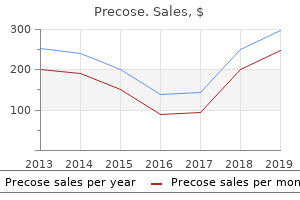
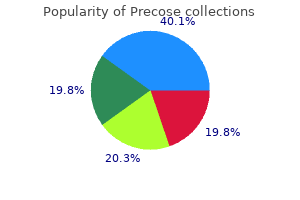
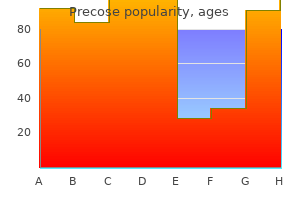
"Buy precose paypal, diabetes mellitus x doença periodontal."By: Peter Bartlett Bressler, MD - Associate Professor of Medicine
 https://medicine.duke.edu/faculty/peter-bartlett-bressler-md
Order precose 50mg without prescriptionToday, menstruating women proceed to be among the more than likely people to develop iron deficiency, together with young kids whose development outstrips their iron provide. An understanding of normal iron physiology is essential to best respect the pathophysiology of iron deficiency anemia. Full-term infants start life with roughly seventy five mg/kg physique weight of iron, primarily acquired from their moms in the course of the third trimester of gestation. These ample stores are quickly depleted over the primary few months of life, and most young youngsters have tenuous iron steadiness, as their consumption must keep pace with fast development. Requirements decrease after adolescence, and males have a small gradual enhance in iron stores throughout life. In contrast, postpubertal ladies have increased losses of iron as a outcome of menstruation, being pregnant, and childbirth, leading to a body iron endowment averaging 35 mg/kg. Most of the physique iron is found in heme-containing oxygen transport and storage proteins, together with hemoglobin and myoglobin (Table 23. Smaller quantities are integrated into enzymes with energetic websites containing heme or iron�sulfur clusters, together with enzymes of electron transport chain, peroxidases, catalases, and ribonucleotide reductase. Most nonheme iron (approximately 1 g in adult men) is saved as ferritin or hemosiderin in macrophages Ta bl E 2 3. The remainder is utilized by the cell or integrated into ferritin,23 an intracellular iron storage protein discussed in a later section. Complete ablation of ferroportin in mice, together with extraembryonic tissues, resulted in embryonic dying,28 whereas selective inactivation that preserved placental ferroportin expression resulted in reside births, demonstrating the important operate of ferroportin in materno-fetal iron transfer. Ferroportin can also be important for systemic iron homeostasis as inactivation of ferroportin in all tissues in mice other than placenta led to the event of extreme anemia resembling iron deficiency, and stemmed from the shortcoming to mobilize iron from enterocytes, macrophages, and hepatocytes. Ferroportin exports Fe2+ and this iron must be oxidized to its Fe3+ type to bind to transferrin. A membrane-bound multicopper oxidase, hephaestin, has been implicated in this process. Mice carrying a big deletion in the X-chromosomal hephaestin gene29 have impaired placental iron transfer and decreased intestinal iron absorption. The easiest interpretation is that hephaestin is important in placental iron transport but dispensable for intestinal iron uptake. The useful relationship between hephaestin and ferroportin has not but been defined intimately. On the premise of long-term studies of physique iron turnover, the total average daily lack of iron has been estimated at 1 to 2 mg in normal grownup males and nonmenstruating girls. Menstruating girls lose an extra, extremely variable amount over every menstrual cycle, from zero. Fractional absorption of dietary iron can increase as much as three- to fivefold (3 to 5 mg/day) if iron stores are depleted. Thus, iron stability is primarily, if not solely, achieved by management of absorption rather than by management of excretion. Intestinal absorption Iron is absorbed in the duodenum, and humans and other omnivorous mammals have at least two distinct pathways for iron absorption: one for uptake of heme iron and another for ferrous (Fe2+) iron. Heme iron is derived from hemoglobin, myoglobin, and other heme proteins in foods of animal origin, representing roughly 10% to 15% of iron content material within the typical Western diet,9 although heme-derived iron accounts for 2/3 of absorbed iron in meat-eating humans. Exposure to acid and proteases current in gastric juices frees the heme from its apoprotein. Dietary constituents may have profound effects on the absorption of nonheme iron, making the bioavailability of meals iron extremely variable. Both systemic mechanisms and native mechanisms within enterocytes (discussed later in the chapter) regulate dietary iron uptake. The figure shows a drawing of an absorptive enterocyte from the proximal duodenum. Within the cell, some iron is saved, and some is transported throughout the basolateral membrane. Hephaestin, a ferroxidase, facilitates basolateral iron export, presumably by oxidizing the iron as it exits the cell to the Fe3+ form to bind to plasma apotransferrin. Hepcidin binds to the iron exporter ferroportin, causing ferroportin endocytosis and lysosomal degradation,41 and leading to cessation of cellular iron export. Thus, hepcidin instantly and coordinately controls the entry of iron into the plasma from ferroportin-expressing cells, including absorptive cells of the gut and tissue macrophages. Alterations in hepcidin production lead to modifications in iron absorption and recycling. Multiple indicators are identified to regulate hepcidin expression, together with iron, erythropoiesis, inflammation, and growth elements. As with different hormones which are feedback regulated by the substances whose concentration they control, hepcidin expression is controlled by iron. When iron is poor, hepatocytes produce much less hepcidin, allowing extra iron to enter plasma. When iron is ample, hepcidin production increases, limiting additional iron absorption and launch from stores. In human volunteers ingesting a single dose of oral iron, hepcidin concentrations in urine increased within a quantity of hours and have been proportional to the increase in transferrin saturation. This is observed in efficient in addition to in ineffective erythropoiesis when erythroid precursors are destroyed comparatively near their site of origin within the bone marrow (as seen in thalassemia syndromes, congenital dyserythropoietic anemias, and sideroblastic anemias). It is now identified that the hormone hepcidin functions as each the shops and erythroid regulator. Hepcidin is a small peptide of 25 amino acids, produced in the liver, secreted into the plasma, and excreted by way of the kidneys. Hepcidin controls the entry of iron into plasma by causing degradation of its receptor, the iron exporter ferroportin. The main iron flows that are regulated by hepcidin�ferroportin interactions include the discharge of iron from macrophages that recycle iron in the spleen and the liver, dietary iron absorption in the duodenum, and, a minimum of in part, the release of iron from storage in hepatocytes. The feedback stimulation of hepcidin by plasma holotransferrin and iron stores ensures that extracellular iron concentration and iron stores stay inside regular limits. Hepcidin synthesis is suppressed by erythropoietic activity, guaranteeing a sufficient provide of iron to the bone marrow when demand for hemoglobin synthesis is high. During inflammation, hepcidin manufacturing is stimulated and iron entry into plasma is inhibited, causing the hypoferremia and anemia of irritation. As already mentioned, hepcidin synthesis additionally increases in response to saved intracellular iron in hepatocytes however the underlying mechanism is but unclear. Hepcidin synthesis, and consequently absorption of iron and its availability for erythropoiesis, is also regulated by erythropoiesis itself. Increased erythropoietic activity due to bleeding, hemolysis, or administration of erythropoietin in humans or mice causes hepcidin suppression. The severe suppression of hepcidin, particularly in untransfused b-thalassemia, results in elevated iron absorption and the development of lethal iron overload. In the iron-regulated pathway, extracellular iron in the form of holotransferrin (HoloTf) is sensed by the 2 transferrin receptors (TfR1 and TfR2). A fraction of the filtered hepcidin is excreted into urine, and urinary hepcidin concentrations are proportionate to plasma hepcidin ranges in wholesome subjects. At least two mechanisms have been described: one associated to the enterocyte iron levels and the other to the hypoxia pathway.
Order discount precose on lineHpr is poorly expressed in contrast with Hp, with approximately tenfold decrease levels within the serum. These considerably conflicting results illustrate the numerous variations in the haptoglobin genes, haptoglobin expression regulation and haptoglobin and hemoglobin clearance that exist between rodents and people, differences believed to be as a outcome of the evolutionary strain on primates from prevalent hemolytic illnesses such as malaria and trypanosomiasis. Thus, the level of circulating haptoglobin is an important determinant of the obvious renal threshold. As discussed, hepatic parenchymal cells are responsible for removal of some of the free hemoglobin from plasma. When iron-laden tubular cells are sloughed into the urine, the urine iron focus increases and both ferritin and hemosiderin could additionally be detected. With time, Hp-deleted animals accumulate hemoglobin-derived iron within the proximal tubular cells of the kidneys. Notably, the redistribution of iron from the liver to the kidney with deletion of Hp ameliorates the hepatic iron loading noticed in a mouse mannequin of hereditary hemochromatosis. It binds heme with the best known affinity of any heme-binding protein (Kd < 1 pM) and performs an important function in receptor-mediated hepatocyte heme uptake. Heme sits in a pocket formed between the 2 domains and the linker protein with the heme iron coordinated to a histidine residue within the linker area and one other in the C-terminal area. In addition to heme, hemopexin also can bind other porphyrins and bilirubin, however with much less avidity. The every day manufacturing of bilirubin in people is roughly four hundred mg, of which roughly 300 mg is derived from the breakdown of hemoglobin,635 with the rest derived from catabolism of other hemoproteins, corresponding to cytochromes, catalase, and myoglobin. Interestingly, in animals with deletion of Hp or hemopexin the expression of the opposite protein is up-regulated as a compensatory mechanism,628 perhaps by heme. Analysis means that with acute hemolysis massive quantities of hemoglobin and/or heme are deposited in the liver and the splenomegaly seems to be related to purple cell congestion. The enzyme is also induced by hormones, various medication, fever, hunger, and stress. In addition to catalyzing the discount of biliverdin to bilirubin, biliverdin reductase has kinase, transcription issue, and intracellular heme transport activities. The intramolecular hydrogen bonding that happens with the Z,Z configuration is less extensive in the geometric isomers designated E,Z, and E,E (not shown); therefore, the latter are extra soluble in water. Very excessive von Willebrand issue and thrombomodulin levels with proof of disseminated intravascular coagulation had been observed, suggesting widespread endothelial damage. There was iron overload of the liver (involving both Kuppfer cells and parenchymal cells) and kidney (proximal tubule cells). Bilirubin Transport After release from sites of heme catabolism, bilirubin seems within the plasma. At equilibrium, the concentration is instantly associated to bilirubin manufacturing (mostly from erythropoiesis and pink cell destruction) and inversely associated to hepatic clearance. If either outer ring is rotated, then the E,Z or Z,E geometric isomers are fashioned. Photoisomerization of the Z,Z configuration of bilirubin ends in formation of these extra soluble photoisomers, which may be excreted without conjugation. At normal plasma albumin concentrations, the theoretical bilirubin-binding capacity is approximately 70 mg/dl, of which half is tightly bound. These values are decreased by a decrease in plasma albumin focus or by the presence of organic anionic substances that compete for albumin-binding sites, similar to heme, fatty acids, sulfonamides, and salicylates. Most is much less tightly sure than the unconjugated kind, however a portion is covalently and irreversibly bound. The normal pathways (solid arrows) embody uptake and conjugation of bilirubin and excretion of the conjugated by-product. Abnormal pathways (dashed arrows) include regurgitation of bilirubin glucuronide into plasma and excretion of unconjugated bilirubin into bile. Hepatic bilirubin metabolism is divided into three distinct phases: uptake, conjugation, and excretion635. All three phases are essential for bilirubin to be excreted at a traditional rate; however, the excretion step is often the slowest, and subsequently the rate-limiting, step. Little or no unconjugated bilirubin is found in bile, and if conjugation is impaired, bilirubin content is low. In addition, a small portion of conjugated bilirubin throughout the hepatocyte is deconjugated and may reflux into the plasma. In different scientific situations, hyperbilirubinemia is mainly due to an increase in unconjugated bilirubin. The commonest of these is hemolytic illness, where hemoglobin catabolism and thus bilirubin production are elevated. However, inherited disorders may also trigger unconjugated hyperbilirubinemia due to an impaired capacity for bilirubin conjugation. In the two Crigler-Najjar syndromes, the mutation incessantly includes exon 1, which confers substrate specificity to the enzyme, leading to a structurally irregular protein. In Crigler-Najjar kind I, the heme oxygenase inhibitor Sn-protoporphyrin could also be efficient in decreasing bilirubin ranges. The diploma of hyperbilirubinemia seen in kids with persistent hemolytic states is influenced by simultaneous inheritance of the gene for Gilbert illness. Traditionally, it has been measured by the van den Bergh take a look at in which a mixture of sulfanilic acid, hydrochloric acid, and sodium nitrite (diazo reagent) yields a reddish-violet color with a most absorption at 450 nm when added to plasma or different solutions containing bilirubin. Detection of the unconjugated bilirubin found in plasma of sufferers with hemolytic disease requires addition of an accelerator, corresponding to alcohol (indirect reaction). In situations where bilirubin production could additionally be increased and the bilirubin load is likely excessive, precise measurements of heme catabolism can be determined by measuring endogenous bilirubin manufacturing or generation of carbon monoxide (produced in equimolar quantities throughout heme breakdown). Bilirubin diglucuronide most likely stays conjugated throughout its transit via the small intestine. However, with intestinal stasis, and in newborns, elevated deconjugation occurs and intestinal absorption happens. This enterohepatic circulation of bilirubin may contribute to the severity of jaundice associated with the physiologic hyperbilirubinemia of the new child. The methine bridges and usually the vinyl teams are then lowered by bacterial flora forming colorless tetrapyrroles referred to as urobilinogens. The urobilinogens are easily dehydrogenated to type the orange-yellow pigments, urobilins, which contribute to the colour of feces. The reabsorbed fraction is effectively excreted by the normal liver with out being conjugated. Urobilinogen is filtered by the glomerulus, secreted by the renal tubule, and reabsorbed. Emmanuel Dessypris, Stephen Sawyer, and Marilyn Telen to the chapters masking this content material in the earlier edition of this textbook.
Buy precose paypalIn mouse fashions, loss of Fli1 suppresses megakaryopoiesis, whereas overexpression of Fli1 promotes megakaryocyte development whereas suppressing erythropoiesis. In megakaryocytes, miR155 expression is reduced as cells differentiate toward megakaryocytes, and overexpression of miR-155 inhibits megakaryopoiesis in in vitro and mouse fashions, potentially by focusing on Meis1 and Ets1 transcripts. Down-regulation of c-Myb promotes megakaryocytic differentiation at the expense of erythroid cells. Genetic elimination of c-mpl or tpo in mice results in profound thrombocytopenia due to a greatly decreased variety of megakaryocyte progenitors and mature megakaryocytes and the reduced polyploidy of the remaining megakaryocytes. ChaPtEr 15 Megakaryocytes are highly associated,301,302 and the receptors for the 2 cytokines share a typical subunit. Notch signaling is initiated when the extracellular portion of a Notch receptor binds certainly one of its cognate ligands, resulting in proteolytic cleavage that releases the intracellular domain of Notch from the membrane, permitting it to translocate to the nucleus and stimulate gene transcription. Although previously acknowledged for its position in T-cell development, Notch has extra recently been proven to specify megakaryocyte growth from hematopoietic stem and progenitor cells. The extracellular area is N-glycosylated, enhancing receptor secretion and cell floor expression. As ought to be clear from the earlier discussion, the megakaryocyte (and in all probability all hematopoietic cells) uses a number of molecular pathways to have an effect on cell survival and proliferation. Recent work with c-Mpl has helped to clarify the character and teleology behind this seeming redundancy. As mentioned above, following initiation of signaling, the ligated c-Mpl is internalized and degraded. In the absence of Lnk, mice exhibit thrombocytosis and over time develop a myeloproliferative dysfunction. Akt is a serine-threonine kinase with multiple targets that have roles in cell survival and development. Additional skeletal and nonskeletal defects are frequent, including decrease extremity, cardiac, renal, and gastrointestinal abnormalities. Granule Disorders: the study of disorders involving platelet a-granules (gray platelet syndrome) or dense granules (Hermansky Pudlak syndrome) has supplied insights into the mobile mechanisms involved in granule formation within the megakaryocyte. In Hermansky Pudlak syndrome, defects in the biogenesis and trafficking of lysosome-related organelles, including melanosomes and platelet dense granules, underlie the hypopigmentation and bleeding manifestations attribute of the disorder. The mutation Ser505Asn inside the transmembrane area of c-Mpl was identified in a big Japanese household with thrombocytosis, and the mutant c-Mpl was proven to confer cytokine independence in a Ba/F3 cell line. Although inheritance is X-linked, a gentle phenotype due to skewed X-inactivation in female family members has been described. This dysfunction resembles kind 2B von Willebrand illness and is called platelet-type von Willebrand illness. Lnk negatively regulates self-renewal of hematopoietic stem cells by modifying thrombopoietin-mediated signal transduction. Characterization of a bipotent erythromegakaryocytic progenitor in human bone marrow. Endomitotic megakaryocytes that kind a bipolar spindle exhibit cleavage furrow ingression adopted by furrow regression. Megakaryocyte endomitosis is a failure of late cytokinesis related to defects in the contractile ring and Rho/Rock signaling. Role of RhoA-specific guanine exchange factors in regulation of endomitosis in megakaryocytes. Characterization of the megakaryocyte demarcation membrane system and its role in thrombopoiesis. Distinct platelet packaging, release, and floor expression of proangiogenic and antiangiogenic components on totally different platelet stimuli. Blood platelets are assembled principally on the ends of proplatelet processes produced by differentiated megakaryocytes. Mechanisms of organelle transport and seize along proplatelets throughout platelet production. Promotion of megakaryocyte progenitor expansion and differentiation by the c-Mpl ligand thrombopoietin. Caspase-9 mediates the apoptotic demise of megakaryocytes and platelets, however is dispensable for their generation and performance. Megakaryocytes possess a practical intrinsic apoptosis pathway that should be restrained to survive and produce platelets. Mef2C is a lineage-restricted goal of Scl/Tal1 and regulates megakaryopoiesis and B-cell homeostasis. The c-Mpl ligand (thrombopoietin) stimulates tyrosine phosphorylation of Jak2, Shc, and c-Mpl. Dissecting the thrombopoietin receptor: practical components of the Mpl cytoplasmic domain. Megakaryocytic differentiation induced by constitutive activation of mitogen-activated protein kinase kinase. Control of thrombopoietininduced megakaryocytic differentiation by the mitogen-activated protein kinase pathway. Fetal anemia and apoptosis of pink cell progenitors in Stat5a-/-5b-/- mice: a direct role for Stat5 in Bcl-X(L) induction. Two patterns of thrombopoietin signaling suggest no coupling between platelet production and thrombopoietin reactivity in thrombocytopenia-absent radii syndrome. Complex inheritance pattern resembling autosomal recessive inheritance involving a microdeletion in thrombocytopenia-absent radius syndrome. FlnA-null megakaryocytes prematurely release massive and fragile platelets that circulate poorly. Platelet-type von Willebrand disease: a uncommon, often misdiagnosed and underdiagnosed bleeding dysfunction. Autoinhibition of Jak2 tyrosine kinase relies on particular areas in its pseudokinase domain. An activating splice donor mutation within the thrombopoietin gene causes hereditary thrombocythaemia. A lineage-restricted and divergent betatubulin isoform is essential for the biogenesis, construction and performance of blood platelets. Gata2, Fli1, and Scl kind a recursively wired gene-regulatory circuit throughout early hematopoietic improvement. Fli-1 is required for murine vascular and megakaryocytic improvement and is hemizygously deleted in patients with thrombocytopenia. Thrombopoietin (c-mpl ligand) acts synergistically with erythropoietin, stem cell issue, and interleukin-11 to enhance murine megakaryocyte colony development and will increase megakaryocyte ploidy in vitro. The reciprocal relationship of thrombopoietin (c-Mpl ligand) to changes in the platelet mass during busulfan-induced thrombocytopenia in the rabbit.
Buy generic precose 50 mg lineDuring the ovulatory period, eosinopenia and a slight rise in the number of leukocytes, in addition to elevated 17-hydroxycorticosteroid levels, have been reported. This state continues for 1 day after supply, receding to regular only after 4 or 5 days. These adjustments are accompanied by a discount in the variety of circulating eosinophils. The administration of cortisone or hydrocortisone ends in increased blood ranges of 17-hydroxycorticosteroids that peak at 1 hour384 and are associated with neutrophilia. Neutrophilia was much less fixed than the depression in eosinophil and lymphocyte numbers but might be caused by a steroid hormone�mediated decreased efflux of neutrophils from the blood and increased cell launch from the bone marrow. The nature of those management mechanisms is complicated, however several control factors exist: recruitment of pluripotent stem cells and their induction into committed stem cells, stimulation (and perhaps inhibition) of stem cell and myeloid proliferative cell growth, and selective launch of cells from the marrow. Blood cell development is discussed in Chapter 5 and is only briefly discussed right here. Pluripotent stem cells are principally within the G0 state and must be induced into actively proliferating committed stem cells. Hematopoietic cell growth and development are normally restricted to certain tissues. In studies of perfused rat hind limbs, the release of neutrophils from the marrow into the blood420 increased with a rise in perfusion flow rate or with a low leukocyte content material of the perfusate. This neutrophilia-inducing activity was qualitatively dissimilar from that famous after endotoxin, epinephrine, or cortisone administration and acted by inflicting launch of marrow cells. The outcomes of those research suggest that an endogenously produced humoral factor causes neutrophil release from the marrow. To accomplish this task, the neutrophil must first sense infection, migrate to the site of the infecting organism, and then destroy the infectious agents. Thus, though in some cases neutrophils in blood might respond to a stimulus by adhering to different blood cells or overseas our bodies, corresponding to bacteria or biomaterials, the usual first step of the neutrophil after sensing an inflammatory stimulus is to adhere more strongly to the blood vessel wall. After adhesion to the endothelial surface, the neutrophil follows a gradient of chemotactic elements to the positioning of an infection and interacts with the organisms. This destruction is mostly accomplished by phagocytosis of the agent adopted by release of granules into the phagocytic vesicle, followed by killing of the organism. The mechanisms by which these phenomena happen are very complex and never utterly understood. White, creamy pus, due to the presence of many neutrophils, suggested a better end result than thin watery pus, and was often known as "good and laudible pus" (pus bonum et laudable). He noticed that the mobile (buffy coat) element of blood may retard the "spoilage" of blood431; we now would acknowledge these effects as reflecting the antibacterial properties of leukocytes. In these traditional studies, Hunter observed that when blood was allowed to stand, a "buff colored" layer was visible on high of the purple cells. He noted that blood from sufferers with infected wounds had a thicker "buff coloured inflammatory crust" than noticed in blood from healthy topics, which we now perceive displays the neutrophilia related to an infection. With time, he famous that blood would "spoil," as decided by the development of an odor typical of spoiled meals. Hunter discovered that the addition of the "buff coloured inflammatory crust" to a blood sample would delay the time to "spoilage," now understood to replicate the antibacterial abilities of neutrophils. The response to an infection by neutrophils in the microvasculature was elegantly described in An American Text-Book of Surgery in 1892. At one time, the inflammatory cells at sites of infection were thought to be brought on by proliferation of connective tissue cells. After the observations of von Recklinghausen that many of these cells have been able to locomotion (and called "amoeboid cells from their resemblance to the amoeba"), and the work of Addison, who advised that leukocytes in blood may extravasate to tissues,429,432 Cohnheim recognized the cells in the inflamed tissue as leukocytes. The purple blood corpuscles occupy the axis of the blood vessel, and the few white corpuscles which are seen float in the extra sluggish stream of plasma which occupies the borders of the lumen and seems as a clear layer". Induction of irritation by the application of a caustic agent results in hyperemia. Diagram of dilation of the vessels in irritation: a, artery; b, vein; c, capillary. Diagram of stasis of blood and diapedesis of white corpuscles in inflammation: a, artery; b, vein; c, capillary. The capillaries are now fairly distinctly seen, and are crowded with blood corpuscles". This is followed by a slowing of the current, which quickly becomes rather more sluggish than in the regular state. As a result of this diminution of pace the column of blood corpuscles becomes broader and almost completely fills the inside of the vessels. In the veins a fantastic accumulation of white corpuscles takes place on the interior of the partitions. The white corpuscles additionally accumulate in the capillaries, but to not the identical extent. Beginning concurrently with the slowing of the blood stream, is the emigration of the leukocytes from the inside of the veins. Many leukocytes, by a change of shape, send out little prolongations of protoplasm into the substance of the wall, and slight protuberances are soon seen projecting from its outer floor. The portions inside the vessel soon observe these without, and the leukocytes escape from all contact with the vessel. Migration takes place to a restricted extent also from the capillary vessels, however no such course of is observed in the walls of the arteries. These similar actions of neutrophils, in addition to the formation of neutrophil-neutrophil aggregates with infections in rabbit ear veins, were videotaped by W. Diagram of levels of the migration of a single white blood corpuscle by way of the wall of a vein in 1 hour and 50 minutes (mesentery of the frog). Metchnikoff advanced the speculation known as phagocytosis, Here according to this theory, the cells of the infected part, by virtue of their capacity to eat overseas substances, assault and destroy the invading bacteria. The leukocytes are called micro-phagocytes (or microphages), and the bigger cells developed from the mounted connective tissue cells are known as the macro-phagocytes (or macrophages). The interaction of bacteria with blood parts, especially antibodies and the complement system, results in the formation of assorted chemotactic factors. In some cases, the bacteria instantly launch elements that are chemotactic for neutrophils. The interplay of bacteria or their products with other host cells may also result within the formation of chemotactic factors. Neutrophils express particular receptors on their cell surface for quite lots of chemotactic elements. The initial activation of the neutrophil occurs when soluble chemotactic elements bind their receptors on the neutrophil floor. As with the interplay of antibodies and haptens, the affiliation kinetics for these receptor�ligand interactions are very rapid. Typically, enough receptor�ligand interaction to initiate neutrophil activation happens inside seconds. Signaling Many chemotactic issue receptors seem to be coupled to guanine nucleotide-binding proteins (G proteins).
Cheap precose 50mg otcTheir consensus sequence Modules of the C1 the primary enzymatic exercise of the C cascade is assembled from 5 elements, one C1q, two C1r, and two C1s. The C1r�C1s tetramer, in isolation, is a linear construction, with the C-terminal domains responsible for the catalytic perform and the N-terminal domain involved within the Ca2+-dependent protein interactions. In the linear form, the 2 C1r catalytic domains are in the middle, whereas those of the C1s are at the two ends. In the meeting of the C1 esterase, which is the first enzymatic activity of the classical complement cascade, the linear tetramer assumes a compact figure-eight conformation. This binding generates transient conformational adjustments, which activate C1r by disrupting the C1r homodimer. C1s is a extremely particular enzyme, but, throughout the mechanical constraints that are imposed by the superstructure of the entire meeting, it requires some degree of freedom of mobility for its interaction with the substrate. The C1 esterase is a complex that consists of 1 C1q molecule (recognition component) and a tetramer of two C1r and two C1s. It weaves among the many arms of the C1q in a necklacelike means and assumes a figure eight. This association permits access of the catalytic domain of the C1 in the zymogen kind to keep in touch with the lively catalytic area of C1r for C1s to be activated. The flexibility of the tetramer permits changes of their relative position, in order that the energetic C1s websites have entry to C4 and C2 for his or her cleavage and formation of the C4a�C2b C3 convertase. Step three: C3b�C4b�C2a Complex: C5 Convertase the C3 element of complement is essentially the most abundant within the serum (1. The prevailing hypothesis is that a gene that was common for all three elements, C3, C4, and C5, originated from an ancestral a2-macroglobulin gene. Subsequent duplication shaped the C4 and C3�C5 genes, and a second duplication formed separate C3 and C5 genes. It is synthesized as a single protein and is modified post-translationally by a furinlike enzyme, which removes a sequence of 4 arginines. The C3b consists of the remaining a chain, which is linked by the disulfide bond to the intact b chain. Cleavage of the a chain of C3 by the C3 convertase exposes the thioester bond, which, within the intact molecule, is nicely protected inside a pocket in the a series, with a half-life of 231 hours. In the metastable C3b fragment, the bond is uncovered, with a half-life of 60 microseconds. These variations strikingly specific the extraordinary reactivity of the thioester bond for sure groups on the cell surfaces. However, the collectins are C-type lectins and bind carbohydrates, whereas the heads of C1q recognize protein patterns on immune complexes. The time period C1qR has been used loosely, generally with out exhausting proof that the receptor triggers cell signaling that leads to some mobile functions. It has been discovered that calreticulin binds C1q and subsequently qualifies as cC1qR, however the significance of this interplay remains elusive. Step 2: C4 and C2 Complex: C3 Convertase C3 convertase is fashioned by the interaction of two fragments from the C4 and C2 parts of complement. Complement component four circulates in the blood as a disulfide-linked heterotrimer that consists of a (93 kDa), b (75 kDa), and g chains (33 kDa). The C3 and C4 parts share an inside thioester bond, which is shaped between a cysteine and a glutamine, which are two residues aside. C1s activates C4 by splitting the a chain, releasing the C4a fragment from the N-terminal finish of the chain. Loops that join the b strands protrude from the module and may perform as the ligandbinding websites. By electron microscopy, the C2a fragment appears as a two-lobed construction that hyperlinks the C4b and C3b fragments within the final C5 convertase (see the next discussion). The C4b�C2a complex is a Ser esterase with an esterolytic activity and with the C3 because the natural substrate. C3b is deposited on and across the C4b�C2a complicated, binding by way of the thioester bond. The deposition produces an enzyme with a change in the specificity from C3 to C5, generating the C5 convertase. The C3b�C4b and C3b�C3b form high-affinity binding sites for C5 and doubtless, the function of those dimers is to maintain the substrate in a inflexible position for efficient cleavage of C5. It additionally appears that the C3b�C3b�IgG complexes function as higher precursors of convertases than monomeric C3b. C3 is fragmented by several enzymes that generate quite a lot of functionally energetic fragments. The activation of C3 by the C3 convertase cleaves the peptide bond between residues 726 and 727 (Arg-Ser) and generates a small C3a (9 kDa) and a big C3b (176 kDa) fragment. C3b consists of the remaining a chain (a) and the entire b chain, that are linked by the disulfide bond. A second cleavage by factor I separates a small fragment C3f (2 kDa) from the a series and yields another inactivated C3b or iC3b2. Activation of the choice pathway involves three parts: C3, B issue, and D factor. Polysaccharides (zymosan), bacterial merchandise, aggregated human IgA, cobra venom issue, and many other substances are activators of the alternative C cascade. The enzyme that cleaves C3 contains C3b as one of its components, which is the product of a earlier C3 cleavage. Normally, the C3 repeatedly generates a low degree of a functionally C3b-like type by a "tick-over" mechanism. By electron microscopy, it appears as a three-lobed construction, presumably with each module similar to one of many lobes. The C3 part not solely contributes to the classical pathway in the formation of the C5 convertase, it also, as a end result of fragmentation, supplies components of its molecule for different necessary capabilities. The single Arg233�Lys234 bond of issue B becomes susceptible to the enzymatic exercise of issue D only when it varieties an Mg2+dependent complex with C3b. It is the only enzyme in blood that is ready to catalyze this response and is due to this fact completely required for alternative-pathway activation. It is a single chain protein (24 kDa) and is structurally just like pancreatic serine proteases. It circulates in blood in a zymogen or profactor form615 converted to the mature enzyme as a end result of conformational modifications. However, this primary step generates a "resting" enzyme because of an inhibitory sequence loop, which prevents its activation. The energetic enzyme conformation is induced after binding to the substrate in a second step.
Purchase precose 25mg without a prescriptionAfter preliminary adherence, neutrophils project microscopically visible pseudopods between or via the endothelial cells and pressure a passage throughout the endothelial layer. Further migration is then delayed by the basement membrane and periendothelial cells, and the neutrophils may move parallel to , but beneath, the endothelium till a passage into the encircling connective tissue is discovered. Labeled blood neutrophils are found in saliva,136 however loss into saliva might reflect subclinical infections, as a result of few if any cells are found in the salivary ducts289; the rate at which granulocytes enter the oral cavity has been correlated with the diploma of gingivitis. No quantitative data in regards to the price of loss via these numerous organs can be found. It has been advised that the lack to speed up neutrophil production above baseline would possibly handicap neonates by limiting their neutrophil supply during a bacterial an infection. Therefore, one would possibly anticipate that newborns, notably those delivered prematurely, can be at vital threat for critical bacterial infection, and many studies reveal a powerful correlation between prematurity and severe bacterial an infection. Newborn infants, notably if premature, show many other deficiencies in antibacterial protection, such as low levels of IgG antibody, complement components, fibronectin, and lymphokine manufacturing,305 but only maturational differences in neutrophil kinetics are discussed right here. Realizing that the neutrophil system of a fetus is underdeveloped and in a state of maturation, a difference in neutrophil pool sizes and kinetics in this group from these in adults may be anticipated. In addition, fast somatic progress in the fetus and new child places added demands, unique to the neonate, on neutrophil production306; cells are wanted not just for ongoing antibacterial protection, but additionally for a rapidly growing body mass. The investigation of neutrophil kinetics throughout fetal and neonatal life in humans has been hampered by lack of applicability of the techniques used for such research in adults. In fetal and neonatal animals, nonetheless, the liver and spleen, in addition to the lengthy bones, may be eliminated, and the neutrophils inside them could be quantified. Such research in rats show that the neutrophil storage pool is considerably smaller in prematurely delivered animals (1. Experiments performed with a variety of organisms326,328�334 reveal depletion of the storage pool and neutropenia before dying. Similarly, in human neonates with lethal bacterial sepsis, neutropenia and depletion of the neutrophil storage pool, as assessed by bone marrow aspiration, are nearly universal findings. In other studies, this delay in launch of marrow neutrophils was fully corrected by prior administration of type-specific antibody directed toward the organism with which the animal was inoculated. In early investigations, Eitzman and Smith, utilizing the Rebuck skin window technique, demonstrated that a preponderance of eosinophils, not neutrophils, was interested in the abraded dermis of neonates. Diminished chemotaxis of twine blood neutrophils was also demonstrated, with reduction to roughly 80% of levels observed with grownup neutrophils. A additional discount in chemotaxis of neutrophils from sick neonates compared to healthy neonates345 and decreased chemotaxis in preterm neonates with bacterial sepsis followed by a return to normal neonatal values (approx. Neutrophil migration has also been investigated in vivo in neonatal and grownup animals. One technique involved surgical implantation of a sterile polyvinyl sponge disc, standardized for physique weight, into rats. At various intervals, the sponges have been eliminated, and neutrophils that had migrated into them had been chemically quantified. Concurrent with sponge removal, the long bones (and the liver and spleen in neonates) had been also removed, and the dimensions of the entire body neutrophil storage pool was determined. In distinction, approximately 60% of the neutrophils released from the marrow in adults migrated to the sponge, indicating extra efficient neutrophil migration in the adult. Another examine discovered that the accumulation of neutrophils within the peritoneal cavity of rats after intraperitoneal inoculation with numerous chemical attractants was impaired in neonates. By measuring the pressure wanted to aspirate neutrophils right into a glass pipet, Miller determined that the neonatal neutrophil was extra inflexible and less deformable than the adult neutrophil, a characteristic that could be detrimental to movement of neutrophils by way of tissues. A deficiency in the redistribution of cell-surface adhesion websites, elements associated to impaired migration, and impairment of neutrophil adhesiveness has additionally been reported351,352 and would impair neutrophil operate in vivo. Response to complement-derived peptides was additionally impaired, as proven in the response of twine blood neutrophils to endotoxin-activated serum. Whether a big distinction exists in leukocyte focus between the sexes or with advancing years has been debated. The suggestion that a characteristic hourly rhythm occurs has not been confirmed,365,366 nor has the occurrence of a digestive leukocytosis been established. Under all these circumstances, however, the leukocyte count tends to stay throughout the normal range (Table 7. Conclusive demonstration of the effects of climate or season on the leukocyte rely is lacking. In the first few days after a topic has arrived at a high altitude, some leukocytosis, accompanied by lymphopenia and eosinopenia, has been noticed, followed rapidly by slight lymphocytosis and eosinophilia. The magnitude of the leukocytosis associated with exercise appears to rely totally on the intensity of the exercise quite than on its duration. Electrically induced convulsions are followed by a discount in eosinophil and lymphocyte number and a rise in neutrophil number, findings according to the effects of adrenal hormone secretion. In the second part, the variety of neutrophils rises again at roughly four hours, though the number of lymphocytes and eosinophils stays at or below preinjection levels379; this section might mirror an adrenal steroid effect and consists of an absolute neutrophilia. After intravenous injection, leukocytosis peaking at 5 to 10 minutes and of whole period of lower than 20 minutes happens and has been shown to be purely shift neutrophilia. Ether anesthesia produces leukocytosis, most likely because of emotional and reflex reactions, in addition to struggling through the stage of excitement. Thus, shortly after receptor�ligand binding, the intracellular calcium quickly rises from a resting level of approximately zero. It seems that the initial rise in intracellular calcium attributable to the release of intracellular calcium shops performs a critical half within the alteration of membrane permeability to allow the inflow of extracellular calcium. To some extent, variations in intracellular calcium transients might direct particular mobile features, in that specific granule release happens at very low (submicromolar) free calcium concentrations, whereas in studies using permeabilized cells, greater (micromolar) ranges of free calcium end in release of both specific and azurophil granules. Tyrosine phosphorylation has been found to play a crucial role in signal transduction from numerous chemotactic issue receptors. Multiple neutrophil proteins are rapidly phosphorylated after activation, including Src family kinases; the Lyn kinase is activated by chemotaxins, growing its capacity to phosphorylate substrates. Knowledge of signal transduction is rapidly advancing, and the reader is referred to the present literature. For example, adenosine inhibits neutrophil aggregation, adhesion, chemotaxis, and superoxide manufacturing. Signaling in neutrophils is complex and could be initiated by many various stimuli that may share downstream signaling pathways. It seems that the glucocorticoid-regulated protein annexin 1 (lipocortin 1) can bind a formyl-peptide receptor, induce calcium transients, and desensitize neutrophils to subsequent stimulation by other brokers. After priming, neutrophils exhibit a more outstanding respiratory burst or secretory response to a given stimulus than would occur if priming had not occurred. Neutrophil priming may be reversible, with the cells still capable of being reprimed. The mechanism of neutrophil priming appears to be the result of a conformational change in p47phox. Some of the known adhesion molecules of neutrophils and endothelial cells are indicated in Table 7. Approximately one half of the circulating neutrophils exist within the so-called marginating pool, a few of which can be seen microscopically to be rolling alongside the endothelial surface, sustaining a free intermittent contact with endothelial cells.
Order precose with a mastercardSynthetic vitamin K3 (menadione) has no intrinsic exercise till it undergoes in vivo transformation to the active menaquinone form. These K vitamins are 2-methyl-1,4-naphthoquinones with repeating fivecarbon prenyl models at place 3. In vivo, vitamin K is recycled in a microsomal oxidation-reduction system for continued use in the g-carboxylation reaction. To carry out the g-carboxylation reaction, vitamin K has to be present in its lowered hydroquinone kind. One essential goal for anticoagulant therapy is the process required for the regeneration of decreased hydroquinone vitamin K. Anticoagulants that successfully block this response embody warfarin (Coumadin), dicumarol, and phenprocoumon. These oral anticoagulants are structurally just like the quinone form of vitamin K, thereby concentrating on the reductase enzyme and inhibiting the discount to the requisite hydroquinone type. The affinity of the anticoagulants for the reductase enzymes determines the efficacy of the drug. It acts as a aggressive inhibitor of oxidized vitamin K and interferes with its discount. Without the regeneration of the decreased form of vitamin K, the vitamin K�dependent protein carboxylase is unable to convert glutamate to g-carboxy glutamate. Thus, these drugs indirectly have an effect on carboxylation and could be overcome with excess vitamin K. The degree of aggressive inhibition achieved in Coumadin remedy among people taking the identical dose regimen is variable. Factors affecting the efficacy of therapy embody liver operate in the synthesis of the clotting components, enhancement of effect from different drugs, and dietary intake/ adsorption of vitamin K. The hydrophobic sign peptide (prepeptide) gets the protein to the endoplasmic reticulum, the first compartment in the secretory pathway. For the vitamin K�dependent proteins to become mature, the polypeptide is translocated out of the primary compartment within the endoplasmic reticulum throughout the lipid bilayer into the lumen of the endoplasmic reticulum. The propeptide, which plays a role in docking vitamin K�dependent carboxylase,339 is eliminated by an endoproteinase. Removal of an internal di- or tripeptide in singlechain issue X and protein C occurs, which converts them to their mature two-chain zymogen form. Several studies describe the endoproteinase that cleaves the propeptide and the inner bonds as furin/paired fundamental amino acid cleaving enzyme. This enzyme is positioned within the tough endoplasmic reticulum and requires the lowered type of vitamin K, oxygen, and carbon dioxide. It is that this Gla region that mediates the Ca2+-dependent binding of the protein to anionic phospholipid surfaces, thereby making certain close proximity and interplay with different components of the coagulation sequence and with cell receptors for vitamin K�dependent ligands. A: Schematic illustration of the synthesis and posttranslational carboxylation pathway of vitamin K�dependent proteins in the endoplasmic reticulum. The regeneration of vitamin K hydroquinone by the vitamin K�dependent reductases is inhibited by anticoagulants, as illustrated by Coumadin. The importance of every of the domains has been uncovered by way of research from pure variants that occur in patients with both familial bleeding. Defects have diverse causes, together with mutations that result in amino acid substitutions in one or more domains, defects in posttranslational modifications, or mutations that introduce cease codons leading to either no expression or expression of truncated proteins. In the case of mixed vitamin K deficiency, a rare hereditary bleeding disorder,365,366 two studies have recognized a missense mutation within the g-carboxylase gene that ends in a defective g-glutamyl carboxylase and thus incomplete processing of the vitamin K� dependent proteins. Single amino acid substitutions may be introduced into domains or complete domains removed to decide where the intra- and interprotein interactions take place. Structural information by way of nuclear magnetic resonance spectroscopy and x-ray crystallography supplies amino acid assignments and tertiary structure, thus allowing for exact approaches to site-directed mutagenesis research. The mixture of all these strategies ends in a map Glycosylation the addition of a carbohydrate moiety as a posttranslational modification to proteins is referred to as glycosylation. The vitamin K�dependent proteins comprise vital amounts of carbohydrate (Tables 18. However, differences within the properties of the carbohydrate variants of protein C have been famous. The Gla domain is involved within the Ca2+ ion-dependent binding of vitamin K�dependent proteins to anionic phospholipid membranes. Chapter 18 Blood Coagulation and Fibrinolysis of how the domains are aligned and interact. Further, utilizing computational molecular dynamics, one can predict conformational changes associated with protein�protein, protein�ligand, and protein�surface interactions. Identifying residues instantly concerned in binding to membranes, metal ions, or small substrates can lead to new drug therapies. In the absence of calcium, solely the connector peptide and the kringle may be visualized within the ensuing x-ray crystal evaluation. It is most likely going that organization of the polypeptide chains of the Gla area is analogous for all vitamin K�dependent proteins. To date, a number of other vitamin K�dependent protein structures have been elucidated372,373,374,375�382 (see Table 18. Many research on the person vitamin K�dependent proteins have been carried out and are detailed underneath each protein subsection. The negative cost elicited from the string of Gla residues (9 to 13) contributes to the binding to Ca2+ and the era of the conformation required for binding to anionic phospholipid membranes. Chapter 18 Blood Coagulation and Fibrinolysis phospholipids would even be very related. One entails the bridging of calcium between specific Gla residues and the unfavorable anionic phospholipid membrane parts. X-ray crystallographic370,394�396 and nuclear magnetic resonance studies397 have been carried out to elucidate the conformational modifications, within the absence and presence of calcium, that occur on Gla area binding to a lipid membrane. In the absence of calcium, the negatively charged Gla residues seem exposed to the answer, and the hydrophobic residues of the Gla domain are buried in its inside. The hydrophobic patch in prothrombin fragment 1 surrounding the primary pair of Gla residues was decided to be Phe4, Leu5, and Val8. Site-directed mutagenesis studies of protein C determined these residues (Phe4, Leu5, and Leu8) to be necessary in membrane interactions. These enzymes are serine proteases in the same family as trypsin and chymotrypsin. The mechanism of proteolysis by chymotrypsin entails a catalytic triad, composed of Asp102, His57, and Ser195 (chymotrypsin numbering). The nucleophilic attack is carried out by the hydroxyl group of Ser195 with the imidazole ring of His57 taking on the liberated proton and the carboxylate ion of Asp102 stabilizing the growing charge. The serine protease domains of all the Gla-containing components show a excessive diploma of sequence identification with each other and to trypsin and chymotrypsin, cleaving nearly specifically at arginyl residues. However, unlike trypsin, which exhibits little specificity beyond the requirement for arginyl or lysyl residues at the cleavage website, the activated coagulation factors have prolonged substrate specificity pockets where only a small variety of amino acid sequences are recognized by each activated factor. Proteins containing these domains are concerned in blood coagulation, fibrinolysis, complement activation, and microfibril formation in connective tissue and in signal transduction.
Order precose 25 mgThe primary position of ferritin is cellular safety against oxidative damage that may be attributable to highly reactive free iron. The placenta also accepts iron from transferrin and will accomplish that even at comparatively low plasma iron levels, thus successfully competing with the maternal erythroid bone marrow. The export of iron from placental trophoblast into fetal circulation happens by way of ferroportin, and this step is controlled by fetal hepcidin. Although H and L chains make up the abundant cytoplasmic ferritin molecules, a unique ferritin protein is present in mitochondria, and is encoded by a distinct intronless gene. Ferritin can additionally be found in plasma in small quantities (12 to 300 mg/L), and within the absence of inflammation,143 the circulating ferritin concentration correlates roughly with the quantity of iron in shops. Plasma ferritin appears to be actively secreted into plasma, primarily by macrophages144,145 and is iron-poor in comparability with tissue ferritin. Hemosiderin was formerly distinguished from ferritin on the basis of solubility and the Perls Prussian blue reaction. It differs from ferritin in having a higher iron-to-protein ratio in addition to being less soluble in aqueous options. Standard hemosiderin preparations could comprise a wide selection of organic constituents, including proteins, lipids, sialic acid, and porphyrins. Hemosiderin appears to represent a more secure and less out there type of storage iron than ferritin. Newly deposited or newly mobilized iron enters or leaves the ferritin compartment. Only after extended storage or continued mobilization does the hemosiderin compartment change in measurement. Iron deficiency anemia, hemochromatosis, and the anemia of persistent disease/inflammation are each examples of this principle. Third, survival of erythroid precursors and erythrocytes is reduced, significantly when the anemia is extreme. When transferrin saturation falls under 15%, the provision of iron to the marrow is insufficient to meet basal necessities for hemoglobin manufacturing (generally 25 mg of iron day by day in average adults). As a outcome, the amount of free erythrocyte protoporphyrin increases, reflecting the excess of protoporphyrin over iron in heme synthesis. If globin synthesis was not decreased in heme deficiency, misfolding and precipitation of excess globin chains would result in apoptosis. Globin synthesis is managed by heme availability at both the transcriptional and translational levels. Heme regulates globin gene expression by its capability to bind a transcription suppressor Bach1. When heme is deficient, Bach1 associates with small Maf proteins (sMafs) and causes transcriptional repression of globin genes. In Hri-/- mice, the adaptive hypochromic and microcytic response to iron deficiency was absent. Aside from erythroid precursors and tumor cells, iron uptake by hepatic parenchymal cells has been most extensively studied. Normally, approximately 5% of iron leaving plasma is accounted for by this pathway. Cellular proliferation is also restricted in iron deficiency, and red blood cell numbers fall. Their iron is reused throughout the bone marrow, making the interpretation of ferrokinetic studies more sophisticated. There is a robust correlation between the diploma to which pink cell survival is shortened and the proportion of morphologically irregular cells on blood smear. It is typically recommended that many of the enzymes are depleted in proportion to the degree of anemia. In iron-deficient rats, impaired exercise performance correlated with decreased ranges of a-glycerophosphate oxidase in muscle. Several forms of genetic iron deficiency anemia are related to hypochromic microcytic anemia and iron overload outdoors of the erythron. These are attributable to autosomal recessive mutations in a number of genes and are exceedingly uncommon. Deficiency of one other major plasma protein, ceruloplasmin, also causes mild iron deficiency anemia associated with iron accumulation in the liver and brain. Further studies might be needed to evaluate the chance that much less extreme or heterozygous mutations enhance susceptibility to frequent, acquired iron deficiency anemia. As the total body iron stage begins to fall, a attribute sequence of occasions ensues. First, the iron stores within the hepatocytes and the macrophages of the liver, spleen, and bone marrow are depleted. Once shops are gone, plasma iron content decreases, and the provision of iron to marrow turns into inadequate for regular hemoglobin production. Consequently, the quantity of free erythrocyte protoporphyrin increases, manufacturing of microcytic erythrocytes begins, and the blood hemoglobin level decreases, finally reaching abnormal ranges. The first stage, additionally called prelatent iron deficiency or iron depletion, represents a reduction in iron shops with out decreased serum iron ranges. Finally, in the third stage, the blood hemoglobin focus falls under the lower limit of regular, and iron deficiency anemia is clear. Iron-containing enzymes, such because the cytochromes, also reach abnormally low levels throughout this period. Clinical manifestations include a constellation of constitutional signs: fatigue, decreased exercise tolerance with tachycardia, dermatologic manifestations, decreased mental efficiency, dysphagia, despair, and stressed legs syndrome. It has been confirmed by experiments by which normal volunteers have been steadily depleted of iron by phlebotomy. Inasmuch as serum ferritin is an acute phase reactant regulated by irritation, these information might underestimate the prevalence of anemia in some populations, particularly the elderly. Recent analyses have estimated prevalence of iron deficiency anemia within the aged (>65 years of age) and extreme elderly (>75 years of age) ranging from 10% to up to 36%. Iron deficiency was detected in 9% of infants and toddlers, with anemia in approximately one third of those kids. The prevalence of iron deficiency was also greater among folks residing in continual poverty. If an iron-deficient youngster is identified, the mother and siblings of that child are regularly additionally deficient. The regular mechanisms for maintaining iron stability were mentioned earlier on this chapter. Factors leading to adverse iron steadiness, elevated necessities, or insufficient iron for erythropoiesis are listed in Table 23. The association of a marginal diet with some source of blood loss, similar to that associated with menstruation, is a typical combination. Another instance is hookworm infestation, which produces anemia primarily in these individuals whose diets are marginally sufficient. Diet the entire quantity of iron within the diet roughly correlates with caloric content material; in the United States, the average food plan contains 6 mg of iron per 1,000 kcal.
References - Varela-Duran J, Urdiales-Viedma M, Taboada-Blanco F, et al: Neurofibroma of the ureter, J Urol 138(6):1425n1426, 1987.
- Tsuda M, Davis IJ, Argani P, et al: TFE3 fusions activate MET signaling by transcriptional up-regulation, defining another class of tumors as candidates for therapeutic MET inhibition, Cancer Res 67:919n929, 2007.
- Rioja J, Rodriguez-Fraile M, Lima-Favaretto R, et al: Role of positron emission tomography in urological oncology, BJU Int 106:1578-1593, 2010.
- Cody JD, Jacobs ML, Richardson K, et al: Oestrogen therapy for urinary incontinence in post-menopausal women (Review), Cochrane Database Syst Rev (10):CD001405, 2012.
- Michel MC, Vrydag W: Alpha1-, alpha2- and beta-adrenoceptors in the urinary bladder, urethra and prostate, Br J Pharmacol 147(Suppl 2):S88nS119, 2006.
|
|