"Order altace australia, hypertension 1."By: Dawn Sowards Brezina, MD - Assistant Professor of Medicine
 https://medicine.duke.edu/faculty/dawn-sowards-brezina-md
Generic altace 5 mg on lineChronic temporal lobe epilepsy is associated with severely declined dentate neurogenesis within the adult hippocampus. Differential upregulation of extracellular matrix molecules associated with the looks of granule cell dispersion and mossy fiber sprouting during epileptogenesis in a murine mannequin of temporal lobe epilepsy. Chronic temporal lobe epilepsy: a neurodevelopmental or progressively dementing disease Neuropathological spectrum of cortical dysplasia in youngsters with severe focal epilepsies. Seizures within the growing brain: cellular and molecular mechanisms of neuronal injury, neurogenesis and cellular reorganization. Histological heterogeneity of dysembryoplastic neuroepithelial tumour: identification and differential diagnosis in a sequence of seventy four cases. Granule cell dispersion within the dentate gyrus of humans with temporal lobe epilepsy. Kalachikov S, Evgrafov O, Ross B, Winawer M, Barker-Cummings C, Martinelli Boneschi F, et al. Disruption of the serine/threonine kinase 9 gene causes extreme X-linked infantile spasms and psychological retardation. Common genetic variation and susceptibility to partial epilepsies: a genome-wide association research. Alterations of the microvascular community in sclerotic hippocampi from patients with epilepsy. Voxel-based morphometry of temporal lobe epilepsy: an introduction and review of the literature. Damage to the amygdalo-hippocampal projection in temporal lobe epilepsy: a tracttracing research in chronic epileptic rats. Cerebral cortical dysplasia: giant neurons present potential for increased excitation and axonal plasticity. The hypothalamic hamartoma: a mannequin of subcortical epileptogenesis and encephalopathy. Predictors of surgical consequence and pathologic concerns in focal cortical dysplasia. Clinical features and pathological traits of amygdala enlargement in mesial temporal lobe epilepsy. Hippocampal atrophy and T2-weighted signal adjustments in familial mesial temporal lobe epilepsy. Developmental historical past of the subplate zone, subplate neurons and interstitial white matter neurons: relevance for schizophrenia. Prolonged seizure activity impairs mitochondrial bioenergetics and induces cell demise. Low-grade focal cortical dysplasia is related to prenatal and perinatal mind harm. Incomplete resection of focal cortical dysplasia is the principle predictor of poor postsurgical end result. Different features of histopathological subtypes of pediatric focal cortical dysplasia. The epilepsy, the protease inhibitor and the dodecamer: progressive myoclonus epilepsy, cystatin b and a 12-mer repeat enlargement. Vesicular zinc regulates the Ca2+ sensitivity of a subpopulation of presynaptic vesicles at hippocampal mossy fiber terminals. Is there a critical period for mossy fiber sprouting in a mouse mannequin of temporal lobe epilepsy A meta-analysis of voxel-based morphometry studies on unilateral refractory temporal lobe epilepsy. Spatiotemporal profile of N-cadherin expression within the mossy fiber sprouting and synaptic plasticity following seizures. To die or to not die for neurons in ischemia, traumatic brain injury and epilepsy: a evaluate on the stress-activated signaling pathways and apoptotic pathways. Prevention or modification of epileptogenesis after brain insults: experimental approaches and translational analysis. Granule cell dispersion is correlated with early epileptic occasions in human temporal lobe epilepsy. Ontogeny of Lafora bodies and neurocytoskeleton modifications in Laforin-deficient mice. Triple pathology in epilepsy: coexistence of cavernous angiomas and cortical dysplasias with other lesions. Sprouting in human temporal lobe epilepsy: excitatory pathways and axons of interneurons. Loss of Calbindin-D28K immunoreactivity from dentate granule cells in human temporal lobe epilepsy. Changes within the distribution and connectivity of interneurons in the epileptic human dentate gyrus. Cytoarchitectural alterations are widespread in cerebral cortex in tuberous sclerosis complicated. Neuronal bursting properties in focal and parafocal areas in pediatric neocortical epilepsy stratified by histology. A medical, electroencephalographic and neuropathological examine of the brain in epilepsy, with particular reference to the temporal lobes. Shaken infant syndrome: developmental neuropathology, progressive cortical dysplasia, and epilepsy. Toll-like receptor 4 and high-mobility group box-1 are concerned in ictogenesis and could be focused to cut back seizures. Calbindin D28K expression in relation to granule cell dispersion, mossy fibre sprouting and memory impairment in hippocampal sclerosis: A surgical and post mortem collection. Somatic translocation: a novel mechanism of granule cell dendritic dysmorphogenesis and dispersion. Infiltration of T lymphocytes and expression of icam-1 in the hippocampus of patients with hippocampal sclerosis. Electrophysiologic modifications within the lateral and basal amygdaloid nuclei in temporal lobe epilepsy: an in vitro research in epileptic rats. Is mossy fiber sprouting present on the time of the first spontaneous seizures in rat experimental temporal lobe epilepsy Neuropeptide Y gene remedy decreases continual spontaneous seizures in a rat mannequin of temporal lobe epilepsy. Classic hippocampal sclerosis and hippocampal-onset epilepsy produced by a single "cryptic" episode of focal hippocampal excitation in awake rats. Cerebral hemiatrophy related to hippocampal sclerosis following a single extended febrile seizure.
Order 2.5 mg altace with amexNevertheless, certain immunohistochemical staining patterns may be helpful to distinguish oligodendrogliomas from most other mind tumour entities. However, some oligodendrogliomas, together with cases with combined losses of 1p and 19q, comprise tumour cells with morphological options indicative of neuronal/neurocytic differentiation and immunohistochemical positivity for synaptophysin and other neuronal markers. In basic, the imply fraction of constructive tumour cells is Oligodendroglioma 1677 considerably higher in anaplastic oligodendrogliomas as compared to low-grade oligodendrogliomas. Cytological preparations from tissue smears most readily permit the identification of macrophages with their vacuolated cytoplasm and accompanying reactive astrocytes. These cells often lie clustered around blood vessels in association with lymphocytes, but perivascular macrophages may also be current in otherwise typical oligodendrogliomas. Partial lobectomy specimens carried out for intractable seizures not sometimes have seemingly elevated numbers of oligodendrocytes. In such instances, nonetheless, the white matter is condensed with resultant crowding of oligodendroglial nuclei, whereas the accompanying astrogliosis additional contributes to the elevated cellularity. Similar histological features may be seen adjoining to arteriovenous malformations. Smear preparations also assist to distinguish well-differentiated oligodendroglioma from gliosis, in that standard oligodendrocytes possess little discernible cytoplasm and no nuclear lobation, and reactive astrocytes typically have extra open chromatin, ample cytoplasm, and symmetrically radiating tapered processes. With respect to the differential prognosis of neoplasms, the distinction of oligodendroglioma from astrocytomas, specifically diffuse and pilocytic subtypes, bears necessary scientific implications (Box 28. For instance, a central pathology evaluate of of low-grade oligodendrogliomas submitted for 1p deletion testing may affirm this analysis in solely half of the cases. In the absence of the everyday perinuclear clearing, the distinction of oligodendroglioma from diffuse astrocytoma is largely primarily based on the roundness and uniformity of nuclei. In addition, infiltration into the cortex and formation of secondary constructions is more typical of oligodendrogliomas, however not particular. In most situations, however, at least focally traditional pilocytic options are current. Tumours are usually composed of small, round tumour cells displaying a paucity of cytoplasmic intermediate glial filaments, which are in any other case frequent in regular and neoplastic astrocytes. Gliofibrillary oligodendrocytes and minigemistocytes comprise cytoplasmic skeins or whorls of intermediate filaments, in distinction to the notably random distribution of quick intermediate filaments within the gemistocytic astrocytoma tumour cells. In comparison with other gliomas, cytoplasm is sparse and processes are probably to be brief and tapered. Variable numbers of randomly organized microtubules could additionally be noticed, and there could additionally be moderate amounts of endoplasmic reticulum, moderately to well-developed Golgi complicated, and variable numbers of mitochondria. Signet-ring cells in oligodendroglioma have their cytoplasm crammed with degenerating mitochondria and irregularly and widely dilated cisternae of tough endoplasmic reticulum containing granular materials. Diagnostic overview the histopathological differential prognosis of oligodendroglioma involves the popularity of both reactive and neoplastic lesions. Concerning reactive lesions, oligodendrogliomas need to be distinguished from macrophage-rich processes similar to demyelinating diseases or cerebral infarcts. It can also be important to know if a biopsy comes from the temporal lobe as a end result of regular perineuronal oligodendrocytes may be numerous there and should mimic neoplastic perineuronal satellitosis. Freezing artefacts that cause loss of detail in chromatin construction, chromatin hyperchromasia and nuclear irregularity are problematic in low-grade oligodendrogliomas by eliminating salient nuclear features. Ependymomas, notably these of the clear cell kind, may be mistaken for oligodendroglioma. The highly attribute, complicated nodules vary significantly in morphology, a minority being composed of astrocytic cells with pilocytic or different gliomatous features. The finding of perinuclear halos, arborizing vasculature and never infrequent calcification in both tumours contributes to the possible confusion. This distinctive location mixed with neurocytic rosettes, immunohistochemical reactivity for synaptophysin, lack of diffuse immunoreactivity for S�100 protein, and the characteristic neuronal ultrastructural options provide the definitive diagnosis. Nevertheless, neurocytic tumours also come up exterior the ventricular system, including the cerebral hemispheres. The differences in cellularity and mitotic activity, and the immunohistochemistry for neurofilaments and synaptophysin are options that distinguish them from oligodendrogliomas. Distinguishing factors are just like those of neurocytoma, with the additional feature of lipidized cells that resemble adipocytes, and the preferential cerebellar location. Clear cell meningiomas hardly ever enter the differential analysis, but must be thought of in the setting of a primarily leptomeningeal oligodendroglioma. The immunocytochemical profile of oligodendroglioma cells is more reminiscent of immature glial cells than mature oligodendroglia. Furthermore, the discovering that oligodendroglioma cells may often specific markers of other lineages, including astrocytic and neuronal antigens, would possibly favour the hypothesis of an origin from neural stem or progenitor cells somewhat than mature oligodendrocytes. Diagnostically, the demonstration of 1p/19q deletion may serve to verify the analysis of oligodendroglioma versus other clear cell tumours. In explicit, paediatric oligodendrogliomas usually lack these deletions however may represent a distinct entity. Note two green signals from probes to the lengthy arm of chromosome 1 (1q), but only a single purple signal from the probe to the short arm of chromosome 1(1p). In truth, low-grade gliomas are troublesome to study because they rarely present dramatic radiological responses to remedy and require long follow-up times. In rodents, oligodendroglioma can be induced by numerous carcinogens; specifically administration of ethylnitrosourea and methylnitrosourea in rats frequently causes glial tumours with the morphology of oligodendroglioma. Cranial irradiation clearly is a risk factor, as indicated by particular person sufferers who developed oligodendrogliomas after radiation therapy for different tumours. In addition, mixed therapy offered a survival profit in patients alive beyond two years, suggesting a delayed profit for chemotherapy. Because late toxicity is a serious concern for such patients with anticipated longterm survival, radio- and/ or chemotherapy is usually deferred till tumour progression, in particular in young sufferers presenting with seizures Incidence, age and gender distribution Anaplastic oligodendroglioma accounts for about 0. Caucasians are more generally affected than black people, as indicated by incidence rates of 0. The characteristic vascular pattern of branching capillaries is often still recognizable, though extra microvascular proliferation is normally obvious. Occasional tumours present marked cellular pleomorphism including multinucleated big cells. In addition, rare anaplastic oligodendrogliomas could current with a sarcomatous component. Such deletions are significantly frequent in anaplastic oligodendrogliomas without 1p and 19q losses, but can also be current in 1p/19q-deleted cases. Other chromosomal imbalances detected at more than random frequency embrace deletions on 4q, 10q and 18q as nicely as gains on 7, 8q and 19p. Assessment of prognostic and predictive molecular markers in anaplastic glioma patients There are currently three clinically relevant molecular markers that present robust prognostic and/or predictive data past the histological classification of anaplastic oligodendroglial tumours. However, this molecular marker is additionally useful to predict a profit from the addition of alkylating chemotherapy to radiotherapy, i. Thus, testing for 1p/19q deletion could guide remedy choices in sufferers with anaplastic oligodendroglial tumours along with serving as a prognostic marker. Various methods can be found for the testing of these clinically relevant molecular markers within the routine diagnostic setting, every associated with distinct benefits and drawbacks. Moreover, appropriate methods of high quality management have to be established to avoid unacceptable intra- and interlaboratory variability in molecular testing outcomes.
Order altace australiaSeveral studies counsel that oligoastrocytoma follows a clinical course intermediate between that of oligodendroglioma or diffuse astrocytoma. Molecular genetics the molecular genetic modifications noticed in oligoastrocytomas both correspond to these generally present in oligodendrogliomas, i. Molecular analyses of microdissected oligodendroglial and astrocytic areas revealed common genetic alterations in most cases, indicating a monoclonal origin of each components. Incidence, age and sex distribution Data on the incidence of anaplastic oligoastrocytomas are sparse and confounded by the variability within the histological classification of those tumours. In their collection of 987 sufferers with oligodendroglial, mixed or astrocytic tumours, solely eleven (1. Most anaplastic oligoastrocytomas are major tumours that current with a short clinical historical past. However, tumours can also develop by development from pre-existing low-grade tumours. Undefined margins and inhomogeneous T1/T2 alerts had been discovered more generally in anaplastic than low-grade oligoastrocytomas. Microscopy exhibits a diffusely infiltrating oligoastrocytoma with focal or diffuse histologic signs of anaplasia. These embrace excessive cellularity, nuclear atypia, cellular pleomorphism and apparent mitotic activity. However, the identification of necrotic areas signifies progression towards glioblastoma with oligodendroglial part. Most generally, the astrocytic and oligodendroglial parts each show anaplastic features. In some cases, nonetheless, anaplasia could additionally be focal and restricted to both component. This distinction was initially primarily based on a retrospective analysis of a giant collection of malignant glioma patients that exposed considerably shorter survival of patients with anaplastic oligoastrocytomas containing areas of necrosis. Biological Behaviour and Prognosis Anaplastic oligoastrocytomas are quickly rising malignant tumours that are inclined to recur after therapy, which normally consists of a multimodal routine involving resection, radiotherapy and/or chemotherapy. In sufferers not stratified based on the 1p/19q genotype, median total survival of 2. Among these, the distinction from anaplastic astrocytoma poses no problem when a definite oligodendroglioma component is recognized. The identification of an oligodendroglial element is prognostically necessary, as indicated by the study of Donahue et al. The differential analysis would come with different entities that will reveal both a fibrillar matrix and variably angiocentric features, corresponding to subependymoma, tanycytic ependymoma, astroblastoma, pilomyxoid astrocytoma and angiocentric glioma. Outcome of second malignancies after retinoblastoma: a retrospective analysis of 25 patients treated on the Institut Curie. Multiparametric characterization of grade 2 glioma subtypes utilizing magnetic resonance spectroscopic, perfusion and diffusion imaging. Distinct expression pattern of microtubule-associated protein�2 in human oligodendrogliomas and glial precursor cells. Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas. The characteristics of astrocytomas and oligodendrogliomas are attributable to two distinct and interchangeable signaling codecs. Prognostic implication of histopathological, immunohistochemical and clinical features of oligodendrogliomas: a examine of 89 cases. Platelet-derived progress factor and its receptor expression in human oligodendrogliomas. Influence of an oligodendroglial element on the survival of patients with anaplastic astrocytomas: a report of Radiation Therapy Oncology Group 83�02. Anaplastic oligodendrogliomas with 1p19q codeletion have a proneural gene expression profile. Internexin in the prognosis of oligodendroglial tumors and association with 1p/19q status. Genetic differences between neurocytoma and dysembryoplastic neuroepithelial tumour and oligodendroglial tumours. Value and limits of immunohistochemistry in differential diagnosis of clear cell major brain tumours. Shared allelic losses on chromosomes 1p and 19q counsel a common origin of oligodendroglioma and oligoastrocytoma. Panel review of anaplastic oligodendroglioma from European Organization for Research and Treatment of Cancer Trial 26951: evaluation of consensus in analysis, influence of 1p/19q loss, and correlations with outcome. Signet-ring cell oligodendroglioma � report of two circumstances and discussion of the differential diagnosis. Genetic signature of oligoastrocytomas correlates with tumour location and denotes distinct molecular subsets. Immunohistochemical characterization of oligodendrogliomas: an evaluation of a quantity of markers. Identification of a CpG island methylator phenotype that defines a distinct subgroup of glioma. Population-based studies on incidence, survival charges and genetic alterations in astrocytic and oligodendroglial gliomas. Oligodendroglial neoplasms with ganglioglioma-like maturation: a diagnostic pitfall. Oligodendrogliomas: reproducibility and prognostic worth of histologic analysis and grading. Expression of the genes encoding myelin fundamental protein and proteolipid protein in human malignant gliomas. Temozolomide as initial therapy for adults with low-grade oligodendrogliomas or oligoastrocytomas and correlation with chromosome 1p deletions. A t(1;19)(q10;p10) mediates the mixed deletions of 1p and 19q and predicts a greater prognosis of sufferers with oligodendroglioma. Oligodendroglial tumors with marked desmoplasia: clinicopathologic and molecular options of 7 cases. Prognostic value of Ki67 index in anaplastic oligodendroglial tumours � a translational examine of the European Organization for Research and Treatment of Cancer Brain Tumor Group. Anaplastic oligodendrogliomas: prognostic elements for tumour recurrence and survival. Evaluation of cell proliferation, epidermal growth issue receptor and bcl�2 immunoexpression as prognostic elements for sufferers with World Health Organization grade 2 oligodendroglioma. Disseminated oligodendroglial-like leptomeningeal tumor of childhood: a distinctive clinicopathologic entity. Investigation of human brain tumours for the presence of polyomavirus genome sequences by two independent laboratories.
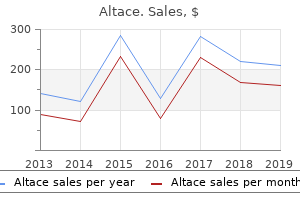
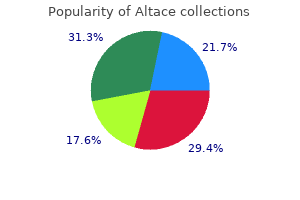
Cheap altace ukIn situ expression of angiopoietins in astrocytomas identifies angiopoietin-2 as an early marker of tumor angiogenesis. Tumor location and development pattern correlate with genetic signature in oligodendroglial neoplasms. Alterations of chromosome arms 1p and 19q as predictors of survival in oligodendrogliomas, astrocytomas, and mixed oligoastrocytomas. Large effect of age on the survival of patients with glioblastoma handled with radiotherapy and brachytherapy boost. Comparative genomic hybridization indicates two distinct subgroups of pilocytic astrocytomas. Intravascular thrombosis in central nervous system malignancies: a potential function in astrocytoma development to glioblastoma. Incidence, age and intercourse distribution Oligodendroglioma accounts for roughly 2 per cent of all main mind tumours and 6 per cent of all gliomas. For the United States of America, the general annual incidence rate through the years 2004 to 2008 has been estimated as 0. In older research, patient histories were typically long-standing with intervals greater than 5 years between the primary symptom and the final diagnosis being widespread. Some tumours demonstrate heterogeneity because of intratumoural haemorrhages and/or cystic degeneration. Contrast enhancement in low-grade tumours has been linked to much less favourable prognosis. Oligodendrogliomas are densely vascularized tumours and intratumoural haemorrhages are frequent. Occasional mitotic figures are nonetheless appropriate with a lowgrade oligodendroglioma. The typical nuclear options are finest demonstrated in tissue smears and in well-fixed, paraffin-embedded specimens. On smear preparations, oligodendroglioma cells have a small rim of cytoplasm and processes are sparse. There is a notable paucity of fibrillarity in solid areas of oligodendrogliomas, whereas the infiltrative edge incorporates background neuropil. On low-power examination of tissue sections, a striking feature of most oligodendrogliomas is their mobile uniformity. In this regard, the diagnosis of oligodendroglioma must be considered within the setting of any moderately hypercellular glioma with uniform nuclei. This could also be particularly useful in frozen sections, where the presence of a hypercellular glioma with out a lot nuclear pleomorphism, spindled cells or mitoses ought to prompt consideration of oligodendroglioma. However, pathologists must be reluctant to make a particular prognosis of oligodendroglioma based on intraoperative frozen sections alone. The tumour cells are usually arranged in diffuse sheets, usually conspicuously grouped by a branching capillary community. Some tumours include rather distinct nodules that have to be distinguished from those seen in dysembryoplastic neuroepithelial tumours. Extracellular mucin deposition and microcyst formation are distinguished in some circumstances. Macroscopy Oligodendrogliomas could come up wherever within the central nervous system but most develop in the cerebral hemispheres. With lowering frequencies, oligodendrogliomas manifest within the temporal, parietal and occipital lobes. Oligodendrogliomas are far less frequent within the basal ganglia, thalamus, mind stem or cerebellum. Oligodendrogliomas might focally infiltrate adjacent leptomeninges, sometimes with an accompanying desmoplastic reaction resulting in a more firm, rubbery consistency of the superficial element. Rare cases appear as very delicate, gelatinous lots as a outcome of Oligodendroglioma (a) (b) 1675 28 (c) (d) 28. In some tumours, the capillary network subdivides the tumour tissue into smaller and bigger lobules. Probably due to their dense vascularization, oligodendrogliomas tend for intratumoural haemorrhages. Microvascular proliferation and necrosis are absent in low-grade oligodendroglioma. Oligodendrogliomas can also unfold into the leptomeninges and, often, grow primarily as leptomeningeal masses. Minute calcifications are most common alongside or within the delicate vasculature. These embrace nuclear atypia and pleomorphism, excessive cellularity, brisk mitotic activity, endothelial hypertrophy and microvascular proliferation, as nicely as necrosis. Collectively, these morphological options are much like these commonly used for the grading of diffuse astrocytic gliomas. However, their individual impact on grading and their integration into an objective and reproducible grading 1676 Chapter 28 Oligodendroglial Tumours system of oligodendrogliomas is less established. A study by seven impartial neuropathologists recognized older patient age, excessive cellularity, presence of mitoses, endothelial hypertrophy and proliferation, and necrosis considerably related to shorter survival on univariate analysis in a cohort of 124 sufferers. As a rule, the histological analysis of an anaplastic oligodendroglioma ought to require both the presence of conspicuous endothelial proliferation and/or high mitotic activity. Thus, fashionable evaluation of oligodendroglioma behaviour ought to contemplate scientific and neuroimaging findings, histological grading, proliferation indices and molecular genetic characteristics. Immunohistochemistry Immunohistochemical research might present useful information for the classification and grading of oligodendroglial tumours. However, a specific and sensitive immunohistochemical marker of oligodendroglial tumours is still lacking. Vimentin immunopositivity is also more widespread in anaplastic than in low-grade oligodendrogliomas. Occasional anaplastic oligodendrogliomas may superficially resemble metastatic clear cell carcinomas. Unlike the latter, that are stable and sharply demarcated, oligodendrogliomas are infiltrative. By distinction, stains for low molecular weight cytokeratin are unfavorable in oligodendrogliomas and subsequently reliably exclude metastatic carcinoma. In a fraction of anaplastic oligodendrogliomas, the differential diagnosis with anaplastic oligoastrocytoma could additionally be problematic and related to appreciable interobserver variability. Moreover, it is essential to separate anaplastic oligodendrogliomas from malignant small cell astrocytic neoplasms, i. Alternatively, the 1p/19q standing may just characterize a molecular signpost for genetic/ epigenetic alterations on different chromosomes that influence remedy response and survival. In fact, malignant gliomas carrying deletions of just one chromosomal arm or deletions of only elements of those arms usually demonstrate more aggressive conduct, even when compared to 1p/19q-undeleted cases. The prognosis is less beneficial when compared to low-grade oligodendroglioma however significantly higher when in comparison with malignant astrocytic tumours.
Generic 1.25mg altace with visaPutative antibodies directed against the endothelial cells activate the complement cascade resulting in C5b-9, the terminal lytic element of the complement pathway, being deposited early in the disease course. Rhabdomyolysis and myoglobinuria may occur, however that is uncommon in dermatomyositis. There is a well-established affiliation between malignancy and dermatomyositis in adults. In dermatomyositis, involvement of pores and skin vasculature manifests as a heliotrope or violaceous rash, particularly over the eyes and malar regions of the face, and as erythema around the nail beds and over the knees and elbows. In 1606 Chapter 25 Diseases of Skeletal Muscle extreme cases, the entire skin turns into tight, shiny and reddened. Calcium is deposited in the subcutaneous tissue and in the supportive connective tissues within muscle, but not in muscle fibres themselves. Children with dermatomyositis normally have systemic symptoms, corresponding to mood swings, malaise, listlessness and lethargy, which may be the presenting feature or characterize a relapse. Inclusion body myositis is certainly one of the most typical disorders of muscle in sufferers aged over 50 years. Dysphagia, weak point of the wrist, finger flexor muscular tissues and of ankle dorsiflexion are common. They are extremely illness particular, can appear months before the onset of symptoms, correlate with disease activity and disappear on disease remission. Electromyography exhibits a attribute pattern, with a mixture of spontaneous fibrillation potentials, much like those seen in denervation, and polyphasic short-duration potentials on voluntary contraction, as in myopathies. Imaging strategies are having an rising function, and show increased signal in relation to oedema and inflammatory adjustments in subcutaneous fats. Note the sarcolemmal labelling within the case of dermatomyosits and normal labelling of blood vessels in each. Abnormal variation in fibre measurement is usually present, but hypertrophy is absent or much less pronounced than in muscular dystrophies. Other pathological features embrace inner nuclei, basophilic fibres, a rise in connective tissue (usually less than in muscular dystrophies), moth-eaten fibres or fibres with core-like areas, and fibre splitting. There may also be loose oedematous separation of muscle fibres with interspersed fibrous tissue. In dermatomyositis, areas of infarction, characterized by teams of pale-staining necrotic fibres, could also be present. Necrotic fibres may present a peripheral cuff of basophilia, comparable to regeneration, a characteristic hardly ever seen in muscular dystrophies. Acid phosphatase exercise is associated with the presence of inflammatory cells and macrophages and can be increased in the fibres. They occur in the perimysium and endomysium, are sometimes perivascular and should partly invade blood vessel walls. The proportion and distribution of the various inflammatory cell sorts differ in polymyositis and dermatomyositis. B-cells, in distinction, are predominantly perivascular and barely positioned within the endomysium in polymyositis. With electron microscopy, endothelial cells of capillaries and arterioles are seen to comprise tubuloreticular inclusions. Surface deposition of C5b�9 could additionally be seen on a restricted number of fibres and inside necrotic 25. Basal lamina markers similar to Ulex europaeus or laminin 5, are additionally useful because the capillaries are highlighted towards the unfavorable (Ulex) or weak (laminin 5) labelling of the sarcolemma. Perifascicular atrophy and capillary pathology are concentrated near the avascular perimysium. Multiple or single foci of amyloid deposits are present in vacuolated and non-vacuolated fibres, and best observed with Congo red staining considered with fluorescence utilizing an excitation filter suitable for rhodamine or Texas purple. The very uncommon necrotizing myopathy with pipestem capillaries shows distinct thickening of the capillary partitions with complement deposition, and deposition of granular amorphous material in their basement membranes is seen electron microscopically. All reported patients had severe systemic disease corresponding to neoplasia, vasculitis and interstitial lung illness. Muscle biopsies might present fibre necrosis and inflammation, typically with a vasculitis. Non-specific myopathic modifications, such as sort 2 fibre atrophy, are also frequent in connective tissue disorders. Myofibres distant from the infiltrate are typically intact however the alum can reach the brain. Electron microscopy reveals spicules of osmiophilic aluminium oxyhydroxide surrounded by discontinuous lysosomal membranes. The disease may be triggered by exposure to toxins, treatment or trauma, and infections corresponding to borreliosis and Mycoplasma arginine. Fasciitis/Myofasciitis with Panniculitis Fasciitis and panniculitis embody a diverse clinicopathological spectrum of illnesses the place the inflammatory changes are centred on the fascia and subcutaneous fat respectively. A small proportion of people who obtain vaccines containing aluminium oxyhydroxide as an adjuvant current with delayed onset of myalgia, chronic fatigue and cognitive dysfunction, and exhibit very long-term persistence of alum-loaded macrophages at the site of vaccination forming a lesion referred to as macrophagic myofasciitis. There is focal infiltration of the epimysium, perimysium and perifascicular endomysium by circumscribed collections and sheets 25. Granulomatous Myositis, Focal Myositis and Brachiocervical Inflammatory Myopathy Granulomatous myositis is a rare illness characterized by discrete perimysial or endomysial epithelioid granulomas which would possibly be often non-necrotizing, with variable interstitial inflammation and myonecrosis. The affiliation with sarcoidosis is well-known and the prevalence of asymptomatic granulomatous myositis in sarcoid is reported to be as high as 50�80 per cent. The diagnosis of idiopathic/primary/isolated granulomatous myositis is one of exclusion. Focal myositis is a rare entity that presents clinically as a solitary, intramuscular mass lesion and histologically corresponds to an inflammatory pseudotumour, with variable myopathic, focal neurogenic and inflammatory modifications, and fibrosis. The infiltrate is macrophage and T-cell wealthy, with a prominent B-cell and plasmacytoid dendritic cell element present when the lesion is actively infected. Common misdiagnoses embody haematological or soft tissue malignancy, primary or proliferative myositis, myositis ossificans and inflammatory myofibroblastic tumour. Careful attention to the morphology and immunophenotype and the clinical presentation is necessary to avoid these pitfalls. More lately it has been suggested that focal myositis could also be a neurogenic phenomenon. Histology reveals an energetic myopathic course of with focal perimysial and perivascular irritation with prominent B-cells, endomysial dendritic cells and complement C5b-9 staining of the endomysial connective tissue. There is a strong affiliation with systemic autoimmune problems and presence of antinuclear antibodies. Additional proof of vascular injury including haemosiderin deposits, fibrous scarring or organization is utilized by many investigators. The presence of neurogenic atrophy, presumably due to concomitant peripheral nerve involvement (if present), factors to a multisystem course of.
Generic 1.25 mg altaceRecent research of glutamate transporters suggest that balloon cells would possibly exhibit a protecting impact towards local ictal exercise, through increased glutamate clearance mechanisms. Neuroradiological correlation is paramount, notably in small and poorly oriented specimens. However, molecular, genetic and electrophysiology studies present differences Table 11. An related history of prenatal/perinatal threat factors (including prematurity, asphyxia, bleeding and mind injury) has been reported. Temporal lobe sclerosis was first acknowledged by Meyer within the earliest epilepsy surgical series. Interneurons are normally distributed,169,396 though discount of parvalbumin-positive neurons has been reported. The neuronal clustering is highlighted with neurofilament immunohistochemistry and could additionally be accompanied by abnormal horizontal bands of cortical myelinated fibres. The entire cortical thickness may be affected (a-laminar) or particular layers could additionally be lacking. Immature neurons are outlined as spherical to oval cells (diameter 10�12 m) with a skinny rim of cytoplasm, rudimentary dendrites and absent neurofilament expression. Hypertrophic neurons resemble giant pyramidal neurons of layer V, however are abnormally located in the superficial cortical layers. Hypertrophic neurons may be overinterpreted as dysmorphic and identification of immature neurons is problematic in H&E sections alone. Arguing against this speculation, however, is that tumours creating from known cortical dysplasias are rare. The interpretation of these histological features as tumour precursor (developmental) lesions or secondary tumour buildings is still conjecture. As with any infiltrating tumour, the organization of the bordering cortex may be disturbed, the layering could additionally be indistinct and the cortex could appear paucicellular, with remaining neurons maloriented and even hypertrophic, simulating cortical dysplasia. An excess of hypertrophic layer I neurons was related to childish spasms in one study. Despite differences in methodologies concerning anatomical areas studied, kinds of neurons counted, cell counting methodology used (stereological versus two-dimensional counting methods), completely different underlying principal pathologies. Similar pathology has also been noted with different neurological conditions, similar to schizophrenia. The incidence of mind tumours in epilepsy sufferers is about four per cent and the frequency of epilepsy in brain tumour sufferers is 30 per cent or more, relying on the tumour kind. They are typically slowly growing, low grade, cortically primarily based tumours, more typically arising in youthful patients and often exhibiting neuronal along with glial differentiation. The primary tumour varieties reported in epilepsy surgical collection are summarized in Table 11. Mechanisms of Epileptogenicity in Tumours the propensity to develop seizures is larger in tumours located within the frontal, temporal or insular cortex, with tumour dimension and price of growth doubtlessly being related. The sluggish development fee of these tumours, suitable with lengthy survival, is most likely going a crucial factor within the induction of secondary cellular and community reorganization in adjoining cortex and even distant sites because the hippocampus. Early surgical procedure is at present regarded as the optimum treatment, each for the epilepsy and to reduce threat of further haemorrhage; 84 per cent of patients with cavernous angiomas turn out to be seizure free. In a recent study there was no affiliation between neuronal discharges with intraoperative electrocorticography and the density of haemosiderin within the resected cavernoma. Glioneuronal hamartomas have been described involving the cortex, particularly temporal and frontal lobes, and symbolize circumscribed masses of mature however haphazardly arranged cell sorts, generally in association with adjoining cortical dysplasia. General Concepts of Epileptogenesis in Focal Epilepsy (a) (b) 723 11 (c) (d) (e) 11. The hypothalamic hamartoma has a robust association with intrinsic subcortical epileptogenesis and gelastic seizures. It consists of cytologically regular, small and huge neurons320 and may be causally linked to secondary cortical epileptogenesis. Epileptogenesis is often divided into three stages: (i) the acute occasion (the triggering insult or initial seizure); (ii) a latent interval (clinically silent); and (iii) spontaneous seizures. Understanding epileptogenesis is important to figuring out new therapeutic targets. This contains reduction in inhibitory neurons and synapses, elevated expression, assembly and function of excitatory neurotransmitter receptors or channels. Experimental information affirm that synaptic remodelling can happen because of seizures quite than as a major abnormality. Abnormal synchronization of neurons may be a further mechanism related to the technology of seizures. Interneuronal populations, via reference to a number of cells, can enhance this course of. Electrophysiological studies in vivo affirm that in focal lesions, the seizure onset zone could show irregular neuronal synchronization, though functionally isolated from surrounding brain regions. Inflammation could be a consequence in addition to a reason for seizures, however contribute to their perpetuation in a vicious loop. Experimental knowledge supports the speculation that seizures can induce brain irritation and that recurrent seizures worsen mind inflammation and should contribute to neuronal loss. A genetic predisposition for sustained inflammatory reactions, such as gene polymorphisms, may also contribute. Patients usually present with a subacute onset of seizures related to neurological signs, cognitive and behavioural adjustments. There is comparatively limited data regarding the composition and severity of the mobile infiltrates in these situations, primarily based on a few case reports. The immunological mechanisms are poorly understood, but autoantibodies in opposition to floor receptors could additionally be pathogenic, supported by constructive responses to plasmapheresis in some cases. Seizures are sometimes refractory to drug treatment and embrace partial motor seizures, secondary generalized seizures and epilepsia partialis continua, the latter afflicting about half of sufferers. Adult-onset circumstances, which account for 10 per cent,42 might show a extra variable, focal, delicate and protracted medical course. The early stages are characterized by more lively persistent irritation and less scarring than the later phases. General Concepts of Epileptogenesis in Focal Epilepsy (a) (b) (c) 727 11 (d) (e) (f) 11. B-lymphocytes are found less incessantly in perivascular cuffs, although plasma cells are rare. Widespread microglial activation, as nicely as microglial clusters and nodules could additionally be seen, however macrophage infiltrates are unusual. Patchy neuronal degeneration, neuronophagia and neuronal dropout are current in early levels. In instances the place post-mortem tissue is on the market, true bilateral disease with associated inflammatory change is uncommon. Autoantibodies may mediate damage by activation of excitatory receptors causing seizure discharges and excitotoxic neuronal demise or complement activation.
Generic 5mg altace with visaAt the ultrastructural degree this corresponds to the presence of fibrillar constructions with characteristic dimensions and periodicity. Classical plaques or neuritic plaques are characterized by a dense central core of amyloid surrounded by a less compact peripheral halo of amyloid. The dense core and peripheral halo are sometimes separated by a clear zone that contains 872 Chapter 16 Dementia 16. The darkish background staining represents a combination of neurofibrillary tangles and neuropil threads. Some plaques have a perivascular orientation, normally in affiliation with amyloid angiopathy. The fine construction of neuritic plaques highlights their complexity, as described in 1964 in the pioneering electron microscopic research by Kidd477 and Terry et al. Processes of microglia interdigitate with and surround wisps of fibrillar amyloid. A may also be detected in the cytoplasm of plaque astrocytes505 and can additionally be detected within neuronal cytoplasm. The change in staining pattern on the cytoarchitectural boundary (arrow) is dramatic. Investigations using confocal microscopy suggest that the neuronal harm is linked to the structural traits of amyloid plaques, with fibrillar types being related to dystrophic neuritic adjustments. They are more ample in superficial cortical layers, whereas plaques with dense amyloid cores are more frequent in deep cortical layers. Certain anatomical areas, such because the molecular layer of the cerebellum, usually have diffuse plaques Fleecy, lake-like and subpial A deposits Fleecy deposits are found in entorhinal layers, and lake-like deposits are typical of the parvocellular layer of the presubiculum. Compact or burnt-out plaques are characterised by a dense core and not using a peripheral rim of non-compact amyloid and often with out a lot neuritic dystrophy or reactive glia. Dense-cored or compact plaques are also more frequent in main cortices, such because the visible and motor cortices, whereas neuritic, primitive and diffuse plaques predominate in multimodal affiliation areas and within the limbic lobe. Increased amyloid burden, as measured with amyloid imaging, is related to changes in cortical network architecture. They are spherical lesions that stand out towards the pale-staining background of the neuropil and sometimes seem to displace normal buildings as would a mass lesion. They are negative or weakly stained with amyloid stains and have been referred to as preamyloid deposits. As in smaller diffuse plaques, these bigger deposits are composed of loosely organized A deposits that lack amyloid staining properties. Fleecy deposits and band-like subpial deposits are common in association with cerebral amyloid angiopathy. The extent of subpial amyloid deposition correlates with the severity of amyloid angiopathy. A Plaque-Associated Molecules Immunohistochemistry has revealed a variety of molecules in A plaques, either immediately related to the amyloid deposits or inside cells associated with plaques. Their presence reflects deposition of amyloid within the extracellular area, products related to harm to adjacent cells, inflammatory response components, and components associated to aggregation or dispersal of the amyloid. Dense amyloid cores could be seen as eosinophilic structures (c), which also stain strongly with Congo red. Capillaries and veins may also be involved however blood vessels in the white matter are typically spared. Amyloid angiopathy tends to be most severe within the occipital cortex, however its severity bears little or no relationship to the frequency with which plaques and neurofibrillary tangles are found. These embody hereditary cerebral haemorrhage with amyloidosis (Dutch, Icelandic and Finnish types), familial amyloid angiopathy with deafness and ocular haemorrhage (Danish type), and familial British dementia with amyloid angiopathy. Plaques showing ubiquitin staining with each granular and curvilinear patterns (c) are usually associated with tau immunoreactivity. Some of those are useful in neuropathological diagnosis and others are more of analysis interest. Numerous neurites filled with dense our bodies and paired helical filaments (arrows) along with intercellular accumulations of amyloid (asterisks) are seen. The relatively normal adjoining neuropil with many synapses is current on the right. Amyloid fibrils (A) are seen in close opposition to the cytoplasmic boundaries (Cyt R, arrows) of a cell inside a neuritic plaque. The significance of Hirano our bodies remains unsure however they seem to characterize a degenerative change in the cytoskeletal microfilament system. Hirano bodies share antigenic determinants with several cytoskeletal proteins, including most prominently F-actin309 and actin-binding proteins similar to -actinin, tropomyosin, vinculin, and cofilin. Electron microscopy shows that inclusions have a double membrane and exhibit electron-dense granular cores within a translucent matrix. Stage four: granulovacuolar degeneration extends to amygdala and/or the hypothalamus. Stage 5: granulovacuolar degeneration reaches cingulate cortex and occasionally frontal and parietal cortices. The plaques may be stained by antibodies to A peptide (b) and may include variable quantities of tau protein. Ultrastructurally, the neurites seem as swollen nerve terminals crammed with dense bodies, vesicles and degenerating organelles. These lesions are most plentiful within the hippocampus, however can sometimes be found in entorhinal cortex as properly. Hirano physique in a hippocampal pyramidal cell from a affected person with parkinsonism� dementia complex of Guam. Neurofibrillary tangles are frequently seen in residual neurons of the locus coeruleus. Defects in opioid systems have been reviewed116 with the suggestion that these can contribute to several downstream pathways leading to scientific illness. Two such factors, nerve growth factor and brain-derived neurotrophic factor,218 promote survival (c) sixteen. A proportion of granulovacuoles is immunoreactive with antibodies to phospho-tau (c). Autopsies are needed not only to verify diagnoses and outline overlapping and blended pathologies, but in addition to check new markers and to assess the outcomes of quickly rising therapy methods. Stage B: neuritic plaques present in neocortical association areas and reasonable hippocampal involvement. The BrainNet Europe Consortium has additionally put forward a validated system for assessment of tangles based on a staging system based on the Braak system. These diagnoses ought to be readily obvious with tau immunohistochemistry that reveals presence of glial in addition to neuronal lesions and intensive involvement of subcortical mind areas. The cleavage site for -secretase is in the middle of the A sequence and precludes production of A.
Order cheap altace onlineVesicular: no surrounding parenchymal response round a viable cysticercus (indicating tolerance), non-enhancing. Granular-nodular: irregular perilesional oedema, the fluid content of the cyst being isodense with the parenchyma, and a capsule. This stage correlates with the florid inflammatory response to a degenerating cyst, and is related to seizures. Neuropsychological exams counsel that neurocysticercosis also contributes to abnormal behavioural perform. The major inflammatory reaction to cysts is mainly Th2 mediated; antibody ranges correlate with disease severity. As with falciparum cerebral malaria, neurocysticercosis research throws up ever extra complexities in our understanding of the pathogenesis because the scientific heterogeneity outcomes from advanced interactions among parasite, host and environmental factors. They could additionally be positioned in the ventricle, the cortical parenchyma (70 per cent) or within the meningeal spaces. The cysticercus is a bladder containing fluid and an inverted head, or protoscolex. The wall is 100�200 m thick and has an outer tegument, with microvilli on the surface. These merge right into a loose parenchyma that characteristically contains many haematoxyphilic calcareous our bodies (corpuscles) � a typical function of several cestode larvae. These hooklets are about one hundred ten m long, birefringent, visible on haematoxylin and eosin (H&E) staining and particularly well stained red with the Ziehl�Neelsen technique. Viable cysts evoke just about no inflammatory response, and if brain is examined, there may solely be a minimal fibrous capsule round, and no inflammatory cells. The cysticercus structure becomes less distinct, and the entire lesion may resemble an abscess. As the cysticercus dies, it calcifies and the irritation becomes extra mononuclear and fewer marked. A large post-mortem examine in Brazil found that one quarter of cysts contained viable larvae. There is hydrocephalus from obstruction of the ventricles and quite a few cysticerci are scattered throughout the parenchyma and ventricles. Serology could have a role, but is complicated by the fact that antibodies indicate earlier an infection in addition to presumably current energetic illness. The sensitivity of serology in single cyst disease is <50 per cent, but approaches Nematode Infections (a) 1271 21 (b) 21. The invaginated scolex is clearly seen, and the rim of fibrous tissue around the cyst. Surgery is used diagnostically, for accessible cysts in basal cisterns, and neuroendoscopy can remove intraventricular cysts; and a ventriculoperitoneal shunt could also be required for hydrocephalus. It is present in Africa, Europe and 1272 Chapter 21 Parasitic Infections the Americas. Infection is via the eggs in the faeces; when ingested, they move into the circulation and become coenurus cysts within the mind and meninges, subcutaneous tissue, skeletal muscle, the attention and around the spinal twine. Some cases can be mistaken for a hydatid cyst till tissue diagnosis upon elimination. Over years it grows into the hydatid cyst, and will unfold to other elements of the body. The scolices within the cyst turn out to be the top segments of future grownup tapeworms within the host intestine. Man acquires hydatid cyst disease by accidentally ingesting canine faeces containing eggs. Iraq, northern Kenya), the cyst is so common that consideration of a tumour in any a part of the physique has to embody hydatid cyst within the prognosis. The cyst behaves as a spaceoccupying lesion, thrilling normally little host inflammatory reaction and slightly fibrosis. Clinical Features Within the mind or head, the order of frequency of website is the mind parenchyma, the ventricles,88 extradural location, the cerebellum and the orbit. Clinical presentation is with focal neurological signs, seizures, hemiparesis, chorea and speech problems. This offers rise to the scolices both instantly or from smaller internal brood capsules. The scolices are characteristic: 200 m long ovoid mobile constructions with 4 spherical suckers, a rostellum and two rows of hooklets. These features are higher appreciated on cytology preparations than in histopathological slides. The hooklets retain carbol fuchsin, so are highlighted by a Ziehl�Neelsen stain; this is helpful if the scolices have degenerated and died, as a result of the hooklets remain within the cyst. Around a viable unruptured cyst, the host inflammatory response is normally minimal, with little astrocytosis. However, because the cyst dies, it generates a extra marked, allergic, inflammatory response, with polymorphs, eosinophils and granulomas, and fibrosis. Presentation is with Hydatid Disease In man, there are two totally different hydatid infection syndromes, triggered respectively by Echinococcus granulosus: classical hydatid cyst disease; Echinococcus multilocularis: much less widespread alveolar hydatid disease. These launch eggs into the faeces, which are ingested by sheep, cattle, goats, camels and other herbivores. In the duodenum of those intermediate hosts, the egg hatches and the oncosphere burrows by way of the intestine wall and reaches the Life Cycle and Epidemiology 21. Nematode Infections 1273 6 Scolex attaches to gut 21 1 Adult in small intestine 5 Protoscolex from cyst 2 Ingestion of cysts (in organs) (dogs and other canidae) (sheep, goats, swine, and so forth. Within the bone in most surgical specimens, there are fragments of degenerate laminated membrane related to a continual osteomyelitis reaction. Tissue biopsy could also be accomplished for diagnostic functions, but 1274 Chapter 21 Parasitic Infections aspiration of cyst contents can show scolices, hooklets and optimistic serology. The danger of anaphylactic shock from unintended spillage of hydatid antigen during surgery is low. Imaging reveals a multiseptate irregular mass, partly strong, partly cystic, with incomplete rim enhancement. The pathology is of an invasive cyst with thin laminated membrane; protoscolices may be scanty or absent. This is eaten by frogs and snakes and some mammals and a plerocercoid larva (the sparganum) develops. When these second intermediate hosts are eaten by dogs or cats, the cycle is accomplished. Man turns into by chance infected by drinking water contaminated by copepods, or consuming undercooked meat of the second intermediate host; or hardly ever by utilizing poultices of contaminated animal flesh on pores and skin lesions. In the brain, because it migrates, the larva causes headache seizures, focal neurological signs and focal haemorrhage. Migration through the brain is a key diagnostic feature on imaging in cerebral sparganosis. Histologically, the worm has small easy muscle bundles via the length, excretory ducts and calcareous corpuscles throughout the mesenchyme, and a typical cestode cuticle.
References - Uetani N, Bouchard M: Plumbing in the embryo: developmental defects of the urinary tracts, Clin Genet 75(4):307-317, 2009.
- Harmann P, Kron I, et al: Elevated intra-abdominal pressure and renal function, Ann Surg 196:594-597, 1982.
- Heinrich M, Oberbach A, Schlichting N, et al: Cytokine effects on gap junction communication and connexin expression in human bladder smooth muscle cells and suburothelial myofibroblasts, PLoS ONE 6(6):e20792, 2011.
|
|


