"Purchase viagra vigour overnight delivery, impotence natural supplements."By: Jonathan Tze-Wei Ho, M.A., M.D. - Assistant Professor of Anesthesiology and Critical Care Medicine
 https://www.hopkinsmedicine.org/profiles/results/directory/profile/10003132/jonathan-ho
Order 800mg viagra vigour with mastercardAt the delicate end of the spectrum are gastric dysrhythmias, that are refined electrical disturbances related to mild to extreme nausea symptoms. At the extreme finish of the spectrum, antral hypomotility and profound gastroparesis are related to prolonged postprandial fullness, vomiting, bloating, weight loss, and malnutrition that will require enteral or parenteral dietary help. Gastric neuromuscular issues range from irregular fundic leisure and emptying to gastric dysrhythmias and antral hypomotility and gastroparesis. Pyloric sphincter dysfunction, duodenal dysfunction, antroduodenal dyscoordination, and vagal hypersensitivity may all be current in some sufferers with gastric neuromuscular disorders. The pyloric sphincter is a key pathophysiologic factor in over 20% of patients with gastroparesis. Gastroparesis Gastroparesis means "paralysis" of the stomach, as defined by the delayed rate of emptying of a standard take a look at meal from the stomach in the absence of mechanical obstruction. Data from Olmstead County, Minnesota, indicate an age-adjusted prevalence of particular gastroparesis of 9. The definite gastroparesis group was established on the idea of standard gastric scintigraphy results. These sufferers usually have diabetes for greater than 10 years, erratic and elevated glucose levels, peripheral neuropathy, nephropathy, and heart problems. One important manifestation of gastric emptying dysfunction in patients with insulin-dependent diabetes is erratic glucose control, particularly with surprising hypoglycemic episodes in the postprandial period if the similar old insulin doses are administered before meals. When postprandial insulin ranges enhance following insulin injection and yet gastric emptying is delayed, nutrient supply into the duodenum and intestinal glucose absorption are delayed. Thus, plasma glucose ranges decrease in response to the insulin remedy and symptomatic hypoglycemia develops unexpectedly. Hypomotility of the fundus and hypercontractility of the pylorus were found in db/db mice. Postsurgical Gastroparesis Gastroparesis happens in a subset of sufferers present process delicate or radical abdomen operations that vary from vagotomy to fundoplication to antrectomy. Truncal vagotomy produces complex results on the neuromuscular function of the stomach. After vagotomy, the fundus fails to chill out usually after meals, leading to fast filling of the antrum. But in patients present process in depth resection of the antrum and corpus, prolonged signs and continual gastric neuromuscular dysfunction are likely. Lower esophageal resection for esophageal cancer contains resection of the fundus. Pyloroplasty is performed to facilitate gastric emptying, but the lack of the fundus and variable quantities of the corpus (that could encompass the pacemaker region) typically results in chronic nausea, gastric dysrhythmias, and gastroparesis. Ingested meals is retained within the remnant fundus and fails to empty into the corpus203; the corpus fails to mix and empty gastric contents even though the anastomosis is extensively patent. The Roux-en-Y gastroenterostomy operation might result within the Roux syndrome during which postprandial pain, bloating, and nausea develop. Delayed gastric emptying is as a result of of "useful obstruction" by the Roux limb as the neuromuscular dyssynchrony throughout the Roux limb prevents emptying of the stomach. In the gastric "sleeve" resection for weight problems, two thirds of the abdomen is eliminated together with portions of the fundus, corpus, and antrum. After the sleeve resection, gastric emptying of liquid and stable take a look at meals is accelerated, however there are few studies available for evaluate. Postfundoplication gastroparesis and early satiety, bloating, prolonged fullness, and nausea may occur. These patients have altered fundic leisure, delayed gastric emptying, and gastric dysrhythmias, probably on the basis of vagal nerve injury during or after the fundoplication process. Gastric clean muscle dysfunction is one other mechanism of delayed gastric emptying in some sufferers with diabetes. Gastric easy muscle contractility in diabetic rats is reduced in response to electrical stimulation. Type 2 diabetes mellitus sufferers with gastroparesis are older, have milder delays in gastric emptying, and more severe early satiety. This affected person had electrical and contractile abnormalities of the stomach as documented by the tachygastria and gastroparesis. Gastric myoelectrical exercise in sufferers with gastric outlet obstruction and idiopathic gastroparesis. Ischemic gastroparesis is distinct from acute mesenteric ischemia, which presents as an belly catastrophe with an acute abdomen and gangrenous small intestine (see Chapter 118). Chronic mesenteric ischemia is often due to progressive atherosclerosis or hyperplasia of the intima of the arteries of the celiac, superior mesenteric, or inferior mesenteric artery. Collaterals of those obstructed arteries type over time so that neuromuscular function of the abdomen is preserved, at least for a while. Bypass graft surgery or dilatation of the stenotic arteries results in resolution of symptoms, eradication of gastric dysrhythmias, and reversal of gastroparesis. Patients with idiopathic (discussed below), diabetic, or postsurgical gastroparesis might have a subtype of gastroparesis-obstructive gastroparesis as a end result of pyloric dysfunction. This subtype is important as a outcome of endoscopic and surgical remedies are directed in the course of the pylorus. Fixed Pyloric Obstruction Fixed obstructive gastroparesis refers to delayed emptying as a end result of mechanical obstruction at the pylorus or duodenal bulbar or postbulbar area by tumor, chronic peptic ulcer or irritation, rings, or webs. Gastroparesis may very well be obstructive gastroparesis as a end result of pyloric stenosis or postduodenal bulb cancer. Functional Pyloric Obstruction A extra delicate type of gastric outlet obstruction occurs in pylorospasm. The "spasm" of the pylorus may trigger postprandial right upper quadrant belly ache within the setting of gastroparesislike signs. Pylorospasm of the pylorus prevents regular gastric peristaltic waves from empting chyme into the duodenum. In these sufferers dilatation of the pylorus with a 20-mm balloon for 2 minutes or botulinum toxin A injections into the pylorus decreased postprandial symptoms. If these problems are recognized, then the gastroparesis could also be secondary to these specific diseases. Importantly, postprandial misery signs are additionally just like signs associated with gastroparesis. These neurologic issues embody Ehlers-Danlos syndrome,239 postural orthostatic tachycardia syndrome,240 spinal twine and head injuries, amyotrophic lateral sclerosis, myasthenia gravis, a big selection of muscular dystrophies, and Parkinson illness (see Chapter 37). This mismatch of plasma glucose and insulin may find yourself in symptomatic hypoglycemia. The fast small bowel transit and poor absorption of the ingested nutrients result in an osmotic form of diarrhea. Idiopathic fast emptying is identified in sufferers with no history of gastric operations or different causes. However, the ingestion of meals stimulates the disordered gastric neuromuscular equipment, and early satiety, extended epigastric fullness, epigastric discomfort or ache, delicate to extreme nausea, and vomiting are then experienced. Vomitus that incorporates undigested, chewed food is robust evidence for gastroparesis. Prolonged postprandial fullness, weight reduction, and female gender are predictive factors for gastroparesis.
Purchase generic viagra vigourMost are situated alongside the higher curvature of the abdomen and are extragastric, although intramural extension has been reported. Premalignant changes and frank malignant transformation to adenocarcinoma have been reported,30,31 and peritoneal gliomatosis has been noticed. Fortunately, even those cases with malignant histologic options or extension into adjoining tissues have a superb prognosis. The newborn toddler with a teratoma may be delivered prematurely or have respiratory misery on the premise of elevated belly strain. Delivery may be difficult, putting the toddler at risk for injuries such as shoulder dystocia. Gastric teratoma associated with gastric perforation, mimicking meconium peritonitis, has Gastric Volvulus See Table 49. Incidence is highest among whites (especially northern Europeans), whereas incidence is decrease amongst African Americans and Africans and lowest amongst Asians. Others at elevated risk are first-born male infants, especially those with high start weights or born to professional dad and mom. Initially, infants present with mild spitting, which progresses to projectile vomiting following feedings. Vomiting could also be so forceful as to exit via the nostrils, in addition to the mouth. Early within the course, the infant stays hungry following vomiting episodes but, with time, loses interest in feeding and should present wasted and severely quantity depleted. The basic physical indicators are a palpable pyloric mass and visual peristaltic waves. The palpable "olive" is most easily felt in a wasted patient, instantly following emesis or aspiration of the stomach. The location of the olive varies from the extent of the umbilicus to near the epigastrium. The pyloric mass is palpable in 70% to 90% of affected infants, depending on the experience and persistence of the examiner. Emptying the abdomen by nasogastric tube placement and palpation of the abdomen with the infant within the susceptible position could enhance detection. Many infants seem jaundiced because of an indirect hyperbilirubinemia associated to quantity depletion and, maybe, malnutrition. When the presentation is typical and the olive palpated, no research are needed. However, within the minority of infants with projectile vomiting, definitive prognosis requires radiologic research. Non-contrast radiography demonstrates a distended abdomen with paucity of fuel beyond the stomach. The numeric value for the lower restrict of pyloric muscle thickness has various in reviews within the literature, ranging between three and four. Many think about the numeric value less essential than the overall morphology of the canal and real-time observations. Contrast radiography have to be carried out rigorously, and gastric contents ought to first be aspirated. Characteristic findings include an elongated slim pylorus with the looks of a "double channel. The resected pylorus demonstrates regular mucosa and marked circumferential thickening of the muscularis propria. In distinction with the infantile kind, the physical examination may not be useful because the pyloric mass is tough to palpate in adults. On distinction radiography, the elongated slender pylorus is once more obvious; gastric emptying is delayed, and the abdomen may be dilated. Treatment Traditionally, surgical pyloromyotomy or resection of the concerned area has been thought-about the process of selection. Because of the chance of a small focus of carcinoma, surgical resection of the pylorus has been really helpful. Depending on severity, fluid and electrolyte repletion can normally be accomplished inside 24 hours. Definitive remedy is the Ramstedt pyloromyotomy, which entails a longitudinal incision through the hypertrophied pyloric muscle right down to the submucosa on the anterior surface of the pylorus. After spreading the muscle, the intact mucosa bulges via the incision to the extent of the incised muscle. An different operation is the pyloric traumamyoplasty, the place the pylorus is grasped with a Babcock clamp that disrupts the hypertrophied circular muscle tissue in 2 places. Nonoperative remedy consists of using anticholinergic medications59 and paste-consistency feedings till such time that the muscle hypertrophy resolves. The prognosis following surgery is superb, with the infant resuming normal progress and growth. Duodenal Atresia and Stenosis Duodenal atresia and stenosis are congenital defects characterized by full and partial obstruction of the duodenum, respectively. Atresias happen in varied anatomic configurations including a blind-ending pouch with no connection to the distal duodenum (least common), a pouch with a fibrous twine connecting to the distal duodenum, or a complete membrane obstructing the lumen (most common). All of those lesions happen with greatest frequency close to the ampulla of Vater, with most lesions (80%) occurring distal to this landmark. The total incidence of the 3 anomalies combined is roughly 1 per 200,000 stay births, with a slight predilection for women. This is distinct from atresia or stenosis of the jejunum and ileum, which are brought on by vascular accidents in utero. Trisomy 21 is strongly related to duodenal atresia/stenosis/web in that anyplace from 25% to greater than 50% of cases occur in infants and kids with this chromosomal anomaly. Familial association is rare, although isolated case reviews recommend a attainable genetic association. Emesis is often bilious as a result of most lesions happen distal to the entry of the bile duct into the duodenum. Nonbilious emesis is seen in 15% to 20% of cases secondary to more proximal obstruction. Any child with trisomy 21 and vomiting (especially bile-stained) requires additional evaluation for duodenal stenosis. Duodenal stenosis or a partial membrane may current at any age, depending on the degree of obstruction. Infants and kids present with vomiting, failure to achieve weight adequately, and/or aspiration. Vomiting may be intermittent and of variable severity such that symptomatic lesions could stay undiagnosed for months to years. Noncontrast radiographs of the toddler with duodenal obstruction classically demonstrate the presence of air in the abdomen and within the first portion of the duodenum-the "double-bubble" signal. The absence of air past the second bubble must be interpreted as probable duodenal atresia. Contrast radiography is mostly effective in demonstrating atresias, stenosis, membranes, and other anomalies leading to exterior compression of the duodenum. In addition, regular or abnormal rotation and fixation of the bowel may be assessed.
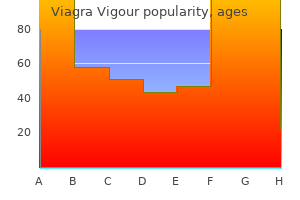
Purchase viagra vigour overnight deliveryA 60 sec Bradygastria (low-amplitude) 500 �V B 60 sec Bradygastria (high-amplitude) 500 �V C 60 sec Normal Capsule Technology the wi-fi ingestible capsule described beforehand measures contractions of the stomach wall. After a regular check meal, irregular contractions happen at 1 to three per minute and are according to manometric recordings from the antrum. In sufferers with gastroparesis, capsule studies showed a decreased motility index in the course of the 20 to half-hour before emptying of the capsule, but a standard motility index within the 10 minutes before the capsule was emptied into the duodenum. These studies counsel that standard terminal antral contractions may be maintained even in sufferers with gastroparesis, whereas antral contractility required for trituration of digestible foodstuffs is abnormal. A, Tachygastria, an abnormally fast signal at 6 cycles per minute (cpm), proven by dots. After ingestion of most stable or liquid meals, a socalled frequency dip happens within the first 10 to 15 minutes after the meal. The frequency dip displays modifications ensuing from marked gastric leisure and accommodation of the test meal associated to the volume or the temperature of the meal. Recordings that have mixtures of tachygastria and bradygastrias are termed nonspecific or mixed gastric dysrhythmias. Slow frequencies are additionally current from 1 to 2 cpm (bradygastrias) and from 4 to 9 cpm (tachygastrias) in patients with nausea with or without gastroparesis. The barostat balloon was designed to measure modifications in tone (or gastric relaxation) and volume in the more spherical areas of the proximal abdomen. As the fundus and proximal abdomen relax in response to the take a look at meal, more air is concomitantly infused into the balloon to preserve the established baseline intraballoon strain. Failure of fundic rest has also been recorded in patients with gastroparesis. Histopathologic Studies in Gastric and Pyloric Neuromuscular Disorders Efforts to define the histopathologic foundation of gastric neuromuscular problems have offered fundamental information for the evolving subject of neurogastroenterology. Thus, these disorders could also be thought of Cajalopathies or gastric enteric neuropathies or, extra likely typically, combinations of each. Results from histochemical studies of full-thickness gastric and pyloric tissue also provide new instructions for understanding the neuromuscular dysfunction of the stomach and stimulate ideas for novel therapeutic approaches. In the water-load satiety take a look at, water is consumed over a 5-minute interval until the topic feels full. The pylorus is troublesome to examine with reference to fasting and postprandial function in awake topics. Thus, liquid and stable vitamins are rapidly emptied or "dumped" into the duodenum or jejunum. The dumping syndrome signs embody nonspecific belly discomfort, bloating, and nausea and vomiting. These signs are usually experienced in the first hour after ingestion of foods. Sweating and lightheadedness, nonetheless, might happen and be followed by stomach cramps and diarrhea that occur 2 to four hours after the meal and are further clues to the dumping syndrome. A thorough evaluation of the causes of nausea and vomiting is required (see Chapter 15), and an acceptable differential analysis should be thought-about (see Box 50. Rumination refers to the easy return of ingested liquids and strong foods into the mouth with out burning, bitter taste, or nausea. Patients with rumination have impaired gastric lodging and a more delicate leisure of the lower esophageal sphincter strain in response to gastric distention. Abdominal pain, in contrast to the belly discomfort of bloating and nausea, happens in approximately 20% of patients with gastroparesis. On the opposite hand, the epigastric discomfort or ache in some gastroparesis patients might originate from the stomach: excessive muscle tone of the fundus, high-amplitude antral contractions, pylorospasm, or hypersensitivity of the stomach are potential causes of ache. The classes are (1) gastroparesis with gastric dysrhythmia, (2) gastroparesis with regular gastric electrical rhythm, (3) normal gastric emptying with gastric dysrhythmia, and (4) normal gastric emptying with normal gastric electrical rhythm. The 4 classes present a conceptual framework for understanding the spectrum of gastric neuromuscular disorders and providing an method to remedy (see Table 50. These sufferers may have fixed mechanical obstructions of the pylorus and duodenum which are reversible with operation. The gastroparesis-like signs could also be because of poor gastric relaxation or gastric visceral hypersensitivity in response to distension with the water load or caloric satiety tests. Diagnoses of nongastric issues should also be considered in this affected person group. Auscultation over the epigastrium could detect bruits that point out stenoses of the celiac or superior mesenteric arteries. Pain and tenderness which are precisely localized to healed belly incisions and improve when the pinnacle is flexed and anterior belly muscles are contracted (positive Carnett sign) suggest the ache is from an stomach wall syndrome and not the stomach. The reversible obstructive causes of gastroparesis because of mounted pyloric stenosis or useful pylorospasm and ischemic gastroparesis due to persistent mesenteric ischemia should be excluded as a outcome of these entities are reversible. If gastric emptying is normal, then gastric dysrhythmia and gastric accommodation problems will be the neuromuscular issues which may be relevant to the signs. Electrical Therapy Acustimulation Acustimulation (mild electrical stimulation of acupuncture points) reduces nausea of pregnancy, nausea because of chemotherapy brokers, postoperative nausea, and the nausea of motion sickness285,286 and symptoms related to gastroparesis. The remedy consists of prokinetics, antinauseant therapies, and dietary counseling. Metoclopramide, a substituted benzamide related to procainamide, is a helpful prokinetic antiemetic but has a "black box" warning. Cisapride was not permitted for gastric emptying disorders but increased gastric emptying charges and decreased dyspepsia symptoms in some patients. Gastric Pacing Low-frequency gastric stimulation utilizing a 3-cpm stimulus to pace or entrain the traditional sluggish wave rhythm in sufferers with gastroparesis seeks to stimulate 3 gastric peristaltic contractions per minute and enhance gastric emptying. In a similar study of 9 further patients, electrical stimulation was used to entrain the slow wave, and tachygastria was converted to normal 3-cpm rhythms in 2 sufferers. Adverse occasions because of gastric pacing units are discomfort at the website of electrical stimulation and fracture or dislodgement of the electrodes. Sequential Neural Electrical Stimulation Sequential neural electrical gastric stimulation is gastric pacing that makes use of a microprocessor to sequentially activate a collection of electrodes that encircle the distal two thirds of the abdomen. The stimulation sequence induces propagated contractions that trigger a forceful emptying of the gastric content material. Botulinum toxin relaxes the pyloric sphincter strain and is described later in endoscopic therapy. Lorazepam or alprazolam or different antianxiety medicines cut back nausea in some patients. An uncontrolled trial of tricyclic antidepressants alleviated nausea in approximately 70% of patients with unexplained nausea,283 however a current placebo-controlled trial showed that one tricyclic compound, nortriptyline, was no higher than placebo in reducing signs of gastroparesis. Endoscopic Therapy Endoscopic therapies check with drug or device therapies delivered to the related areas of the abdomen through endoscopes. The injection of botulinum toxin A into the pylorus to lower sphincter strain and to enhance gastric emptying and nausea and vomiting in patients with gastroparesis produced outcomes similar to placebo injections. Early studies with gastric-peroral endoscopic myotomy point out symptoms and gastric emptying improve after remedy. Step 1 is primarily electrolyte options which are consumed in small quantities over a 24-hour period to have the ability to avoid volume depletion.
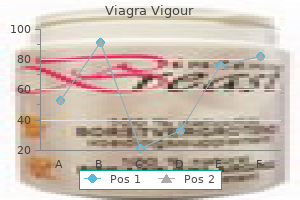
Buy viagra vigour 800 mg on lineThe time line illustrates the coordination and timing of occasions within the pharyngeal swallow on fluoroscopy. Esophagus the esophagus is a 20- to 22-cm tube composed of skeletal and clean muscle. The proportion of each muscle sort is species dependent, but in humans, the proximal 5% is striated, the middle 35% to 40% is combined with an rising proportion of easy muscle distally, and the distal 50% to 60% is totally smooth muscle. The outer longitudinal muscle arises from the cricoid cartilage with slips from the cricopharyngeus passing dorsolaterally to fuse posteriorly about three cm distal to the cricoid cartilage. This results in a posterior triangular area devoid of longitudinal muscle, Laimer triangle. Distal to Laimer triangle, the longitudinal muscle tissue kind a continuous sheath of uniform thickness across the esophagus. The adjacent, internal muscle layer is fashioned of round or, more precisely, helical muscle also forming a sheath of uniform thickness along the length of the esophagus. The extrinsic innervation of the esophagus is by way of the vagus nerve with motor neurons in nucleus ambiguus (striated muscle portion) and the dorsal motor nucleus of the vagus (smooth muscle portion). The proximal striated phase 1 and the distal smooth muscle esophageal contractile segments 2 and 3 are separated by a transition zone (P). The distal esophagus can also be divided into 2 distinct contractile segments (2 and 3), separated by a stress trough (M). Of curiosity is the idea of concurrent esophageal contraction illustrated by the vertical dashed arrows. The vagus also present sensory innervation; in the cervical esophagus, this is through the superior laryngeal nerve with cell our bodies in the nodose ganglion, whereas within the remainder of the esophagus, sensory fibers journey by way of the recurrent laryngeal nerve or, in probably the most distal esophagus, by way of the esophageal branches of the vagus. The esophagus also contains an autonomic nerve community, the myenteric plexus, positioned between the longitudinal and round muscle layers. Myenteric plexus neurons are sparse in the proximal esophagus, and their operate is unclear as a outcome of the striated muscle is immediately managed by nucleus ambiguus motor neurons. On the opposite hand, in the clean muscle esophagus preganglionic neurons within the dorsal motor nucleus of the vagus synapse on relay neurons in the myenteric plexus ganglia. A second nerve community, the submucosal or Meissner plexus, is situated between the muscularis mucosa and the circular muscle layer, but this is sparse in the human esophagus. Esophageal Peristalsis the esophagus is often atonic and its intraluminal stress closely reflects pleural stress, turning into adverse during inspiration. Primary peristalsis is initiated by a swallow and traverses the entire length of the esophagus; secondary peristalsis can be elicited in response to focal esophageal distention with air, fluid, or a balloon, starting on the locus of distention. The mechanical correlate of peristalsis is of a stripping wave that milks the esophagus clean from its proximal to distal end. A second swallow initiated while an earlier peristaltic contraction remains to be progressing within the proximal esophagus completely inhibits the contraction induced by the primary swallow. Deglutitive inhibition within the distal esophagus is attributable to hyperpolarization of the round clean muscle and is mediated by way of inhibitory ganglionic neurons within the myenteric plexus. Deglutitive inhibition can be demonstrated experimentally within the esophagus by distending an intraluminal balloon, which stimulates esophageal contraction. The physiologic management mechanisms governing the striated and clean muscle esophagus differ. The striated muscle receives completely excitatory vagal innervation, and its peristaltic contraction outcomes from sequential activation of the musculature. Striated muscle peristalsis is programmed by the medullary swallowing center in a lot the same means as is the pharyngeal swallow. The vagus nerves also exhibit control of main peristalsis in the smooth muscle esophagus, however the mechanism of vagal management is extra advanced than that of the striated muscle as a outcome of vagal fibers synapse on myenteric plexus neurons rather than immediately on muscle cells. However, the myenteric plexus also can orchestrate peristalsis independently of vagal activation; secondary peristalsis could be elicited anywhere along the sleek muscle esophagus despite extrinsic denervation. Regardless of central or ganglionic control, esophageal easy muscle contraction is in the end elicited by ganglionic cholinergic neurons. Less clear are the management mechanisms for the course and velocity of peristalsis. Nerve conduction research point out that neural stimuli initiated by swallowing reach the ganglionic neurons alongside the size of the esophagus essentially simultaneously. However, the latency between the arrival of the vagal stimulus and muscle contraction progressively increases, shifting aborally. The present hypothesis is that peristaltic direction and velocity end result from a neural gradient along the esophagus, whereby excitatory ganglionic neurons dominate proximally and inhibitory ganglionic neurons dominate distally. This group is in maintaining with the demonstration of 2 subsegments throughout the easy muscle phase with stress topography plotting, the first of which is strongly reactive to cholinergic medication. Clouse and colleagues pioneered this expertise, noting that peristalsis was not a seamless wave of pressurization, but rather a coordinated sequence of 4 contiguous contractile segments A transition zone exists between the first and second segments, characterised by the nadir peristaltic amplitude, slightly delayed development, and occasional failed transmission. Longitudinal Muscle the longitudinal muscle of the esophagus additionally contracts throughout peristalsis, with the online effect of transiently shortening the construction by 2 to 2. Similar to the pattern of round muscle contraction, longitudinal muscle contraction is propagated distally as an active section at a fee of two to four cm/s. However, unlike the round muscle, nerve stimulation studies suggest the longitudinal muscle to be free of inhibitory neural management. The esophagus then traverses the diaphragmatic hiatus and joins the abdomen nearly tangentially. Viewed intraluminally, this area extends within the gastric lumen, showing as a fold that has been conceptually referred to as a "flap valve" because elevated intragastric pressure forces it closed, sealing off the entry to the esophagus. The blue circles represent excitatory neurons, and the purple circles represent inhibitory neurons. A, In regular topics, cholinergic neurons are most dense proximally, changing into increasingly sparse distally. Conversely, inhibitory neurons are extra prominent distally and relatively sparse proximally. This inverse neural gradient causes increasing latency of the contraction as it progresses distally. With simultaneous vagal stimulation of ganglia alongside the length of the esophagus, contraction first happens proximally and propagates distally solely as the consequences of increasingly dense inhibition put on off. Thus, pharmacologic manipulation can alter both contractile vigor and timing of propagation. Conceptually, esophageal motor pathophysiology can be defined by alterations in these neural gradients. B, Patients with hypercontractility and normal (or fast) propagation might have a relative improve in excitatory neurons. C, Patients with lack of inhibitory neurons will lose deglutitive inhibition, and contractions will occur concurrently and prematurely. Vagal influence is similar to that of the esophageal physique, with vagal stimulation activating both excitatory and inhibitory myenteric neurons.
Order viagra vigour without prescriptionTreatment with soma tostatin analogs and chemoembolization of liver metastases for se vere hypoglycemia in malignant insulinomas. Somatostatin analogues within the therapy of gastroenteropancreatic neuroendocrine tumours, present features and new views. Highresolution evaluation of genetic alterations in small bowel carcinoid tumors reveals areas of recurrent amplification and loss. Expression of vascular endo thelial growth think about digestive neuroendocrine tumours. Inherited pancreatic endocrine tumor syndromes: advances in molecular pathogen esis, prognosis, management, and controversies. Multiple endocrine neoplasia type 1 and ZollingerEllison syndrome: a prospective examine of 107 circumstances and comparison with 1009 instances from the literature. Resolved and unresolved controversies within the surgical management of patients with ZollingerEllison syn drome. Diagnostic uses of radiolabelled somatostatin receptor analogues in gastroenteropancreatic endocrine tumours. Efficacy of evero limus in patients with metastatic insulinoma and refractory hypogly cemia. Diagnosis of insulinoma in a affected person with hypoglycemia with out apparent hyperinsulinemia. Surgical administration of pa tients with insulinomas: results of 292 circumstances in a single establishment. Surgical management of insulinomas: quick and longterm outcomes after enucleations and pancreatic resections. Laparoscopic surgery in sufferers with sporadic and a quantity of insulinomas associ ated with a number of endocrine neoplasia kind 1. Prospective examine of the clini cal course, prognostic elements, causes of demise, and survival in pa tients with longstanding ZollingerEllison syndrome. Hyperplastic, dysplastic, and neoplastic enterochromaffinlikecell proliferations of the fuel tric mucosa. Effect of chronic hyper gastrinemia on human enterochromaffinlike cells: insights from sufferers with sporadic gastrinomas. A potential study of gastric carcinoids and enterochromaffinlike cell adjustments in multiple endocrine neoplasia kind 1 and ZollingerEllison syndrome: identi fication of risk elements. Duodenal neuroendocrine tumors: classification, useful syndromes, diagnosis and medical remedy. Possible main lymph node gastrinoma: prevalence, pure historical past, and predictive factors: a prospective research. Bone metastases in pa tients with gastrinomas: a prospective study of bone scanning, soma 497. Determinants of metastatic fee and survival in sufferers with ZollingerEllison syndrome: a professional spective longterm examine. Growth of newly diag nosed, untreated metastatic gastrinomas and predictors of progress patterns. Management of the ZollingerEllison syndrome in patients with multiple endocrine neoplasia sort 1. Does the widespread use of proton pump inhibitors masks, complicate and/or delay the di agnosis of ZollingerEllison syndrome Studies on the interrela tion between ZollingerEllison syndrome, Helicobacter pylori, and proton pump inhibitor therapy. Prospective study of fasting serum gastrin in 309 sufferers from the National Institutes of Health and comparison with 2229 cases from the literature. Review article: strategies to decide whether hypergastrinaemia is due to ZollingerEllison syndrome somewhat than a extra frequent benign trigger. The ZollingerEllison syn drome: dangers and consequences of interrupting antisecretory remedy. Positive intravenous se cretin take a look at in patients with achlorhydriarelated hypergastrinemia. Importance of surveillance for a number of endocrine neoplasia1 and surgical procedure in patients with spo radic ZollingerEllison syndrome. Comparison of surgical leads to sufferers with advanced and restricted disease with multiple endocrine neoplasia sort 1 and ZollingerEllison syndrome. Prospective examine of surgical resection of duodenal and pancreatic gastrinomas in mul tiple endocrine neoplasia sort 1. Partial pancreaticoduode nectomy can provide remedy for duodenal gastrinoma associated with multiple endocrine neoplasia type 1. Cutaneous manifestations of inside malignant tumors" by Becker, Kahn and Rothman, June 1942. Glucagonoma and the gluca gonoma syndrome cumulative expertise with an elusive endo crine tumour. Endocrine pancreatic tumors with glucagon hypersecretion: a retrospective study of 23 circumstances during 20 years. Foetal proglucagon course of ing in relation to grownup urge for food control: classes from a transplant in a position rat glucagonoma with extreme anorexia. Reproduction of options of the glucagonoma syndrome with steady intravenous glucagon in fusion as remedy for tumorinduced hypoglycemia. Glucagon therapy as a possible explanation for erythema necrolyticum migrans in two neonates with persistent hyperinsulinaemic hypoglycaemia. Glucagonomaassociat ed neuropsychiatric and affective signs: diagnostic dilemmas raised by paraneoplastic phenomena. Secretinreceptor and secretin receptorvariant expression in gastrinomas: correlation with clini cal and tumoral options and secretin and calcium provocative take a look at results. Prospective study of gastrin pro vocative testing in 293 patients from the National Institutes of Health and comparability with 537 instances from the literature. Validation of a new endo scopic method to assess acid output in ZollingerEllison syn drome. Use of omeprazole in ZollingerEllison syndrome: a prospective nineyear examine of effi cacy and safety. A potential study of the effectiveness of low dose omeprazole as preliminary remedy in Zollinger Ellison syndrome. Effect of parathy roidectomy in patients with hyperparathyroidism, ZollingerEllison syndrome, and a number of endocrine neoplasia kind I: a prospective examine. Association of longterm proton pump inhibi tor remedy with bone fractures and effects on absorption of cal cium, vitamin B12, iron, and magnesium. Iron absorption in patients with ZollingerEllison syndrome treated with long run gastric acid antisecretory remedy. Effect of longterm gasoline tric acid suppressive therapy on serum vitamin B12 ranges in sufferers with ZollingerEllison syndrome.
Generic viagra vigour 800 mg overnight deliveryGuidelines for the management of Helicobacter pylori an infection in Japan: 2009 revised edition. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Sequential remedy versus commonplace triple-drug therapy for Helicobacter pylori eradication: a randomized trial. Meta-analysis: sequential remedy appears superior to standard therapy for Helicobacter pylori infection in patients naive to therapy. Sequential versus triple therapy for the first-line remedy of Helicobacter pylori: a multicentre, open-label, randomised trial. Efficacy of 5-day levofloxacin-containing concomitant remedy in eradication of Helicobacter pylori infection. Risk of recurrent Helicobacter pylori an infection 1 year after preliminary eradication remedy in 7 Latin American communities. Meta-analysis: sequential therapy seems superior to commonplace therapy for Helicobacter pylori an infection in sufferers na�ve to therapy. A randomized study comparing levofloxacin, omeprazole, nitazoxanide and doxycycline versus triple remedy for the eradication of Helicobacter pylori. Penicillin allergy: optimizing diagnostic protocols, public health implications, and future research needs. Iron-deficiency anemia and Helicobacter pylori infection: a evaluate of the proof. Efficacy, security and immunogenicity of an oral recombinant Helicobacter pylori vaccine in youngsters in Chia: a randomized, double-blind, placebo-controlled, part 3 trial. Protective effect of green tea on the risks of continual gastritis and abdomen most cancers. Gastro-protecting effect of gefarnate on continual erosive gastritis with dyspeptic signs. An openlabeled study of rebamipide remedy in persistent gastritis sufferers with dyspeptic symptoms refractory to proton pump inhibitors. Bismuth-based quadruple therapy using a single capsule of bismuth biskalcitrate, metronidazole, and tetracycline given with omeprazole versus omeprazole, amoxicillin, and clarithromycin for eradication of Helicobacter pylori in duodenal ulcer sufferers: a potential, randomized, multicenter, North American trial. One-day quadruple remedy compared with 7-day triple remedy for Helicobacter pylori an infection. Review article: Rifabutin within the treatment of refractory Helicobacter pylori infection. Risk factors for failure of Helicobacter pylori therapy-results of a person information analysis of 2751 patients. Update on non-bismuth quadruple (concomitant) therapy for eradication of Helicobacter pylori. Pattern of main resistance of Helicobacter pylori to metronidazole or clarithromycin within the United States. The recurrence of Helicobacter pylori infection: incidence and variables influencing it. Proton pump inhibitor, clarithromycin and either amoxycillin or nitroimidazole: a metaanalysis of eradication of Helicobacter pylori. Sonnenberg proposed a birth-cohort effect to clarify the peaks in the incidence of, and mortality from, peptic ulcers. Hp infection acquired throughout childhood or adolescence turned manifested as peptic illnesses in later years. As Hp an infection gradually declined within the population over time, the prevalence of an infection also gradually shifted from a youthful towards older age groups. These lesions are referred to as "peptic" as a end result of the enzyme pepsin, proteolytic at an acidic pH (see Chapter 51), plays a major role in causing the mucosal breaks, regardless of the inciting agent. The percentages shown are tough approximations primarily based on research from Western international locations. Hp Infection the prevalence of Hp infection varies widely amongst nations in the world (see Chapter 52). In collection reported between 2009 and 2011, the prevalence of infection ranged from 7% to 87%, depending on the strategies of prognosis and the population that was sampled. Sanchez-Delgado and colleagues compiled 71 research containing 8496 sufferers with bleeding peptic ulcers and found an Hp infection fee of 72%. The use of an Hp diagnostic take a look at after the index bleed was associated with high Hp prevalence. The increased acid output from the stomach leads to increased acid load to the duodenum that can result in gastric metaplasia in the duodenal bulb. Neutrophil adherence liberates oxygen-free radicals, releases proteases, and obstructs capillary blood move. Gastric acid plays a secondary however necessary position by turning superficial mucosal lesions into deeper damage, interfering with platelet aggregation, and impairing ulcer therapeutic. Among Hp-infected sufferers with recent ulcer bleeding who continued to take lowdose aspirin, profitable eradication of Hp infection resulted in a really low risk of recurrent ulcer bleeding, similar to that seen with aspirin/omeprazole co-therapy. In a long-term prospective cohort research,28 Hp-infected low-dose aspirin users (160 mg/day) with bleeding ulcers who resumed their aspirin had a low threat of recurrent ulcer bleeding after eradication of Hp, a threat that was not considerably completely different from the danger in new aspirin customers with no history of ulcer disease (<1 bleed per one hundred patientyears). Hp an infection (past or present) had been at high danger of recurrent ulcer bleeding with continued enteric-coated aspirin remedy (>5 bleeds per a hundred patient-years). Other Causes of Ulcers and Idiopathic Ulcers Deep ulcers and perforations of the stomach and duodenum have been described in cocaine and methamphetamine users, presumably due to mucosal ischemia. Rarer causes of peptic ulcers include eosinophilic gastroenteritis, viral infections With a global decline in the prevalence of Hp infection, the proportion of patients with idiopathic ulcers has been increasing. It has been argued that solely the relative proportion, but not the true incidence, of idiopathic ulcers has elevated on account of a falling incidence of Hp ulcers. However, there are prospective data showing that the absolute incidence of idiopathic bleeding ulcers has elevated by 4-fold. Importantly, patients with a historical past of idiopathic bleeding ulcers have a 4-fold elevated danger of recurrent ulcer bleeding and more than 2-fold improve in mortality compared to sufferers with historical past of Hp ulcers. Pain is usually related to starvation, happens at night time, and is commonly relieved by meals and antacids. Often sufferers complain of dyspeptic symptoms such as a bloated sensation and fullness. Some sufferers complain of heartburn which will or is in all probability not accompanied by erosive esophagitis. Nevertheless, endoscopy is dear and has the potential for problems (see Chapter 42). A small proportion of sufferers with Hp-related useful dyspepsia would also enhance of their signs. These trials differed in how Hp was identified, and the upper age cutoff various from forty five to 55 years.
Cheap 800mg viagra vigour overnight deliveryHistologically, they reveal finger-like projections of connective tissue lined by an increased variety of squamous cells. The endoscopic differential prognosis contains glycogenic acanthosis, verrucous border of squamous cell carcinoma, and verrucous carcinoma. Malignant transformation has been reported in a couple of cases with multiple papillomas (esophageal papillomatosis), however cancer is rare in isolated lesions. Although dermatologic, ocular, and musculoskeletal manifestations dominate the scientific picture, esophageal papillomatosis may be present. Melanocytosis on the basal layer of the epithelium caused by basal hyperplasia or persistent esophagitis is assumed to play an necessary position in its pathogenesis. However, due to the gentle nature of the tumor, symptoms could be delayed, and the dimensions of the tumor at presentation is larger than 2 cm in over 90% of circumstances. They typically current after the age of 40 and symptoms can include dysphagia, bleeding from ulceration, dyspepsia, and weight loss. Although adenocarcinoma is a much more regularly acknowledged lesion associated with Barrett, several instances of adenomas have additionally been reported. Histopathology exhibits dysplastic tubular glands coated by specialized intestinal epithelium. Similar to colonic adenomas, these are thought of to be pre-malignant, and endoscopic resection is recommended for prognosis and treatment. Inflammatory Fibroid Polyp Inflammatory fibroid polyp (also generally identified as inflammatory pseudopolyp or eosinophilic granuloma) is characterised by a definite histology. This includes a submucosal-based polypoid lesion with perivascular, concentric fibroblastic proliferation with an increase in eosinophils. They most often are discovered incidentally in the abdomen and enormous intestines, followed by the small gut. Endoscopically, the few circumstances which are reported describe a spread of findings including submucosal nodules, plenty, ulcerations, and polypoid lesions. The 2 commonest cancers to metastasize to the esophagus are melanoma and breast cancer. Typically, metastatic lesions trigger extrinsic compression, with dysphagia a common symptom. Leiomyosarcomas are the most common subtype and can be troublesome to distinguish from benign leiomyomas. Histologically, they encompass interlacing whorls of spindle cells with elevated mitoses and marked pleomorphism. The endoscopic appearance, location throughout the esophagus, and number of lesions is variable. They are mostly found incidentally on higher endoscopy, as a result of most sufferers are asymptomatic. They may have a neural crest origin, as evidenced by immunohistochemical expression of S-100 protein. Although a couple of cases of malignant transformation are reported, the vast majority of cases are benign. They are almost solely seen in the cervical esophagus, likely because of the relatively free submucosal tissue and redundant mucosa on this anatomic region. Although most instances are diagnosed by the way, large polyps have been described to cause dysphagia and globus sensation. Peculiarly, prolapse of fibrovascular polyps out of the mouth has been described as fleshy tissue seen after vomiting or retching. Rarely, these polyps could cause fatal asphyxiation, and thus endoscopic or surgical removing is recommended. Lipomas are more generally discovered within the colon, small intestine, and abdomen than within the esophagus. Almost all are asymptomatic and found incidentally on endoscopy as barely yellowish, raised nodules within the proximal esophagus. Often, esophageal lipomas exhibit the "pillow" sign-indentation or cushioning with "palpation. They are typically pedunculated polyps that may cause symptoms similar to fibrovascular polyps. However, hamartomatous polyps are much less common and have a unique histologic appearance. They usually include multiple tissue sorts, including cartilage, bone, adipose tissue, smooth muscle, and skeletal muscle. Socioeconomic status and esophageal squamous cell carcinoma risk in Kashmir, India. A case-control examine of component levels and most cancers of the higher aerodigestive tract. Association of esophageal cytological abnormalities with vitamin and lipotrope deficiencies in populations at risk for esophageal cancer. The randomized Linxian Dysplasia Nutrition Intervention Trial after 26 years of follow-up: no impact of multivitamin supplementation on mortality. Prospective research of serum selenium levels and incident esophageal and gastric cancers. Prospective examine of serum selenium concentrations and esophageal and gastric cardia most cancers, heart illness, stroke, and whole demise. Dietary zinc deficiency fuels esophageal most cancers improvement by inducing a definite inflammatory signature. Total and most cancers mortality after supplementation with vitamins and minerals: follow-up of the Linxian common inhabitants nutrition intervention trial. High-temperature drinks and meals and esophageal cancer risk�a systematic evaluation. Nitrosamine and related food consumption and gastric and oesophageal cancer threat: a scientific review of the epidemiological evidence. Sphingolipids as biomarkers of fumonisin exposure and danger of esophageal squamous cell carcinoma in China. Human papillomavirus an infection and esophageal squamous cell carcinoma: a case-control research. Risk of esophageal adenocarcinoma in achalasia patients, a retrospective cohort study in Sweden. Regional variations in esophageal cancer charges by census area within the United States, 1999-2008. Associations of period, depth, and quantity of smoking with adenocarcinoma and squamous cell carcinoma of the esophagus. Alcohol consumption and the dangers of adenocarcinoma and squamous cell carcinoma of the esophagus.

Buy viagra vigour with visaEffect of gastrointestinal manifestations on quality of life in 87 consecutive patients with systemic sclerosis. Malnutrition is common in systemic sclerosis: outcomes from the Canadian scleroderma Research group Database. Muscarinic-3-acetylcholine receptor autoantibody in patients with systemic sclerosis: contribution to severe gastrointestinal tract dysmotility. Characteristics of patients with early systemic sclerosis and extreme gastrointestinal tract involvement. Esophageal motor abnormalities in sufferers with scleroderma: heterogeneity, threat elements, and effects on high quality of life. Loss of peristaltic reserve, decided by multiple rapid swallows, is the most frequent esophageal motility abnormality in patients with systemic sclerosis. Regional esophageal dysfunction in scleroderma and achalasia using multichannel intraluminal impedance and manometry. Distensibility of the anal canal in sufferers with systemic sclerosis: a research with the functional lumen imaging probe. Anorectal motility and sensation abnormalities and its correlation with anorectal signs in patients with systemic sclerosis: a preliminary study. Gastrointestinal involvement in systemic lupus erythematosus: perception into pathogenesis, analysis and therapy. Differences in illness features between childhood-onset and adult-onset systemic lupus erythematosus sufferers presenting with acute stomach ache. Reversible acute gastrointestinal syndrome associated with lively systemic lupus erythematosus in sufferers admitted to hospital. Acute belly pain in systemic lupus erythematosus: focus on lupus enteritis (gastrointestinal vasculitis). Ischemic colitis following colonoscopy in a systemic lupus erythematosus patient: report of a case. Opportunistic infections mimicking gastrointestinal vasculitis in systemic lupus erythematosus. The clinical traits of lupus related protein-losing enteropathy in Hong Kong Chinese inhabitants: 10 years of experience from a regional hospital. Systemic lupus erythematosus difficult with protein-losing enteropathy: a case report and evaluate of published works. Increased danger of systemic lupus erythematosus in 29,000 sufferers with biopsy-verified celiac disease. Systemic lupus erythematosus sophisticated by cytomegalovirus-induced hemophagocytic syndrome and colitis. Gastroesophageal reflux incites interstitial lung disease in systemic sclerosis: medical, radiologic, histopathologic, and therapy evidence. Management of gastrointestinal manifestations in systemic sclerosis (scleroderma). Does long term remedy with lansoprazole gradual progression of oesophageal involvement in systemic sclerosis Comparison of surgical approaches to recalcitrant gastroesophageal reflux disease within the patient with scleroderma. Gastrointestinal manifestation of systemic sclerosis-thickening of the upper gastrointestinal wall detected by endoscopic ultrasonography is a sound sign. Systemic evaluation: pathophysiology and administration of gastrointestinal dysmotility in systemic sclerosis (scleroderma). Gastro-intestinal permeability is elevated in sufferers with restricted systemic sclerosis. Outcome of small-bowel motor impairment in systemic sclerosis-a prospective manometric 5-yr follow-up. Intestinal pseudo-obstruction attributable to neuromyopathy in a affected person with systemic sclerosis. Lower gastrointestinal signs and high quality of life in sufferers with systemic sclerosis: a population-based study. Risk factors of mortality for salmonella an infection in systemic lupus erythematosus. Pneumatosis cystoides intestinalis and benign pneumoperitoneum in a affected person with antinuclear antibody adverse systemic lupus erythematosus. Intestinal pseudo-obstruction in systemic lupus erythematosus: an unusual however essential clinical manifestation. Systemic lupus erythematosus as a trigger and prognostic factor of acute pancreatitis. Pancreatitis in systemic lupus erythematosus: frequency and related factors-a evaluation of the Hopkins lupus cohort. Peritonitis as the first manifestation at onset of childhood systemic lupus erythematosus. Prevalence of active hepatitis C virus infection in patients with systemic lupus erythematosus. Epidemiological features of Budd-Chiari in Egyptian patients: a single-center study. Serum alanine aminotransferase elevations correlate with serum creatine phosphokinase levels in myositis. Myopathy together with polymyositis: a likely class antagonistic effect of proton pump inhibitors Severe gastrointestinal irritation in grownup dermatomyositis: characterization of a novel scientific affiliation. Intravenous immunoglobulins for steroid-refractory esophageal involvement related to polymyositis and dermatomyositis: a collection of 73 sufferers. Esophageal involvement and interstitial lung illness in combined connective tissue disease. Radionuclide imaging for the evaluation of esophageal motility problems in combined connective tissue disease patients: relation to pulmonary impairment. Twenty-four hour intraesophageal pH monitoring in youngsters and adolescents with scleroderma and combined connective tissue illness. A case of blended connective tissue disease with cystic pancreatitis: successful remedy by cyclophosphamide. A case of merged idiopathic portal hypertension in course of combined connective tissue illness. Gastrointestinal involvement in polyarteritis nodosa (1986�2000): presentation and outcomes in 24 patients. Enteropathic spondyloarthropathy: a typical genetic background with inflammatory bowel disease Esophageal motor operate in familial Mediterranean fever: a potential evaluation of motility in 31 sufferers. Ehlers-Danlos syndrome and gastrointestinal manifestations: a 20-year expertise at Mayo Clinic. Unexplained gastrointestinal symptoms and joint hypermobility: is connective tissue the missing link The utility of Tc-99m dextran within the analysis and identification of melanoma metastases liable for protein-losing enteropathy. Surgery for melanoma metastases of the gastrointestinal tract: indications and outcomes.
References - Vale JA, Bowsher WG, Liu K, et al: Post-irradiation bladder dysfunction: development of a rat model, Urol Res 21(6):383n388, 1993.
- Danisi G, Straub RW: Unidirectional influx of phosphate across the mucosal membrane of rabbit small intestine, Pflugers Arch 385:117n122, 1980.
- Edelstein D, Dobs A, Basaria S: Emerging drugs for hypogonadism, Expert Opin Emerg Drugs 11:685n707, 2006.
|
|