising from both excitatory or inhibitory centers in these areas. However, more modern evidence means that spinal cord pro- 1406 Paroxysmal Sympathetic Hyperactivity in the Neurocritical Care Unit cesses are instrumental in initiating the situation. Two research have assessed the impact of standardized nociceptive stimuli in driving paroxysms. These studies provide empirical assist to anecdotal reports courting back to 1954 [18] that multiple bodily stimuli can provoke sympathetic paroxysms. This integrative model means that the causative brainstem facilities are predominantly inhibitory in nature, and that injury to these constructions predisposes the spinal twine to overreact to afferent stimuli in a fashion akin to that which produces allodynia (where non-painful stimuli become perceived as nociceptive) [22]. Such people have been found to have prolonged swallowing abnormalities, longer duration of coma and publish traumatic amnesia [5]. Affected people show lowered capacity for voluntary motion, notably throughout paroxysms, and could additionally be exacerbated by under-managed spasticity and dystonia [5]. In addition, posturing topics present increased metabolic charges [24,25] resulting in a highly catabolic state [26] and an estimated 25% loss of body weight in the first weeks post damage [2]. Affected people have additionally been discovered to be considerably more prone to develop heterotopic ossification [27]. These elements mix to place the individual vulnerable to creating important sickness or compression neuropathies, longer hospital admissions [2,5] and higher overall well being care costs [2]. As restoration continues, posturing patterns might change, revealing an underlying spastic tetraplegia or different focal neurological deficit. Sweating patterns change from entire physique to higher trunk, head and neck, before ceasing totally [31]. While the overt options of sympathetic hyperactivity settle over time, the tendency to show paroxysmal tachycardias remains evident for a minimum of 14 months submit harm [30]. Various autonomic emergency syndromes with similar symptom complexes (for example, malignant hyperthermia and neuroleptic malignant syndrome) ought to be ruled out. A careful examination for proof of triggering [16] and therapy of potential noxious stimuli (such as undiagnosed fractures, heterotopic ossification, pressure areas, painful spasticity or dystonias, an infection, and so forth. In this context, one creator has advised pre-treatment of patients prior to nociceptive procedures being undertaken to cut back "triggering" of paroxysms [33]. In spite of these attainable interventions, conservative measures alone are hardly ever sufficient to management the paroxysmal sympathetic overactivity in severe instances. Although a large quantity of drugs have been used to deal with the condition, info regarding their efficacy is largely restricted to anecdotal reports and has been reviewed elsewhere [3,four,21,34]. Accepting the constraints of current literature, a range of medicines from many courses of neurologically energetic brokers could also be helpful. Many topics will exhibit paroxysmal overactivity lasting for only a few months [5,27], the process is invasive and has a comparatively excessive complication rates (20-50% [39]). Intravenous morphine and midazolam are additionally efficient, but their sedative results limit their usefulness throughout rehabilitation [21]. Of the beta-blockers, propanolol has the biggest literature base, with combined stories between these where it has been useful and the place it has been unable to control paroxysms [4]. Labetalol has little literature obtainable, evenly split between beneficial and unhelpful. Clonidine also reduces catecholamine ranges [44], however has been reported to be helpful in less than half of the instances within the literature [4]. It has been instructed that clonidine could control sympathetic crises but requires excessive doses (for instance, 800 �g 2nd hourly) [45]. Dopamine agonists, predominantly bromocriptine, have a patchy literature of instances with a minimum of partial efficacy versus the place no impact was noticed [4]. Benzodiazepines additionally present a combined image, with anecdotal stories favoring diazepam and midazolam [7]. Drugs which have been reported to be ineffective embody methadone [7,11], metoprolol [13,29,33], oral baclofen [7,35], and phenytoin [11,28,46]. Oral dantrolene has been reported to be unhelpful in all but one patient [7,eleven,47]. However, in phrases of minimizing the chance of opposed drug reactions, it might appear appropriate to utilize morphine/midazolam, gabapentin and/or propanolol in the first occasion. There are occasional stories of wonderful efficacy with bromocriptine, suggesting it might have a secondary function. Also complicating the literature are the large number of synonyms used for the situation (around 33 in total), most of which have only been used a couple of times in the literature. The more generally used names include dysautonomia, autonomic dysfunction syndrome, paroxysmal sympathetic storms, paroxysmal autonomic instability with dystonia and so on [4]. Another difficulty with research in to the situation is the 5 present units of overlapping diagnostic standards [5,27,34]. In addition, it has recently been suggested that the concept of "triggering" of paroxysms following minor stimuli has been proposed as a clinical signal which will assist to differentiate individuals with and with out the syndrome [16]. Linked in with the issue of the dearth of diagnostic criteria, there has also been an absence of quantitative mechanisms to investigate the pharmacological administration of dysautonomia.
Best cinalid 250 mgThe danger related to discontinuation of anticoagulant remedy is determined by the sort of valve, the localization 1506 Postoperative Complications After Neurosurgery and factors of related dangers. In patients with just one aortic valve prosthesis and with out related threat factors, the anticoagulant is suspended three days earlier than surgical procedure. Patients at larger danger of thromboembolism are those with mitral valve prosthesis, atrial fibrillation, earlier thromboembolism, ventricular dysfunction, mechanical tricuspid valve or with a couple of mechanical valve. A interval of 5 to 7 days after-craniotomy might be a safe break to restart anticoagulation. Body Temperature During the instant postoperative interval, hypothermia must be avoided because it causes tremors which enhance oxygen consumption, cardiac debit and/or blood strain. All these alterations favour brain hyperaemia which can contribute to delirium in older patients, difficult to management arterial hypertension and intracranial hypertension. The finest way to restrict the event of tremors within the postoperative period is to keep normothermia. Fever may be very frequent in serious neurosurgery patients due the high risk of nosocomial infections. The mind temperature is underestimated, which increases the risk of secondary neuronal injury. An aggressive antithermic remedy for fever and common cooling measures are indicated. Glucose measurement every four hours is really helpful to stop a neurological disaster through the postoperative interval. Prospective and randomized studies in critically ill patients have demonstrated that the evolution is best in the surgical group that receives insulin remedy and stays euglycaemic (80-110 mg/dl) than in those with glucose levels between a hundred and eighty and 200 mg/dl. Hypoglycaemia can lead to irreversible neuronal damage and should be prevented to the utmost. In the postoperative interval the objective is to maintain the patient euglycaemic (140 mg/ dl) and not using a significant improve in the danger of hypoglycaemia episodes. Electrolyte Control Much attention should be directed to forestall electrolyte disturbances in the postoperative period. Disturbances happen by way of alterations between extracellular quantity and sodium concentration. Hyponatremia associated with hypo-osmolality contributes to the increase in intracellular volume which causes or aggravates cerebral edema and intracranial hypertension and with hyperosmolality can result in cerebral infarction. The major causes of hyponatremia/hypovolaemia in the postoperative interval are: diuretic, mannitol, vomiting, diarrhoea and mineralocorticoid deficiency. In these conditions, arterial stress, urinary debit and urinary osmolality may be low, but urea and creatinine will be raised. Anoth1507 Intensive Care in Neurology and Neurosurgery er essential cause of hyponatremia is the cerebral salt loss syndrome, which causes the discharge of natriuretic components leading to increased diuresis, natriuresis and hypovolemia with normal or raised urinary osmolality. Hyponatremia is corrected by the replacement of solutions with greater sodium focus (physiological saline 3%). This syndrome is caused by the inappropriate secretion of the antidiuretic hormone and is associated with water retention and hypervolemia with excessive urinary osmolality. If sodium is <115 mEq/l, convulsions or a coma state attributable to hyponatremia or within the presence of pathologies by which water restriction is contraindicated (period of vasospasm), a 3% saline answer can be administered. Prophylaxis of Infections the utility of antibiotic prophylaxis has been extensively mentioned over the last many years. Controlled studies have lastly demonstrated the effectiveness of acceptable antibiotic therapy. Prophylactic antibiotic remedy reduces the incidence of surgical website infections and meningitis through the postoperative interval. In craniotomies (clean surgeries) using cefazolin is really helpful in a single dose half-hour earlier than scalp incision or in special circumstances of 24-hour antibiotic treatment (ventriculoperitoneal shunt placement). Some research confirm the utility of pneumatic compression of the lower limbs before surgical procedure until the affected person can stroll once more. Beyond mechanical help, the utilization of low-dose heparin or low-molecular-weight heparin is recommended. The affiliation of mechanical and pharmacological prophylactic therapies in these patients is indicated. The majority presented bleeding but a small number developed with bleeding and perforation. Corticoids, extensively used in the neurosurgery inhabitants, contribute to the formation of gastrointestinal ulcerations. The threat of creating ulcers is twice larger and intestinal perforation can occur in corticosteroid users. Sulcrafate offers environment friendly prophylaxis without excessively rising gastric pH (less danger of ventilator-associated pneumonia). However, the issue to handle sulcrafate and the discount in the absorption of anticonvulsants and other medicine delivered by nasogastric catheter make H2 blockers and proton-pump inhibitors one of the best alternatives for a brief postoperative period. Any variation in this neurological analysis should be interpreted as a signal of worsening of the affected person and be adopted by full neurological examination and diagnostic and therapeutic measures. Over the subsequent 6 hours after extubation, a whole neuro-check could be performed every 30 minutes and then every hour as much as 24 to forty eight hours after surgery. The indications for motoring of intracranial strain after craniotomy are very various and controversial. A retrospective research monitored Postoperative affected person Intubated Extubated (first 6 hours) Extubated (after 6 hours) Glasgow Coma Scale Every quarter-hour Every half-hour Every hour Pupils Every 15 minutes Every 30 minutes Every hour Breathing Every half-hour Every hour Focal deficit Every 30 minutes Every hour Table eighty one. Hypertension is characterized by continual headache, nausea, vomiting, lowered stage of consciousness and neurological compromise. Some measures to management and prevent hypertension include: headboard elevated to 30 degrees; prevention and treatment of arterial hypertension; treatment for pain, nausea and vomiting; prevention and therapy of tremors; and maintenance of adjusted ventilation and oxygenation. The commonest causes of hypertension in the postoperative interval are: edema; hemorrhages; cerebral hydrocephalus; pneumoencephalus; and cerebral infarction. Cerebral Edema Apart from localization and kind of neoplasia, the principle focus in the immediate postoperative interval is cerebral edema. The development of edema in the immediate postoperative period is associated with manipulation of deep buildings and the elimination of cerebral tumours. In response to direct trauma from surgical intervention and tissue retraction, there happen relative tissue ischemia, reduction in venous return and reduction in cerebral complacency. The use of the electrocautery will increase the local damage and is immediately associated with cerebral tissue trauma. Motor or sensory alterations of the psychological state, deficits and paralyses of cranial nerves are widespread. The tomographic findings are: deletion of ridges; reduction of the dimensions of the ipsilateral ventricle; midline deviation; hypodensity and deletion of the interface between the white and gray matter. The headboard of the mattress should stay high (30 degrees) to aid cerebral venous return. Adequate cerebral perfusion pressure is stored by the infusion volume and use of vasoactive medicine. Corticoid administration (dexamethasone in four doses each 6 hours as much as a dose of 10-40 mg) is beneficial for sufferers submitted to brain tumour resection.
Generic cinalid 500 mg on lineIn one survey of 118 community-dwelling individuals sixty five or older with advanced illness, 58% of those with a desire to obtain extremely intensive intervention to treat their underlying disease acquired only symptomatic treatment [6]. This research, no less than, suggested that many "terminal" sufferers had been receiving much less aggressive care than they had been keen to endure. The hospice and palliative care movements have been instrumental in increasing the understanding of end-of-life care, and in providing patients options to dying within the hospital. The most significant barrier in coordinating and providing end-of-life care is inadequate communication, and at current only 25% of sufferers who could be eligible for hospice really enter hospice applications. Early discussion of prognosis and end-of-life care options can help facilitate earlier entry in to hospice and palliative care programs. But the truth is usually very completely different, and a survey of 29 most cancers nurse specialists found 1740 Ethical Considerations within the Neuro-Intensive Care Unit that interventions in the acute setting are typically driven by a preoccupation with treatment, routine apply, and adverse perceptions of palliative care [7]. All of these elements can shape medical decision-making and forestall patients and their households from fully participating in scientific decision-making at the end-of-life. In one prospective examine, the implementation of such a program resulted in a big increase within the variety of signs documented, and the number of care plans recorded [8]. Opioid medicine availability elevated from 57% to 83%, and do-not-resuscitate orders increased from 62% to 85%. The effect of race and cultural background on end-of-life decision-making has been examined, and no less than one U. In addition, the quality of care at the finish of life is strongly correlated with the place sufferers die. To be sure, the effectiveness of palliative care packages in selling end-of-life decision-making is intently associated with the certainty of the prognosis. In addition, the chance that the terminally sick affected person might have access to , or benefit from, palliative care may be related to their age. Studies counsel that elderly sufferers with terminal sicknesses are more likely to obtain palliative care previous to death, while sufferers youthful than 50 years are extra likely to be admitted to acute care hospitals and receive invasive life-support measures. The vast majority of patients who die in acute care hospitals, nursing houses, or hospice facilities have "do1741 Intensive Care in Neurology and Neurosurgery not-resuscitate" orders in place, indicating that the well being care providers and members of the family have been anticipating their demise. Those with advanced directives had been much more likely to have withdrawal of life-sustaining therapies prior to dying than have been those with out such directives. However, the implementation of Advanced Directives is commonly sophisticated by uncertainties of prognosis. For instance, in one research of 88 people sixty five or older, who had been hospitalized for forty eight hours or more, the themes reported less of a want to receive life-sustaining therapy, and notably cardiopulmonary resuscitation or artificial nutrition and hydration, when surveyed 14 days after discharge from the hospital than they did prior to their hospitalization [11].
[newline]Compared to these without dementia, the 31,654 sufferers with dementia had been significantly less prone to receive any of those 5 aggressive medical therapies at the end of life [15]. One report from Ireland cited confusion in translating policy in to practice as contributing to communication difficulties in initiating, documenting, and implementing cardiopulmonary resuscitation choices [16]. But such decisions must always respect 4 key moral principles: beneficence, nonmaleficence, autonomy, and distributive justice [17] (Table ninety seven. Unfortunately, selections to withhold or withdraw treatment are sometimes not given adequate consideration by healthcare providers, and research recommend that physicians need to do a better job communicating with relations about the numerous ramifications of these choices. In one study of 102 elderly patients with terminal ailments admitted to two acute care hospitals in Spain for terminal care, relatives or different main care givers were questioned about numerous features of the care being offered [18]. The relatives felt that the medical data they got was correct in solely 67. Control of medical symptoms was thought of good in 55%, however there was a notion that pain endured in 14%, and 45% of patients had uncontrolled dyspnea. In one study, mechanical ventilation, inotropes or vasopressors, and dialysis, have been considerably more more probably to be withdrawn if the physician predicted a less than 10% probability of survival for the patient [19]. Discontinuation of the mechanical ventilator, and elimination of the endotracheal tube, are the most common methods during which life help systems are removed from a patient for whom no further remedy could be of profit. Patients may be judged to be "symptomatic" in the course of the strategy of extubation, and require sedation with either a benzodiazepine or opioid treatment. The recorded cause for administering the medications was to decrease pain in 88%, lower nervousness in 85%, decrease air hunger in 76%, to consolation families in 82%, and to hasten demise in 39%. But in no occasion was hastening death the only reason cited for administering the sedative or analgesic. During the 24 hours previous to withholding or withdrawing of life-support, common doses of diazepam have been 2. After withholding or withdrawal of life-support significantly larger doses of the drugs have been administered, with average doses of � Beneficence diazepam of 9. Key concerns for withholding or prior to dying have been interviewed regarding withdrawal of care [17]. All sufferers have been sedated following withdrawal of mechanical ventilation, with the most typical medication being morphine (119 pts), adopted by midazolam and lorazepam. In 91% of the circumstances, relations reported that their loved-one was totally, very, or largely snug on the time of death. In one research of 32 non-brain-dead sufferers who had been terminally extubated, 25% died inside an hour of extubation but one third of the sufferers survived for 24 hours or extra, and the median survival following extubation was 7. Moreover, removal of the endotracheal tube often is associated with extreme respiratory secretions that may cause a distressing stridor which may lead family members to imagine the patient is choking and suffering. This "death rattle" is most commonly reported in sufferers dying from pulmonary malignancies, main brain tumors, and brain metastases, and predicts dying within 48 hours in 75% of sufferers. A group in the Netherlands has developed a medical protocol that they declare is efficient in eliminating the demise rattle [23]. Six hours earlier than extubation, enteral feeding is stopped and parenteral fluids are lowered. Sedatives, opiods, and methylprednisolone are administered, and butylscopolamine is given 30 minutes earlier than extubation. However, terminal restlessness, or the unsettled behaviors and delirium that occurs in a substantial proportion of patients throughout the last few days of life, could typically be due to a few of these same medicines. Treatment induced delirium or restlessness has been related to opioids, antisecretory brokers, anxiolytics, antidepressants, antipsychotics, antiepileptics, steroids, and nonsteroidal anti-inflammatory medication. Withholding or withdrawal of the feeding tube is considered by most to be the single most controversial and ethically difficult decision for both family members and treating physicians. For example, a survey of Japanese physicians revealed that while most were comfortable withholding mechanical ventilatory assistance, the bulk felt that tube feeding ought to really be initiated in patients with terminal sickness [24]. And while the primary concern has been that withholding of those fluids is merciless and causes the affected person to suffer, experienced palliative care medical doctors and nurses have really discovered that terminal dehydration seems to lessen suffering for dying sufferers [25]. In their observations of 51 physician-family conferences by which there were deliberations about main end-of-life therapy choices, White and colleagues found that physicians are most likely to give consideration to discussions concerning the anticipated useful status or quality of lifetime of the patient [28]. The instructional stage of the household, as properly as the degree of physician-family conflict about withdrawing life support, had been independently associated with the extent of prognostic data provided by the doctor. The crucial elements of doctor commu� A perception that God can alter the course of the nications with family members was exillness amined in a Seattle research of 4 completely different � A perception that predicting the longer term is inherently hospitals [29]. Strategies most likely to engender belief of treatment preferences were sources of and satisfaction with end-of-life decision making psychosocial help. Limerick interviewed 17 surrogate choice makers in a big Texas hospital system and developed a mannequin for the way typical surrogates make decisions for withholding and withdrawing of life-sustaining measures [31]. In different circumstances, physicians or the healthcare system itself might unilaterally require withholding or withdrawing futile medical interventions because of restricted sources (financial and physical).
Buy 500 mg cinalid free shippingThe feeling that one thing is lacking in the inside world and self, of not being a whole integrated personality, is properly described by Maria. Maria was 12 years old when she was hit by a motorbike whereas crossing the street. At the acute part, Maria had fractures within the left leg, which also remained shorter than the best. She skilled amnesia of the accident for no much less than a quantity of hours, however no loss of consciousness was reported. The poems are genuine experiences 226 Introduction to Neuropsychotherapy and were translated in to English from Finnish for this e-book by Maria herself. However, in neuropsychological therapy procedures, the use has not been as common. In neuropsychological rehabilitation, the neuropsychologist can use many strategies to deal with these symptoms. Neuropsychotherapy typically continues after the lively part of neuropsychological rehabilitation. In neuropsychotherapy, there are also many possibilities to use strategies from artwork remedy in dealing with still-existing neuropsychological issues. The manufacturing of art works recruits exercise from several brain areas and their functions: planning, motor management, hand�eye coordination, memory, long-term memory, ideas, semantic information of the world, emotional circuitry, the hippocampal formation of the parietal lobes, the management of which means and area, international and detailed notion, disembedding strategies, sustained attention, and different widespread neuronal networks, to name a couple of (Zaidel, 2005). Brain buildings provide different paths for accessing and processing visual and motor information and recollections, and artwork remedy is uniquely geared up to reap the advantages of these different paths and activate them via the use of varied artwork media in therapy (Lusebrink, 2004). An example of an art therapy methodology that may be very suitable to neuropsychotherapy is the Mai Color Glossary, developed within the Nineteen Seventies by Sarie Mai, a Canadian art therapist and nurse (Mai, 1987). It has been used with psychiatric sufferers, oncology sufferers, victims of sexual abuse, and in addition with scholar supervision (Mai, 1987; Trent, 1992). The primary premise is that every individual has his or her own shade and image preferences; during strong emotional experiences, these colors and symbols can change. The therapist should remain with the affected person all through the complete session to provide and promote therapeutic assist. Equipment needed are papers sized A4, a pencil and ruler, a color box with eight colours, felt-tip markers (blue, purple, yellow, green, black, purple, orange, and brown). The first sheet of paper consists of columns titled at the high of every column as "word," "color," and "symbol," and the remaining house titled as "written response," and horizontal lines with phrases for the word column one in every line ("pleased," "sad," "love," "angry," "fear," "ache," and "separation"); the words could also be tailored in accordance with the specific needs of the affected person. At the end of the assessment, the therapist will have an entire colour glossary that features colours, symbols, and a series of incidents that describe each feeling for that second. In the second part, the patient is requested to draw with pencil, on a second piece of paper, a full length image of him or herself and present where and the way in the physique, she or he experiences every of the seven stimulus phrases already used in the glossary; the same color alternative is given as earlier than. In the third task, the patient is given a choice of various artwork media and requested to create a picture utilizing one of many stimulus phrases each session; again she or he is requested to put him or herself in to each picture. This discussion is completed in an unstructured and nondirective method; the affected person frequently expresses different important related Summary of Applications of Psychotherapeutic Methods 229 experiences at these instances, and additional emotions that are aroused may be worked by way of presently. There are a few neuropsychological case examples with this method utilizing the primary task. The first case is a young woman, J, age sixteen, who suffered mind harm in a automotive accident. She got intensive neuropsychological rehabilitation and returned to high school after a few months, and he or she was in a position to continue her research properly. We continued neuropsychological rehabilitation with verbal rehearsals, and he or she began to communicate more in regards to the accident and what had occurred to her. He suffered brain harm in a sports accident, was paralyzed, and misplaced his speech capability firstly, however recovered slowly. When we first met for neuropsychological rehabilitation, he was already strolling without any equipment, however suffered difficulties in bodily balance; his speech was dysarthric, and he could use only simple words; his behaviour was quite impulsive. In his neuropsychological rehabilitation, there was need for verbal exercises but also need for impulse management exercises, which brought up his present feelings and feelings earlier than the accident, and the necessity for coping with them. He had at all times been very eager on totally different sports activities, however after his accident, returning to his life-style was not straightforward. The third case is a young man who sustained extreme brain injury in a motorbike accident when he was 15 years old; he had also many different traumas in his again and legs. He came to neuropsychological rehabilitation to prepare himself for attainable skilled training 230 Introduction to Neuropsychotherapy Do your individual color glossary assessment using the next seven feeling words-happy, sad, love, angry, pain and separation. The coronary heart is, after all, typical, although I suppose, the heart of a human being has not an enormous part in the love. Love purple Angry black Fear yellow Pain red Separation black Almost every little thing dealing with separation is darkish. The fourth case is an almost 30-year-old woman with brain damage from bicycle accident about five years prior. She was a proficient picture-maker, and he or she continued to process her emotions with new less-structured footage. Some, but not all, adults also have hyperactivity, which can be limited to feelings of restlessness. Amen (2001) has described specific forms of the disorder, which affect everyday behaviour. However, his general pointers are as follows: schooling, emotional and social assist, medicine, college and work strategies, pondering abilities, and training and self-regulation experiences (Amen, 2001). Neuropsychotherapeutic procedures and methods can be, as has been shown, cognitive�behavioral and/or neuropsychological, and data of the therapeutic components of the interpersonal process in addition to correct tools with which to work make intervention most fruitful. Case Study: Gabriella Gabriella is an instance of a young woman who got here to therapy at the age of 26, when her world was falling apart. All the years of her life had been very troublesome, but she had graduated from high school and wanted to make a profession after that, with no success up to now. She had unfinished coaching as a faculty assistant behind her, and when coming to remedy, she felt inferior in all fields of life. She had a compensatory objective of being a schoolteacher, but that was far past the chances when therapy started. She had a quantity of somatic problems-an consuming dysfunction, usually upset abdomen, and difficulties in getting activated normally for any type of daily work. No bus journey was attainable, and often she took her dog out through the evening, when the streets have been empty. We labored collectively for a complete of approximately eight years, together with breaks for a couple of months. Gabriella gained a more confident angle toward herself and strengthened her self-esteem. Eventually, she was able to take her canine to a canine park during the day, and to get to know different canine homeowners. No cognitive workouts had been wanted, but psychoeducation was an element in the interactive course of to construct up a practical picture of self for the affected person.
Side-Saddle Plant (Pitcher Plant). Cinalid. - Dosing considerations for Pitcher Plant.
- Digestive disorders, constipation, urinary tract diseases, fluid retention, preventing scar formation, pain, and other conditions.
- Are there safety concerns?
- What is Pitcher Plant?
- How does Pitcher Plant work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96145
Buy 100 mg cinalid fast deliveryThe caudad flap dissection ought to be continued till the inguinal ligament (Poupart) is clearly demonstrated. At this level either the nerve is carefully mobilized and retracted behind the cephalad flap of the exterior oblique aponeurosis or some surgeons favor to resect the nerve and allow the proximal finish to retract in to the internal indirect muscle fiber. Not all sufferers experienced numbness when this resection maneuver is carried out because of overlapping innervation. It is elevated off the pubic tubercle in its entirety along with its cremasteric fibers. The spermatic twine must be rigorously elevated from 2 em distal to the pubic tubercle all the greatest way to the inner ring. There are sometimes cremasteric fibers which would possibly be lateral and medial to the spermatic cord that require division in order to achieve full mobilization. Moderate to large direct hernias might present as a construction adherent to the undersurface of the spermatic twine. These hernias are easily separated and identified by elevating the spermatic twine anteriorly and sweeping the direct hernia posteriorly without violating the airplane of the cremasteric muscle. The anterior and medial portion of the cremasteric envelope of the spermatic wire is opened for three to 4 em within the line of its fibers. The hernia sac related to an indirect hernia is situated in this portion of the spermatic twine. After the completion of the exploration of the spermatic twine, the fioor of the inguinal canal is assessed by analyzing the transversalis fascia. These suspicions can be confirmed by examining the area outside of the extemal oblique simply medial to the femoral vein and palpitating for any suspicious lots suggesting femoral hernia. The construction represents the fusion of the internal indirect and transversus abdominis 11 opo. The caudal sutures are in the inguinal ligament and the cephalad sutures are in the conjoined tendon. If the hole is just too unfastened, then an additional suture is positioned till the right spacing is achieved. The shape of the mesh could be modified to leave a larger portion medially to merely tension-free coverage of the femoral area. Technique Variations in Women As in males, direct and oblique inguinal hernias are more widespread than femoral hernias in lady; however, the incidence of femoral hernias are larger in ladies than in males. This should alert the surgeon to be vigilant for this possibility and have a low threshold to open the transversalis fascia layer to inspect the femoral house. The presence of the spherical ligament instead of the spermatic wire requires some consideration as well. Some surgeons choose to ligate the spherical ligament within the preperitoneum with the concept future indirect hemia recurrence risk is lessened by closing the entire ground of the (inguinal) canal of Nook. In youthful girls, this could scale back the assist to the uterus and may not be advisable. The penrose drain around the spermatic wire is removed and the dissection of the spermatic twine is inspected for bleeding. This is confirmed after the drapes are removed and the scrotum is inspected at the finish of the case. The external indirect layar is closed by figuring out the new location of the exterior ring and suturing the aponeurosis collectively at this point with care to not make the ring too tight or catch a portion of the spermatic cord or ilioinguinal nerve in to the closure. This reduces rigidity on the testicle and will increase consolation in the postoparative period. Patients are given oral narcotic pain treatment and non-steroidal anti-intlammatory brokers for pain. Patients are advised to keep away from actually strenuous lifting for 6 weeks postoperatively. Critchlow Introduction Inguinal hernia restore is among the commonest operations carried out by basic surgeons, with roughly 750,000 operations done per year within the United States by surgeons who incorporate it as part of their various practices. Conventional open repairs without prosthetics are most often successful for small hernias. The quest has continued for a prosthetic restore which is speedy, safe, versatile, and easily taught. The patch/plug restore has thus been embraced by a lot of surgeons as their procedure of selection. The open preperitoneal approach described by Stoppa is type of efficient but includes intensive dissection in typically somewhat unfamiliar anatomy. The anterior method was addressed by Lichtenstein, whose work revolutionized herniorrhaphy within the United States. However, this method, which reinforces the entire ground of the inguinal canal without instantly addressing the defect, requires a meticulous closure with continuous sutures, and does expose the patient to some risk of recurrence via small gaps within the external restore, or because the first defect has not been bridged. Gilbert described the "sutureless" repair which was preperitoneal placement of a mesh patch to close the defect of an indirect hernia with an overlay just like that of Lichtenstein, but without sutures as the original defect had been addressed. Direct hernia defects have been bridged with a round plug adopted by an overlay to reinforce the floor and help to maintain the plug in place. Rutkow and Robbins developed an method to restore the first defect with a prosthetic material ("plug") and resurfacing the 25 2& Part I Open Inguinal Hernia entire flooring with mesh to forestall recurrence and to assist hold the plug in place. This method is applicable to direct and indirect hernias and has enjoyed tramandous success and is arguably the commonest repair done in the United States. It can be done quickly and effectively underneath local anesthesia with or with out sedation, permitting for protected repair in high danger sufferers with low recurrence rates. This is a very versatile approach and is adaptable to most all forms of hernias including the findings of an unsuspected femoral hernia or Pantaloon hernias. It is rapid and may most frequently be accomplished as an outpatient without general anesthesia. Some have argued that this can be a extra "minimally invasive" strategy to hernia repair than laparoscopy as it can be accomplished without common anesthesia, bladder catheterization, or intensive dissection violating the house of Retzius across the bladder and prostate which could complicate subsequent prostatectomy. This could be thought-about, but countered by glorious patient outcomes and that the tine factors of anatomy are sometimes misplaced on essentially the most junior trainees who do nearly all of these operations during residency. Aspirin ought to be stopped 10 days prior to the date of operation unless essential for prevention of significant coronary or vascular events. Non-steroidal anti-inflammatory drugs ought to be discontinued 24 to forty eight hours prior to operation. Prophylaxis for deep venous thrombosis is mostly not needed as most sufferers are carried out under sedation with local anesthesia until basic anesthesia is used in a patient at very excessive threat. These repairs are typically carried out underneath native anesthesia with sedation delivered by an anesthesiologist. Repair of hernias that are very large, recurrent or those in uncooperative sufferers are done beneath basic anesthesia. Intravenous antibiotics with good gram-positive coverage are administered, as graft materials is implanted. A nerve block can additionally be useful for intraoperative anesthesia and postoperative analgesia. A blunted 22 gauge needle is used in order that a "pop" could be felt because the needle penetrates by way of the external oblique fascia thus delivering the solution in the appropriate layer. This permits for publicity both the pubic tubercle and the ring by way of a really quick incision, which is hidden in the hairline.
Generic cinalid 250mg with visaWith both method, the test is constructive (attention deficit) when the score is <8 (three or more errors). A main technique for delirium prevention is to keep away from oversedation, stop and re-evaluate every day requirement, and consider the utilization of short-acting medication in case of frequent or steady administration. Clinical guidelines suggest using protocols and scales to enhance the dosage of sedatives and analgesics by maintaining the affected person calm and alert with lowest doses of sedative drugs. These manoeuvres may help us to reorient the affected person: promote the sleep-wake cycle, keep away from extreme noise and synthetic mild at evening time, minimize pain, encourage bodily therapy and early mobilization, early removal of catheters, optimize contact with the household, and promote visual and auditory stimulation, facilitate temporal-spatial orientation via the provision of eyeglasses, clock, calendar, music headset, radio, images of close relatives, favourite meals or objects. These interventions cut back by as a lot as 40% the incidence of delirium, and should be part of prevention and therapy methods. It is imperative to reverse shock, hypoxia, dehydration, abnormalities of sodium and glucose, thiamine replacement, establish a distended bladder or other causes of pain, and take away medicine (anticholinergics, corticosteroids) earlier than deciding on a selected drug. Health personnel and members of the family should preserve a non-confrontational dialogue with the patient, who displays altered opinion and perception, and to not exacerbate or trigger agitation. The best way is to listen and respond with attitudes directed to include general discomfort, displaying that he or she is in a protected environment. Physical restraint may be needed in instances of extreme agitation to prevent the patient from eradicating catheters, tubes or probes, and to stop damage to self or to the attending workers. It will always be a brief measure which shall be reassessed frequently whereas awaiting the motion of drug therapy. If not treated quickly, it can progress to microbial keratitis, corneal ulcers and subsequent loss of imaginative and prescient, all of which can have devastating effects on the next quality of life. The ocular floor in wholesome individuals is protected by pure defence mechanisms such as the bactericidal impact of the tear film, blinking and proper closure of the eyelids. Depression of consciousness, the usage of muscle relaxants and sedation in mechanically ventilated sufferers contributes to a scarcity of lid closure brought on by the decrease within the tonic contraction of the eye muscle tissue (lagophthalmos). The most generally studied strategies for the prevention of keratitis are the applying of lubricating drops and ointments, closing the eyes with duct tape, and humidity chambers. With the applying of easy protocols, keratopathies could be prevented and the care of coma sufferers improved. It is understood that the mind is enclosed in a inflexible case and has a excessive metabolic demand and irrigation, at a temperature roughly 1-2�C higher than the rest of the physique. So in a affected person with fever and neurological damage, the cerebral temperature is greater, with increased mind metabolism. The use of decrease thresholds for treating hyperthermia is really helpful in sufferers with intracranial hypertension, and every effort should be made to keep physique temperature <37. This is achieved by spraying the affected person with warm water or putting a sheet saturated with warm water over the patient and using a fan to promote evaporation. After 60 minutes, at which period the physique temperature should have decreased; the affected person must be dried and the sheets modified in order to not trigger different accidents. This manoeuvre should be performed as usually as needed till the temperature is decreased [32,33]. Other sources say that it should be positioned at the midpoint between the lateral canthus and the tragus of the ear. We suggest closed drainage techniques, at all times preserving the set open to the strain transducer for continuous monitoring, solely opening it after we want to perform therapeutic drainage. In common, minimum care ought to be performed once a day and any time the site is moist or soiled. It is preferable to place a bandage with a brimmed hat for optimum security of catheter fixation. A catheter that strikes or is dislodged will lead to greater morbidity, elevated threat of infection and better prices. The stopcock ought to be disinfected and sterile gloves used to maintain cleanliness of website drainage. First, you should disinfect the top of the stopcock with alcohol iodine for one minute. After donning the sterile gloves, open the system and place the highest of the stopcock on sterile gauze. Physicochemical analysis is then ordered for Gram staining and culture, glucose and lactic acid (>4 mg% suspected postoperative bacterial infection) determinations. Note the presence of fever and/or neurological deterioration not attributable to different causes. With a ventriculostomy we have to know the peak at which we ought to always place the drain. On the opposite hand, opening of drainage ought to be provided towards a optimistic strain that might be achieved by elevating the drip chamber above the zero stage, as many inches as specified by the neurosurgeon. If you see bubbles, shut the port that communicates with the affected person in the three-way stopcock closest to the pinnacle and flush the system with sterile saline answer from the same key to the collection bag. Always use aseptic method: antisepsis 3 minutes for the stopcock, sterile gloves and mask. They should solely be performed when the patient is satisfactorily resuscitated and hemodynamically stable. You ought to always calibrate the system on the degree of the foramen of Monro, whatever the place of the mattress or sofa. It is desirable that in switch the affected person receives the identical drug infusion as in the referring service to find a way to keep intracranial hemodynamics. The major goal of neurological evaluation is to detect any changes early during hospitalization and to keep away from overlooking a new mind damage or deterioration. It is important to keep in thoughts that neurological deterioration often occurs unnoticed, and time to treatment will determine its subsequent evolution. So the extra regularly you perform neurological analysis, the quicker the prognosis and remedy and the higher the evolution of those patients. Initial assessment of the extent of consciousness is critical for evaluating pupillary response and motor perform. A more full neurological examination should be carried out as a part of tertiary assessment. You ought to record what you see, avoiding the temptation to regulate the data to the medical historical past data. Another potential error is to not encourage patients sufficiently to acquire a true reflection of their neurological response. Always get hold of and report one of the best response and apply the dimensions as soon as the patient is stabilized, without evidence of cardiorespiratory instability (hypotension, hypoxemia, hypercapnia). You ought to communicate in a standard tone and, if needed, progressively increase the vol1697 Intensive Care in Neurology and Neurosurgery ume of your voice. Peripheral stimulus is delivered by making use of pressure with a pen on the lateral aspect of the second or third finger near the nail, rotating the point of stimulation at each assessment. In some cases a nociceptive stimulus is utilized to the finger nail mattress or stress on the sternum (rubbing it injures the tissues), however these stimuli can generate residual ache. A common mistake is "eye opening to the decision" when the affected person is physiologically asleep as a substitute of being depressed. If the patient was lately transferred from another hospital, he or she could have an understandable diploma of disorientation; nonetheless, a refined disorientation may be an early indicator of neurological impairment.
Purchase 100 mg cinalid visaPreceding an infection as necessary risk factor for ischemic mind infarction in younger and middle aged patients. The syndrome of inappropriate antidiuretic hormone secretion in tuberculous meningitis. Hyponatremic natriuretic syndrome in tuberculous meningitis: the probable position of arterial natriutetic peptide. Crit Care Clin 2001; 17: 125-38 1049 Intensive Care in Neurology and Neurosurgery seventy two. Acute hyponatraemia secondary to cerebral salt losing syndrome in a patient with tuberculous meningitis. Tuberculous meningitis complicated with hydrocephalus and cerebral salt wasting syndrome in a three-year-old boy. Cerebral infarction and cerebral salt losing syndrome in a patient with tuberculous meningoencephalitis. Acute symptomatic seizures: medical and etiological spectrum in developing international locations. Clinically necessary drug interactions in epilepsy: interactions between antiepileptic drugs and other drugs. Clinical significance of the interaction of phenytoin and isoniazid: a report from the Boston Collaborative Drug Surveillance Program. Continuous monitoring and intervention for cerebral ischemia in tuberculous meningitis. The impact of adjuvant steroid remedy on serial cerebrospinal fluid adjustments in tuberculous meningitis. Vascular endothelial progress issue and blood-brain barrier distruption in tuberculous meningitis. Shunt surgical procedure for poor grade sufferers with tuberculous meningitis and hydrocephalus: impact of response to exterior ventricular drainage and other components on long-term end result. Cerebral perfusion stress in central nervous system infections of infancy and childhood. Acute community-acquired bacterial meningitis in adults admitted to the intensive care unit: medical manifestations, administration and prognostic components. Cerebral perusion pressure-targeted strategy in kids with central nervous system infections and raised intracranial pressure: is it feasible Dev Med Child Neurol 1991; 33: 396-405 1051 Intensive Care in Neurology and Neurosurgery a hundred and ten. Am J rop Med Hyg 1998; fifty eight: 26-34 1052 59 Acinetobacter Infections: An Emerging Problem within the Neurosurgical Intensive Care Unit A. One of the main causes for the present increased curiosity on this genus is the emergence of multiresistant strains, a quantity of of that are pan-resistant to antibiotics and abruptly trigger an outbreak of an infection [1]. Multidrug-resistant Acinetobacter baumannii is a rapidly emerging pathogen within the healthcare setting, the place it causes infections together with bacteraemia, pneumonia, meningitis, urinary tract infections, and wound infections. The crude mortality fee related to bacteraemia is roughly 52% and that associated with pneumonia ranges from 23 to 73% [2,3]. It is among the most difficult antimicrobial-resistant Gram-negative bacilli to control and treat as a result of its capability to survive beneath a variety of environmental conditions and to persist for prolonged durations of time on surfaces, making it a frequent reason for outbreaks of an infection and an endemic healthcare-associated pathogen. This is an particularly extreme occasion in such infections as post-surgical meningitis as a end result of the choice of an antibiotic relies upon not solely on the sensitivity of A. Multidrug-resistance complicates the remedy of an infection, making the search of recent agents imperative and the return to old medication for optimal remedy of this multidrug-resistant organism. The focus of this evaluate is to summarize the present state of data relating to A. Subsequently, a number of adjustments were launched in to the taxonomic classification of Acinetobacter spp. The genus Acinetobacter initially en1053 Intensive Care in Neurology and Neurosurgery compassed a heterogeneous collection of non-pigmented, oxidase-positive and oxidase-negative Gram-negative rods [3,6-8]. Good growth happens at 40�C without the need for development elements, whereas nitrates are decreased only rarely [3]. It appears as bacilli in the course of the speedy progress phase and as cocobacilli in the stationary phase [9]. Some strains can survive environmental desiccation for weeks, a characteristic that promotes transmission through fomite contamination in hospitals [13]. In healthcare settings, colonized and contaminated patients are often the sources of A. Acinetobacter has been isolated from pasteurized milk, frozen foods, chilled poultry, foundry, and hospital air, vaporizer mist, tap water faucets, peritoneal dyalisate baths, bedside urinals, washcloths, door handles, keyboards, angiography catheters, ventilators, contaminated gloves, duodenoscopes, laryngoscope blades, plasma protein fraction, and hospital pillows [14-16]. This capacity to develop on medical tools and all through the hospital environmental emphasizes the need for special attention to disinfection [17-20]. Up to 25% of wholesome ambulatory adults exhibit cutaneous colonization and 7% of adults and children have transient pharyngeal colonization. Differentiating between colonization and an infection has medical and therapeutic relevance as a outcome of the presence of colonized or infected sufferers is essential in maintaining the organism in the hospital. Acinetobacter baumannii can cause community-acquired infections although less regularly than nosocomial infections. Multidrug-resistant Acinetobacter an infection has been reported amongst sufferers residing in rehabilitation and long-term care services, as properly as in acute care hospitals [24-26]. In addition to transmission, the emergence of resistance happens in the context of selective pressure from broad-spectrum antimicrobial remedy with carbapenems or thirdgeneration cephalosporins. The relative contribution of antimicrobial selective strain and transmission between sufferers to the emergence of multidrug-resistant Acinetobacter spp. The most typical definitions of multidrug resistance are carbapenem resistance or resistance to greater than three courses of antimicrobials [32]. The resistance rate varies between geographic areas, hospitals and even totally different hospital wards within the same hospital [34]. Some research [35] found sensitivity charges of imipenem and amikacin of almost 74% in North America and Europe, 60% and 23%, respectively, in Latin America, and sixty nine. In several nations, the speed of resistance to colistin is now 2-3% in relation to earlier use, and heteroresistant populations have emerged which might hinder its future use in monotherapy [41]. Although tigecycline as soon as appeared to be a great various to standard therapies, stories have increasingly described the emergence of resistant strains even during remedy with the drug, severely compromising its use in empirical remedy. Another latest research reported resistance charges of 25%, suggesting that the role of antibiotic remedy with these medication ought to be carefully evaluated [40]. Several risk factors for the acquisition of multidrug-resistant strains have been recognized. These embody the earlier use of antibiotic treatments, especially carbapenems and third-generation cephalosporins, adopted by quinolones, aminoglycosides and metronidazole, and the number of earlier antibiotics. The second most common threat 1055 Intensive Care in Neurology and Neurosurgery issue is using mechanical air flow. The most essential drawback in multidrug-resistant Acinetobacter is its resistance to carbapenems.
Buy cinalid 500 mg amexCumulative meta-analysis of aspirin efficacy after cerebral ischaemia of arterial origin. Dipyridamole for preventing stroke and other vascular events in patients with vascular illness. Thienopyridine derivatives versus aspirin for stopping stroke and different serious vascular events in high vascular threat sufferers. Aspirin noncompliance is the most important reason for "aspirin resistance" in patients undergoing coronary stenting. Incomplete inhibition of thromboxane biosynthesis by acetylsalicylic acid: determinants and effect on cardiovascular danger. J Neurol Neurosurg Psychiatry 1991; 54: 1044-54 1241 Intensive Care in Neurology and Neurosurgery forty four. Analysis of danger of bleeding issues after completely different doses of aspirin in 192,036 patients enrolled in 31 randomized controlled trials. The future of antiplatelet remedy: optimizing management in sufferers with acute coronary syndrome. Association of laboratory-defined aspirin resistance with a higher threat of recurrent cardiovascular occasions: a systematic evaluation and meta-analysis. Comparison of warfarin versus aspirin for the prevention of recurrent stroke or dying: subgroup analyses from the Warfarin-Aspirin Recurrent Stroke Study. An updated review of its pharmacology and therapeutic use in platelet-dependent disorders. Lancet 1989; 1: 1215-20 1242 Antithrombotic Therapy for Secondary Stroke Prevention sixty three. Aspirin and ticlopidine for prevention of recurrent stroke in black sufferers: a randomized trial. Clopidogrel and modified-release dipyridamole for the prevention of occlusive vascular events. Cytochrome P450 2C19 polymorphism in younger patients treated with clopidogrel after myocardial infarction: a cohort research. Pharmacodynamic effect and scientific efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Platelet reactivity after clopidogrel therapy assessed with point-of-care analysis and early drug-eluting stent thrombosis. Combination antiplatelet therapy for secondary stroke prevention: enhanced efficacy or double bother Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. Secondary prevention of stroke and transient ischemic assault: is more platelet inhibition the answer Effect of addition of clopidogrel to aspirin on mortality: systematic review of randomized trials. Dipyridamole for stopping recurrent ischemic stroke and different vascular events: a meta-analysis of individual patient information from randomized managed trials. Trends in utilization of alternative antiplatelet remedy after stroke and transient ischemic attack. Cilostazol versus aspirin for secondary prevention of vascular occasions after stroke of arterial origin. Antiplatelet remedy in elderly people with transient ischaemic attacks or ischaemic strokes. Cilostazol as a substitute for aspirin after ischaemic stroke: a randomised, double-blind, pilot examine. Cilostazol in secondary prevention of stroke: impact of the Cilostazol Stroke Prevention Study. Oral antiplatelet remedy in cerebrovascular illness, coronary artery illness, and peripheral arterial disease. Prescribing antiplatelet medicine and subsequent occasions after intracerebral hemorrhage. Efficacy and safety of anticoagulant therapy in acute cardioembolic stroke: a meta-analysis of randomized controlled trials. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind 1245 Intensive Care in Neurology and Neurosurgery randomised examine. Safety and value of low-molecular-weight heparin as bridging anticoagulant therapy in subacute cerebral ischemia. Antithrombotic and thrombolytic remedy for valvular disease: Antithrombotic Therapy and Prevention of Thrombosis, ninth ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Cost-effectiveness of antiplatelet agents in secondary stroke prevention: the bounds of certainty. Methodology for the event of antithrombotic remedy and prevention of thrombosis guidelines: Antithrombotic Therapy and Prevention of Thrombosis, ninth ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Canadian Cardiovascular Society atrial fibrillation pointers 2010: prevention of stroke and systemic thromboembolism in atrial fibrillation and flutter. Stroke patients with atrial fibrillation have a worse prognosis than sufferers without: data from the Austrian Stroke registry. Independent predictors of stroke in patients with atrial fibrillation: a scientific evaluate. Selecting sufferers with atrial fibrillation for anticoagulation: stroke danger stratification in sufferers taking aspirin. Anticoagulants for preventing stroke in sufferers with nonrheumatic atrial fibrillation and a historical past of stroke or transient ischaemic assault. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Placebo-controlled, randomised trial of warfarin and aspirin for prevention of thromboembolic problems in persistent atrial fibrillation. Primary prevention of arterial thromboembolism in non-rheumatic atrial fibrillation in main care: randomised controlled trial evaluating two intensities of coumarin with aspirin. Comparative effects of antiplatelet, anticoagulant, or mixed therapy in patients with valvular and nonvalvular atrial fibrillation: a randomized multicenter study. Primary prevention of arterial thromboembolism within the oldest old with atrial fibrillation-a randomized pilot trial evaluating adjusted-dose and glued low-dose coumadin with aspirin. The randomized research of efficiency and security of antithrombotic therapy in nonvalvular atrial fibrillation: warfarin in contrast with aspirin. Symptomatic hemorrhagic transformation and its predictors in acute ischemic stroke with atrial fibrillation. Eur Neurol 2010; 64: 193-200 1247 Intensive Care in Neurology and Neurosurgery 146. Risk of early demise and recurrent stroke and impact of heparin in 3169 sufferers with acute ischemic stroke and atrial fibrillation in the International Stroke Trial. Meta-analysis to assess the standard of warfarin management in atrial fibrillation patients within the United States. Warfarin for the prevention of systemic embolism in sufferers with non-valvular atrial fibrillation: a meta-analysis. Heart 2008; 94: 1607-13 1248 Antithrombotic Therapy for Secondary Stroke Prevention a hundred and sixty. Oral anticoagulants for stopping stroke in patients with nonvalvular atrial fibrillation and no previous history of stroke or transient ischemic attacks.
Generic 500 mg cinalid amexReversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover examine in healthy topics. Circulation 2011; 124: 1573-9 1250 Antithrombotic Therapy for Secondary Stroke Prevention 193. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation is dependent upon the quality of worldwide normalized ratio control achieved by centers and countries as measured by time in therapeutic vary. Net clinical advantage of including clopidogrel to aspirin remedy in sufferers with atrial fibrillation for whom vitamin K antagonists are unsuitable. Stroke and thromboembolism in atrial fibrillation: a scientific evaluation of stroke danger elements, danger stratification schema and price effectiveness information. Transcatheter closure versus medical remedy of patent foramen ovale and presumed paradoxical thromboemboli: a systematic review. Occurrence of post-acute recanalization and collateral formation in sufferers with cerebral venous and sinus thrombosis. Mechanical thrombectomy as first-line treatment for venous sinus thrombosis: technical considerations and preliminary outcomes using the AngioJet gadget. Improving affected person choice for coagulopathy testing within the setting of acute ischemic stroke. Anticoagulation for the long-term treatment of venous thromboembolism in patients with most cancers. Antiplatelet remedy for preventing stroke in patients with nonrheumatic atrial fibrillation and a historical past of stroke or transient ischemic assaults. The sin of omission: a scientific evaluation of antithrombotic therapy to prevent stroke in atrial fibrillation. Anticoagulants versus antiplatelet therapy for stopping stroke in sufferers with nonrheumatic atrial fibrillation and a historical past of stroke or transient ischemic assault. Progress in medicine has elevated the number of patients who survive severe acute mind harm. Classically vegetative state follows a coma; after 1 month the time period "persistent vegetative state" is used; after three months (non-traumatic insult) or 1 year (traumatic insult) some authors use the term "permanent vegetative state" which suggests no likelihood of restoration. Bedside evaluation of residual brain perform in severely brain-damaged patients is tough because motor responses could additionally be very restricted or inconsistent. The vegetative state (blue) is a novel persistent dissociated state of consciousness. Arousal is supported by several brainstem neuronal populations that instantly project to each thalamic and cortical neurons [9]. Therefore melancholy of either brainstem or each cerebral hemispheres might cause reduced wakefulness. Awareness is thought to be dependent upon the practical integrity of the cerebral cortex and its reciprocal subcortical connections; every of its many features resides to some extent in anatomically defined areas of the mind [10-12]. Many scoring methods have been developed for a standardized assessment of consciousness in severely mind damaged sufferers (For evaluate see [13]). A simplified scheme of consciousness and its two main parts: arousal and awareness. Note: the grey space represents the reticular activating system encompassing the brainstem and thalamus; the arrow close to the brainstem denotes the progressive disappearance of brainstem reflexes during rostral-caudal deterioration. Clinical Definitions Survivors of severe traumatic or hypoxic-ischemic mind injury classically go through completely different clinical entities before partially or absolutely recovering consciousness. After some days to weeks, comatose sufferers who recuperate will ultimately open their eyes. When this return of "wakefulness" is accompanied by reflexive motor exercise solely, devoid of any voluntary interaction with the environment, the situation known as a vegetative state. Brain Death the idea of brain dying as defining the demise of the person is basically accepted [14]. Most countries have printed recommendations for the analysis of brain dying but the diagnostic criteria differ from nation to nation [15]. Some rely on the death of the brainstem solely [16] others require demise of the entire brain together with the brain stem [17]. However, the clinical assessments for brain demise are very uniform and based on the loss of all brainstem reflexes and the demonstration of constant cessation of respiration in a persistently comatose affected person [procedures of a standardized apnea take a look at could be found in 18]. There should be an evident reason for coma and confounding components (including hypothermia, medication, electrolyte, and endocrine disturbances) ought to be excluded. A repeat analysis in 6h is advised, but the time period is taken into account arbitrary [19]. It is a state of unarousable unresponsiveness in which the affected person lies with the eyes closed and has no awareness of self and environment. To be clearly distinguished from syncope, concussion, or different states of transient unconsciousness, coma must persist for at least one hour. In general, comatose sufferers who survive start to awaken and recover progressively within 2 to 4 weeks. Jennett and Plum cited the Oxford English Dictionary to make clear their alternative of the time period "vegetative": to vegetate is to "stay merely a physical life devoid of mental exercise or social intercourse" and vegetative describes "an natural physique capable of growth and improvement however devoid of sensation and thought". Even after these long and arbitrary delays, some distinctive patients could show some limited recovery. It is important to set up repetitively the formal absence of any signal of conscious notion or deliberate motion earlier than making the analysis. On this analysis will indeed rely, not only the therapeutic surgical or medical selections, but additionally typically cares limitation. Before the event and the diffusion of the scales of coma and particularly of the size of Glasgow [30], the analysis of the affected person presenting with altered consciousness was primarily based on a rather vague nomenclature. The description of the depth of coma was made via phrases often imprecise corresponding to: drowsy, comatose, somnolent, obtunded, obnubilated, obstreperous or combative. From these efforts had been born the primary classifications for altered consciousnesses states [32]. The neurosurgical literature on head injuries sustained in the Vietnam conflict categorised their initial state in three grades, variously defined [33,34]. These classification suffered from their lack of precision and from the therefore ambiguity of the terms employed. This type of classification must be deserted for the assessment of altered consciousnesses. These authors took particular care to the development of their scale to overcome the ambiguities that arose when details about comatose sufferers was offered and teams of sufferers in contrast. Among the aims of its originators, there was the desire to set up an evaluation tool based on simple, clear, unambiguous gadgets that could be easily translated in varied languages. Moreover, the scale had to be utilizable in a dependable method not only by any physician but additionally by nurses and paramedics. Eye Opening Eye opening in response to pain must be examined by stimulation on the stage of the limbs, as a end result of the grimacing related to supra-orbital or jaw-angle stress might cause eye closure. The eye opening either spontaneously or on stimulation defines the transition from coma to vegetative state.
References - Probst, A. M., & Laufer, M. R. (1999). Endometriosis in adolescents. Incidence, diagnosis and treatment. Journal of Reproductive Medicine, 44, 751.
- Bruinsma SM, Roobol MJ, Carroll PR, et al; Movember Foundationis Global Action Plan Prostate Cancer Active Surveillance (GAP3) consortium: Expert consensus document: semantics in active surveillance for men with localized prostate cancer - results of a modified Delphi consensus procedure, Nat Rev Urol 14(5):312n322, 2017.
- Djurhuus JC, Sorensen SS, Jorgensen TM, et al: Predictive value of pressure flow studies for the functional outcome of reconstructive surgery for hydronephrosis, Br J Urol 57(1):6n9, 1985.
- Veening JG, Coolen LM: Neural mechanisms of sexual behavior in the male rat: emphasis on ejaculation-related circuits, Pharmacol Biochem Behav 121:170n183, 2014.
- Morsman B, Gee J: Asbestos-related diseases. N Engl J Med 320: 1721, 1989.
|
|