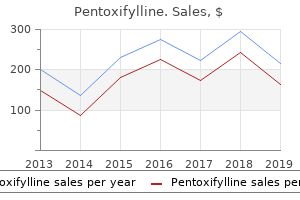
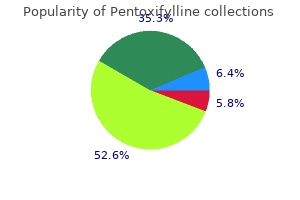
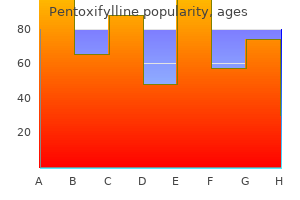
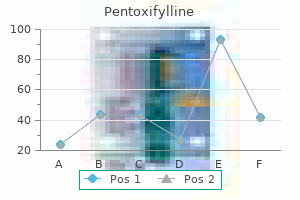
"Buy pentoxifylline with a mastercard, joint arthritis medication for dogs."By: Danielle Marie Brander, MD - Assistant Professor of Medicine
- Member of the Duke Cancer Institute
 https://medicine.duke.edu/faculty/danielle-marie-brander-md
Purchase 400mg pentoxifylline amexClinical Presentation Lung most cancers is the leading cause of cancer-related demise worldwide for men and ladies. Lung cancer accounts for under 13% of new cancer instances however accounts for almost one third of cancer-related deaths. Even accounting for the roughly one third of patients recognized at an early stage, the speed of 5-year survival for all patients with lung most cancers is less than 20% general. Carcinoid tumors and other neuroendocrine tumors are much less frequent, and adenoid cystic carcinomas are uncommon. Owing to differences in biology and the efficacy of therapeutic brokers, the histologic classification of non�small cell lung cancer is now of important importance when contemplating a therapeutic approach. The location of tumors and the appearance of paraneoplastic syndromes decide the clinical presentation of most sufferers with lung cancer (Table 1). Centrally located tumors will typically trigger signs associated with local results of the tumor such as cough, hemoptysis, wheezing, or stridor. Mediastinal lymph node involvement may cause disruption of the recurrent laryngeal nerve, leading to hoarseness. Tumors arising within the superior sulcus, so-called Pancoast tumors, can lead to a lower brachial plexopathy and Horner syndrome. Peripheral tumors are likely to current later as ache when involving the chest wall or pleura. It is extremely rare in people underneath the age of 30, and the incidence decreases above age eighty five. Prior to the Sixties, lung cancer was uncommon amongst women; nonetheless, the current price is almost equal between women and men. The incidence is decreasing amongst men and has leveled off in ladies over the previous decade. Current smokers with a larger than 20-pack-year smoking historical past have a 2000-fold greater threat of developing lung most cancers compared with nonsmokers. Symptoms such as seizures, nausea and vomiting, headache, and focal neurologic signs may be the initial presentation of such sufferers. Bony metastases are frequent in all kinds of lung cancer and can present with pain, pathologic fracture, or spinal twine compression. Lung cancers are notable for ectopic manufacturing of hormones leading to several paraneoplastic syndromes. This leads to release of calcium from bones and elevation of calcium within the blood. Screening 844 Since the overwhelming majority of sufferers present with lung cancer with advanced illness and curative approaches are limited to patients with limited disease, screening at-risk patients for lung most cancers has been undertaken to identify patients with early-stage disease to stop excess mortality from lung cancer. Ninety-five percent of constructive scans have been later decided to be false positives by biopsies or long-term follow-up of nodules. It is now extensively really helpful to incorporate lung most cancers screening in patients with a heavy smoking history; however, selections concerning administration of positive screening scans need to be managed in a multidisciplinary fashion to keep away from unnecessary diagnostic procedures. Once the analysis is confirmed, accurate staging of illness is essential to determine the prognosis and acceptable remedy. All patients ought to be evaluated with baseline bloodwork to embody a complete blood count, liver perform exams, and evaluation of renal operate. The major mode of remedy for these sufferers is surgical resection, which ends up in 5-year survival of roughly 70%. Wherever attainable, lobectomy with full mediastinal lymph node dissection is recommended for correct pathologic staging. Occasionally, pneumonectomy is required based mostly on the placement of the first tumor; nevertheless, the morbidity and mortality of this process are much higher than lobectomy. Video-assisted thoracoscopic approaches are desirable every time possible and lead to decrease surgical morbidity. Surgical resection is in all probability not feasible for all patients, notably those with poor pulmonary function or performance status. Several studies have evaluated the role of adjuvant chemotherapy in this group of patients; however, no clear survival profit has emerged. Several strategies can be used to obtain tissue depending on the placement of the tumor. For patients presenting with pleural effusion, cytologic examination of pleural fluid can establish the prognosis. The alternative of technique for diagnosis should be individualized in accordance with the assets which are available on the treating institution. A survival benefit was solely demonstrated in patients with tumors higher than four cm. In cases during which the surgical margins are positive, adjuvant radiation remedy is routinely beneficial; nonetheless, that is infrequent. Again, lobectomy using a minimally invasive video-assisted thoracoscopic method is most well-liked every time potential. While the overall prognosis of this group of sufferers is poor, treatment with healing intent leads to longterm survival of 10% to 30%. Recurrence charges and progression-free survival were rather more favorable for the surgical procedure arm. Much of the surplus mortality within the surgical procedure arm was for those sufferers requiring a pneumonectomy for complete resection. Finally, 46% of sufferers had been downstaged by induction chemotherapy to have N0 illness at the time of resection. Among those patients, the 5-year survival was 40%, suggesting that good response to induction chemoradiotherapy may predict a benefit to surgical resection. In these patients, radiation therapy to the mediastinum is usually provided either in combination with or sequential to adjuvant chemotherapy. The use of induction chemotherapy adopted by chemoradiation has been evaluated, as has the utilization of consolidation chemotherapy; however, no regimen has clearly confirmed to be superior. For patients with poor efficiency status, using sequential chemotherapy followed by radiation might be preferred, or for those deemed unfit for chemotherapy, palliative radiation could be probably the most applicable therapy. Thus identification of those sufferers with molecular testing is now the usual of care to determine probably the most acceptable first-line remedy for patients with lung adenocarcinoma. If any of those mutations are current, then sufferers should be treated with a molecularly focused agent. For adenocarcinoma, platinum doublet with either pemetrexed � bevacizumab (Avastin) could be offered, however neither of those is efficient for squamous cell tumors. Second-line treatment ends in a survival benefit and subsequently ought to be offered to sufferers with acceptable functional status. Pembrolizumab was related to an improved general survival and improved quality of life in contrast with chemotherapy, with roughly 20% of sufferers handled experiencing a prolonged illness remission of greater than 2 years. While each carboplatin1/pemetrexed and carboplatin1/paclitaxel/bevacizumab regimens are acceptable decisions for adenocarcinoma, the tolerability of carboplatin/pemetrexed makes this the popular regimen for most patients with metastatic adenocarcinoma with no molecular driver mutation.
Order pentoxifylline 400 mg onlineI scapularis is the vector for Anaplasma phagocytophilum within the northeastern and midwestern United States, whereas the western blacklegged tick, Ixodes pacificus, is the principal vector along the West Coast. The seasonality is bimodal, with the first peak June�July and a smaller peak in October, corresponding to the emergence of the adult stage of I scapularis. I scapularis additionally transits Borrelia burgdorferi (Lyme disease), Babesia microti (babesiosis), Borrelia miyamotoi (tickborne relapsing fever), and deer tick virus (a explanation for tickborne encephalitis). Simultaneous infections with A phagocytophilum and B burgdorferi or B microti have occurred. A phagocytophilum is discovered predominantly in neutrophils in the peripheral blood and tissues from contaminated individuals. A phagocytophilum has the distinctive ability to selectively survive and multiply inside cytoplasmic vacuoles (morulae) of polymorphonuclear cells by delaying their apoptosis. Infection with A phagocytophilum induces a systemic inflammatory response, which is believed to be the mechanism for tissue harm. Pathologic findings with human granulocytic anaplasmosis include normocellular or hypercellular bone marrow, erythrophagocytosis, hepatic apoptosis, focal splenic necrosis, and delicate interstitial pneumonitis and pulmonary hemorrhage. Clinical Manifestations 628 A detailed history ought to include information about known tick bites or actions that might be associated with tick publicity. Absence of a tick chunk should by no means dissuade suppliers from contemplating tickborne rickettsial illness within the applicable scientific context. Contact with pets, especially canine, and a historical past of tick attachment or current tick removal from pets could be helpful in assessing human tick exposure. Tickborne rickettsial illnesses commonly have nonspecific medical signs and symptoms early in the midst of illness. The incubation period is generally shorter (5 days) in sufferers who develop severe disease. Initial symptoms are often nonspecific and embody the sudden onset of fever, chills, malaise, and myalgia. A rash usually happens 2 to 4 days after the onset of fever; however, many patients initially seek medical care before the rash. The rash usually begins as small, blanching macules on the ankles, wrists, or forearms that then spreads to the palms, soles, arms, legs, and trunk, often sparing the face. The generalized petechial rash seems later (day 5 or 6) and is indicative of superior disease. In addition to rash, the most frequent clinical findings at any level in the sickness are fever (99%), headache (91%), and myalgia (82%). Symptoms develop a median of 5 days (range, 2�10 days) after the bite of an infected tick. The first manifestation in almost all sufferers is an inoculation eschar, which usually is nonpruritic, nontender or mildly tender, and surrounded by an indurated, erythematous halo and occasionally a couple of petechiae. The rash primarily involves the extremities and trunk and in $half of sufferers entails the palms and soles. Laboratory findings embrace modest elevation of hepatic transaminases (78%), mild leukopenia (50%), and thrombocytopenia (40%). Few patients with Rickettsia species 364D have been reported, so the complete scientific spectrum has but to be described. It does appear to be comparatively delicate and characterized by an eschar or ulcerative pores and skin lesion with regional lymphadenopathy. Symptoms of E chaffeensis ehrlichiosis usually occur a median of 9 days (range, 5�15 days) after an infected tick chew. Rash (maculopapular, petechial, or diffuse erythema) occurs in roughly one-third of sufferers and is extra frequent in kids. The rash happens a median of 5 days after illness onset and can contain the palms and soles. Characteristic laboratory findings in the first week include leukopenia, thrombocytopenia, and elevated ranges of hepatic transaminases. Ehrlichia ewingii and Ehrlichia muris-like agent ehrlichiosis have comparable clinical and laboratory features as E chaffeensis ehrlichiosis, though rash and gastrointestinal signs are much less frequent. Symptoms of human granulocytic anaplasmosis usually happen 5 to 14 days after an contaminated tick chunk. Rash is current in <10% of patients, and central nervous system involvement is rare. Confirmatory diagnostic exams are serologic assays, nucleic acid detection, immunostaining of biopsy tissue, blood-smear microscopy, and culture. Assays using paired acute and convalescent sera (ideally collected 2�4 weeks apart) are the standard for serologic confirmation. Obtaining blood earlier than treatment is really helpful to lower false-negative outcomes. Differential Diagnosis the differential analysis of fever and rash is broad, and during the early levels of illness tickborne rickettsial ailments may be indistinguishable from many viral exanthams, particularly in kids. In addition to viral infections, circumstances that ought to be considered embody meningococcemia, Kawasaki illness, secondary syphilis, disseminated gonococcal an infection, bacterial endocarditis, scarlet fever, leptospirosis, typhoid, drug eruptions, Stevens-Johnson syndrome, toxic shock syndrome, and thrombotic thrombocytopenic purpura. Doxycycline is the drug of choice for therapy of all tickborne rickettsial diseases in sufferers of all ages and ought to be initiated immediately in individuals with signs and symptoms suggestive of rickettsial disease. Because of the nonspecific signs and signs of tickborne rickettsial diseases, concomitant empiric treatment for other situations within the differential analysis must be administered. The use of doxycycline to treat children with suspected tickborne rickettsial illness should no longer be a subject of controversy. Rifamycins show in vitro activity against E chaffeensis and A phagocytophilum. Case reports document favorable outcomes in small numbers of pregnant ladies treated with rifampin for anaplasmosis. Monitoring and Complications Treatment Fever with tickborne rickettsial diseases typically subsides within 24 to 48 hours when treated with doxycycline in the first four to 5 days of illness. Severely ill sufferers could require >48 hours of remedy earlier than clinical enchancment is famous. Patients with proof of organ dysfunction, extreme thrombocytopenia, psychological status modifications, or the necessity for supportive therapy ought to be hospitalized. Predictors of a more extreme course of anaplasmosis embody superior age, immunosuppression, comorbid medical circumstances, and delay in diagnosis and therapy. Confirmed A phagocytophilum coinfection has been reported in <10% of sufferers with Lyme disease. Response to remedy can present clues to possible coinfection with Lyme illness or babesiosis. If the clinical response to treatment with doxycycline is delayed, coinfection or an alternate an infection should be considered. Conversely, if Lyme illness is treated with a betalactam antibiotic in a affected person with unrecognized A phagocytophilum infection symptoms may persist. Longer periods of tick attachment enhance the probability of transmission of tickborne diseases. Those caused by toxin-producing strains of Staphylococcus aureus and Streptococcus pyogenes produce an acute, desquamative febrile illness.
Syndromes - Optic neuritis
- Drug reaction
- Prostate cancer
- A chromosome defect
- Chlorprothixene (Taractan)
- Pancreatitis
- Paralysis
- Chemical peels or topical steroid creams
- Injury from gallbladder surgery
Buy pentoxifylline with a mastercardHowever, these recommendations are based mostly on inhabitants information and must be tailored to individual patient needs, circumstances, and responsiveness to therapy. All sufferers with bronchial asthma ought to have an action plan that describes their pharmacologic self-management. Aspects of pharmacologic self-management embody the maintenance medicine schedule, rescue therapy doses for elevated signs, when and the way to enhance controller treatment remedy, when and tips on how to use prednisone, the way to recognize a extreme exacerbation, Asthma in Adolescents and Adults and when and the means to search pressing or emergency care. Controller medications should be increased with an higher respiratory an infection or with signs requiring greater than two doses of rescue remedy in 12 hours. The increased dose of controller drugs ought to be maintained no much less than until increased symptoms resolve. Prednisone is often needed for patients with incomplete or short-term responses to adequate doses of -agonists (4 puffs with a spacer, waiting at least 1 minute between puffs), substantial interference with sleep each evening, requirement for 12 or extra puffs of -agonist in a 24-hour interval, or a peak move less than 60% predicted. Persistent bronchial asthma is most effectively managed with daily long-term control medications, particularly antiinflammatory remedy. For sufferers with very poorly managed bronchial asthma, think about growing by two steps, a course of oral corticosteroids, or each. Before increasing pharmacologic remedy, contemplate adverse environmental exposures, poor adherence, poor inhaler technique, or comorbidities as targets for intervention. For patients with troublesome or debilitating unwanted effects from asthma therapy, explore a change in therapy. Differences in potencies exist, but all products are primarily comparable on a per-puff foundation. For levalbuterol, ought to prime the inhaler by releasing four actuations previous to use. Evidence is lacking for ipratropium producing additional benefit to 2 agonists in long-term management asthma remedy. Short programs (bursts) are efficient for establishing management when initiating therapy or throughout a interval of gradual deterioration. Fluticasone and salmeterol (AirDuo and generic) Budesonide and formoterol (Symbicort) Mometasone and formoterol (Dulera) Fluticasone furoate/ vilanterol trifenatate (Breo Elipta) 1 inhalation bid 2 inhalations bid 80/4. For zafirlukast: Administration with meals decreases bioavailability; take no less than 1 h earlier than or 2 h after meals. Zafirlukast is a microsomal p450 enzyme inhibitor that may inhibit the metabolism of warfarin. Zileuton is a microsomal p450 enzyme inhibitor that can inhibit the metabolism of warfarin and theophylline. Due to extensive interpatient variability in theophylline metabolic clearance, routine serum theophylline level monitoring is important. Various factors (diet, food, febrile illness, age, smoking, and different medications) can have an effect on serum concentration. Monitor affected person following injections; be ready and geared up to indentify and deal with anaphylaxis which will happen. Whether patients will develop vital antibody titers to the drug with long-term administration is unknown. For 12 years and older with eosinophilic bronchial asthma Benralizumab (Fasenra) Mepolizumab (Nucala) Subcutaneous powder for solution: one hundred mg Intraveneous answer 10 mg/ 1 mL For 12 years and older with eosinophilic asthma Monitor patient following injections; be prepared and outfitted to identify and treat anaphylaxis which will happen. Such assessments must be made in patients presenting with extreme exacerbations after the preliminary bronchodilator remedy and in all sufferers after three doses of bronchodilator therapy (60� 90 min after preliminary treatment). Intubation and mechanical ventilation may be required for patients with respiratory failure regardless of therapy. I hope that the method described herein for assessing and managing bronchial asthma will help physicians help their sufferers achieve well-controlled asthma. Although atelectasis is considered a benign condition, early therapy, reversal, and prevention are important to an overall improved end result. Emergency Department and Hospital Management Assessment should rapidly decide the severity of the exacerbation primarily based on intensity of signs, indicators (heart price, respiratory price, use of accent muscles, chest auscultation), peak circulate (unless the affected person is just too dyspneic to perform), and pulse oximetry. Treatment ought to begin immediately following recognition of an exacerbation extreme enough to trigger dyspnea at relaxation, peak move lower than 70% predicted or private best, or pulse oximetry oxygen saturation lower than 95%. While therapy is being given, a short, focused history and physical examination pertinent to the exacerbation may be obtained. When this response is sustained a minimum of 60 minutes after the final therapy, the affected person may normally be discharged on a course of oral corticosteroids (generally prednisone 40�60 mg for 5�10 days), initiation or continuation of medium-dose inhaled corticosteroids, and association for outpatient follow-up. Summary Asthma is a very common downside with the potential to cause substantial interference with quality of life. Surfactant Impairment Surfactant serves to scale back the alveolar floor pressure, thereby stabilizing the alveoli and preventing collapse. Gas Resorption One mechanism by which gasoline resorption results in atelectasis involves the patent airway. With regard to lung reexpansion, incentive spirometry, continuous or intermittent positive-pressure ventilation, and early ambulation may be used. Additionally, applicable ache administration in the postoperative setting allows for proper ventilation. The pure course of atelectasis may lead to fever, cough, tachypnea, wheezing, rhonchi, and chest ache. On physical examination, atelectasis may manifest as an space of localized decreased breath sounds with constant wheeze or lowered chest wall growth or each. Direct signs embody: � Displaced pulmonary vessels � Air bronchograms � Displacement of intralobar fissures (most reliable sign) Indirect signs embody: � Pulmonary opacification � Diaphragmatic elevation � Hyperexpansion of unaffected lung � Tracheal, coronary heart, and mediastinal shift towards atelectatic side � Shift of the hilum towards the collapsed lobe � Segmental ipsilateral rib approximation Treatment Treatment of atelectasis is geared toward the underlying cause. It is necessary to acknowledge respiratory distress and to intubate the affected person if applicable. In the supine place, the pleural pressures increase to the best extent within the dependent lung areas and might compress the adjacent lung tissue. Studies have shown that hyperinflation via increased tidal volume, sequential air inflations to the entire lung capacity, or even a single cycle of increased tidal quantity can enhance the release of surfactant, aiding in recruitment and stabilization of alveoli. Another mechanism by which fuel resorption leads to atelectasis happens after complete airway occlusion. The gases which would possibly be trapped are absorbed by the blood perfusing through that region of the lung, which ultimately causes collapse of the alveoli. The atelectasis produces alveolar hypoxia and pulmonary vasoconstriction to prevent V =Q mismatching and to minimize arterial hypoxia. Pneumonia often presents with shortness of breath, fever, productive cough, with leukocytosis and radiographic findings of lobar infiltrate. Diagnosis and treatment must be primarily based on underlying traits of the patient and their risk elements. Epidemiology Etiology Risk Factors Predisposing factors for improvement of pneumonia embody a quantity of prescription medicines (angiotensin-converting enzyme inhibitors, antipsychotic drugs, glucocorticoids, H2 blockers, proton pump inhibitors, and sedatives), tobacco use, alcohol use, malnutrition, use of dentures at night time, bronchial obstruction due to overseas physique, altered mental status because of reversible causes, and pulmonary edema. In the United States, however, rates of streptococcal pneumonia have declined after implementation of the pneumococcal vaccine in each adults and youngsters.
Purchase 400 mg pentoxifylline visaTreatment usually consists of low dose cyclosporine1, methotrexate1 or cyclophosphamide (Cytoxan)1. There can additionally be proof that such sufferers have T-cell or monocyte-mediated myelosuppression, probably via the elaboration of varied cytokines. Flow cytometry of peripheral blood reveals a predominance of lymphocytes, however sometimes, these are polyclonal. Autoimmune neutropenia in the absence of an outlined rheumatologic problems can also occur, and is often gentle. Indications for remedy embody an absolute neutrophil count lower than 500/mm3 in addition to constitutional signs similar to fever or infection. Such patients typically respond to corticosteroids or intravenous gamma globulin (Gamunex)1. Autoimmune neutropenia is almost exclusively seen in children between the ages of 6 and 12 months. The situation is usually self-limiting, with most sufferers recovering after a quantity of years. Affected children may have very low neutrophil counts, ranging between 0�150/mm3, and with lots of the sufferers are under 2 years of age. The prognosis is usually one of exclusion, although testing for antineutrophil antibodies may be performed in search of antibodies in opposition to the above epitopes, noting the previously talked about caveats. Treatment consists of supportive care with prophylactic antibiotics as applicable. Paroxysmal nocturnal hemoglobinuria is a rare, acquired disorder, greatest grouped beneath bone marrow failure syndromes, in which affected people display a selection of symptoms, including cytopenias, abnormal blood clotting, and hemoglobinuria. Patients could experience periods of relatively regular well being and blood counts, but a substantial proportion of sufferers go on to develop aplasia or myelodysplasia. Treatments included supportive care, anticoagulation for sufferers with thrombosis, and the complement inhibitor Eculizumab (Soliris). Chronic Idiopathic Neutropenia Rarely grownup sufferers present with persistent neutropenia with no specific etiology discovered. As part of the presentation, other cell line numbers, corresponding to pink cells and platelets, should be regular. Splenic Enlargement/Sequestration Splenic enlargement outcomes from intrinsic splenic disease corresponding to glycogen. Usually the neutropenia is mild to average, and infrequently patients have accompanying gentle anemia and thrombocytopenia. Splenectomy ought to be reserved for very select cases, due to its associated subsequent prolonged increased threat of an infection and thrombosis. Collectively these issues have a very low incidence of round 6/1,000,000 youngsters. The analysis is usually made by having a patient bear serial blood counts over a number of weeks to months. On the other hand, cyclic neutropenia is defined as neutropenia recurring roughly every 2 to 5 weeks and lasting three to 6 days. Although patterns range from affected person to affected person, they tend to be internally constant for a given patient. Kostmann syndrome, first recognized in 1950, is an autosomal recessive dysfunction characterized by profound neutropenia, neurological manifestations, and a robust propensity to develop life threatening bacterial and fungal infections. Unfortunately, affected kids have an increased danger of growing acute myelogenous leukemia and myeloma dysplastic syndromes. Affected patients present with profound neutropenia, and the etiology appears to be the impaired launch of neutrophils from the bone marrow compartment. Patients also show decreased numbers of B cells and a propensity for infections with human papilloma virus, which can be refractory to therapy. Studies are underneath way to consider if the stem cell�mobilizing agent plerixafor (Mozobil)1 may be of profit in these patients. Chediak Higashi syndrome, one other uncommon autosomal dominant disorder, is characterized by oculocutaneous albinism, bleeding diathesis, neuropathy, and recurrent infections. A hallmark of this dysfunction are abnormally large azurophilic granules in neutrophils that are most likely to be reduced in quantity. The solely remedy to cure this disorder is hematopoietic stem cell transplantation. Patients current in early adolescence with nail dystrophy, irregular skin pigmentation and leukoplakia, as nicely as pulmonary and hepatic findings. The treatment of choice is allogeneic bone marrow transplantation, but sufferers seem to have extra chemotherapy-related morbidity with this process. The pure history and prognosis of those vary significantly from indolent and slow-growing types (over many years) to highly aggressive (within weeks) sorts. Expert hematopathology review incorporating morphologic, immunophenotypic, and genetic options is essential for an correct analysis. Infants and kids with persistent neutropenia, particularly if there are other noteworthy bodily signs and signs, should be referred to a pediatric hematologist or tutorial middle with experience in managing these disorders. Affected people present early in life with a wide selection of symptoms, including fever, hepatosplenomegaly, and variable cytopenias. The disease is extremely aware of treatment with a variety of therapy choices (remission charges exceeding 90% with mixed rituximab/chemotherapy), though the clinical course is characterized by repetitive relapses. The highest relative threat of creating a secondary malignancy occurs greater than 21 to 30 years after original diagnosis. Bucaneve G, Micozzi A, Menichetti F, et al: Levofloxacin to forestall bacterial infection in patients with cancer and neutropenia, N Engl J Med 353:977�987, 2005. Capsoni F, Piercarlo S-P, Zanella A: Primary and secondary neutropenia, Arthritis Res Ther 7(5):208�214, 2005. Affected people present with neutrophils counts <1000/mm3 and typically are identified in infancy. These individuals also tend to have genitourinary malformations and cardiac abnormalities. The disorder is uniformly deadly with out remedy, which generally consists of the agent etoposide (Toposar)1 and maintenance remedy with cyclosporine (Neoral)1. Andersohn F, Konzen C, Garbe E: Systematic evaluate: agranulocytosis induced by nonchemotherapy medication, Ann Intern Med 146:657�665, 2007. Dale O, Bolyard A: An replace on the prognosis and remedy of continual idiopathic neutropenia, Current Opin Hematol 24:46�53, 2017. Donadieu J, Fenneteau O, et al: Congenital neutropenia: diagnosis, molecular bases and affected person administration, Orphanet Journal of Rare Diseases 6:26; 1�28, 2011. References the time period malignant lymphoma was originally launched by Billroth in 1871 to describe neoplasms of lymphoid tissue. However, further components are likely liable for this sudden enhance in incidence. Etiology and Risk Factors Chromosomal Translocations and Molecular Rearrangements Nonrandom chromosomal and molecular rearrangements play an important position in the pathogenesis of many lymphomas and sometimes correlate with histology and immunophenotype. These chromosomal adjustments typically lead to oncogenic gene merchandise; for instance, t(11;14)(q13;q32) translocation results in overexpression of bcl-1 (cyclin D1) in mantle-cell lymphoma, while translocation with 8q24 leads to c-myc overexpression in practically all Burkitt lymphomas and in 10%�15% of sufferers with diffuse large B-cell lymphoma.
Buy pentoxifylline 400 mgIf a affected person has mild tics and few or no comorbid symptoms, medical therapy is probably not wanted. Some consultants suggest baseline electrocardiograms, significantly for people with private or household history of cardiac arrhythmias. Weight gain and metabolic syndrome must be thought of when starting neuroleptics, particularly risperidone (Risperdal)1 and aripiprazole (Abilify). Other Tic-Suppressing Medications Several small, managed studies show benefit for topiramate (Topamax),1 dopamine agonists,1 baclofen (Lioresal)1, benzodiazepines,1 and botulinum toxin type A (Botox)1 injections for focal, robust tics. In parallel, however, the getting older of the inhabitants has led to the broader use of antithrombotic drugs in addition to increases in the prevalence of amyloid angiopathy. By contrast, hemorrhages centered within the deep grey buildings of the basal ganglia, thalamus, and the mind stem come up most often as a complication of continual hypertension, with amyloid angiopathy playing no position. The explanation for this is likely the inexorable development of the underlying blood vessel disease, amyloid angiopathy. Nausea and vomiting could be prominent, particularly in sufferers with cerebellar hemorrhages in addition to those who quickly develop substantial mass effect or hydrocephalus. The historical past and laboratory analysis, summarized in Box 1, should be centered on figuring out potential contributing causes as well as targets for therapy. Some clinicians use prothrombin complex focus to reverse Factor Xa inhibitors. Severe thrombocytopenia or coagulation factor deficiency: Platelet and/or factor substitute. External ventricular drainage catheters: Consider for any patient with hydrocephalus or intraventricular hemorrhage. Emergent surgical clot removal: Indicated for cerebellar hemorrhage with brain stem compression or neurologic deterioration. Prevention of deep venous thrombosis: Intermittent pneumatic compression system and elastic stockings. It is subsequently essential to examine head imaging for skull fractures and the presence of subdural or subarachnoid hemorrhage, which might be traumatic in origin. After the focused analysis (see Box 1) is accomplished, emergency care is devoted to preventing neurologic deterioration (Box 3). Clinicians are suggested to provide care in accordance with the rules outlined on this chapter for all patients on the outset, and to defer selections to restrict aggressiveness of care for the first 24 hours. Invasive monitoring of intracranial pressure ought to be thought of in patients with evidence of shift of the intracranial contents on neuroimaging. The multidisciplinary administration of stroke could be improved with particular instructional packages aimed at growing consciousness of stroke within the common population and amongst professionals. The concept of time is mind has nice value in emphasizing that stroke is an emergency. In rural or distant areas with no stroke unit services, telemedicine has proved to be a valid different. After an ischemic stroke, blood pressure should be lowered even in patients with normal blood pressure. Hemphill, et al: Guidelines for the administration of spontaneous intracerebral hemorrhage, Stroke 2015. The administration of patients in stroke models and the demonstration of the efficacy of thrombolysis and thrombectomy have been crucial in this achievement. Improved management has included high-quality rehabilitation, which is started as soon as possible to improve the restoration. Because the window for the out there timedependent therapies could be very narrow, avoiding delay is the major aim in the prehospital section of acute stroke care. All stroke sufferers should be transported as soon as attainable to the closest hospital with a stroke unit. Factors that have to be Lifestyle modification is often a major contributor to reducing the chance of ischemic stroke. Strategies to achieve this protection embody avoiding smoking and extreme alcohol consumption, keeping a low�normal physique mass index, working towards common train, and having a diet low in salt and saturated fat, high in fruits and vegetables, and wealthy in fiber. Blood pressure must be managed with diet and pharmacologic remedy, aiming at regular ranges of 120/80 mm Hg. Diabetes ought to be managed with lifestyle modification and pharmacologic therapy as required, and blood stress needs to be extra tightly controlled in these patients (<130/80 mm Hg). After a noncardioembolic ischemic stroke, statins are helpful in all sufferers for secondary prevention. Ischemic Cerebrovascular Disease Postmenopausal hormone replacement remedy ought to be averted for the primary or secondary prevention of stroke because it can enhance the chance of latest vascular events. Antithrombotic Therapy Low-dose aspirin can be used for the first prevention of stroke in women or of myocardial infarction in men. Aspirin is useful for the prevention of stroke in sufferers with asymptomatic carotid stenosis. With a rating of 1, the decision must be made based on the presence of danger factors, risk of bleeding, and affected person choice. Dabigatran (150 mg bid) and apixaban (5 mg bid) have proven to be superior to warfarin in stroke prevention. The dose of the direct oral anticoagulants must be adjusted relying on age, renal operate, or weight. The handiest routine is clopidogrel (Plavix) or aspirin plus dipyridamole (Aggrenox). Anticoagulation is often indicated for secondary prevention if the stroke cause is cardioembolic and in particular conditions corresponding to aortic arch atheroma, fusiform aneurysms of the basilar artery, or patent foramen ovale in the presence of confirmed deep venous thrombosis. Surgery should be performed in facilities with a perioperative complication rate of less than 6% and as soon as potential after the final ischemic occasion. Endarterectomy could also be indicated for certain patients with moderate stenosis (50%�69%), although it ought to be performed only in centers with a perioperative complication price of lower than 3% to be efficient. In circumstances of symptomatic carotid lesions, angioplasty plus stenting is an inexpensive different, primarily in patients youthful than 70 years old. If stenting is performed, a mixture of clopidogrel and aspirin is required immediately earlier than the procedure and for no much less than 1 month to forestall stent thrombosis. In patients with intracranial atheromatosis and stroke recurrences, intensive medical remedy is the preferred option. Management of Carotid Stenosis Management of Acute Ischemic Stroke 688 All stroke patients ought to be treated in a stroke unit, as a outcome of this is related to a discount of demise, dependency, and the necessity for institutional care. This effect is seen for each type of patients, no matter gender, age, stroke subtype, and stroke severity. Patients with stroke should have a careful scientific assessment, including a neurologic examination. For the detection and early administration of the medical problems of stroke, neurologic standing, pulse, blood pressure, temperature, and oxygen saturation ought to be monitored.
Buy cheap pentoxifylline onlineMood issues and temper dysregulation are among the most common manifestations of human suffering. Mood Disorders* disorder), (b) with blended features, (c) with melancholic features, (d) with atypical options, (e) with psychotic options, (f) with catatonia, (g) with peripartum onset, and (h) with seasonal pattern. Epidemiology Risk Factors For unipolar major depressive problems, danger components embody gender (women at higher risk), age (18�44 years of age at larger risk), marital standing (separated and divorced at greater risk), household history (relatives with depression), early parental demise, life events (negative tense occasions, continual publicity to stress), low confidence, and concrete environments. In addition, for bipolar dysfunction, larger somewhat than decrease socioeconomic standing and suburban environments have been cited as risk components. Individuals with nervousness dysfunction, chronic publicity to stress and trauma, substance abuse, psychotic problems, and persistent medical conditions are all identified to be in danger for temper issues. Certain kinds of adversity, such as frequent childhood bullying, end in a high threat of poor social health and economic outcomes with an increase of suicidality, depression, anxiety disorders, and alcohol dependency, practically four decades after publicity. In addition, psychiatric symptoms which may be present in childhood constitute a danger issue for adult psychopathology, together with mood disorders. Anxiety/depression, labile affect, and manic signs are all predictors for future onset of bipolar spectrum dysfunction. Acute and transient psychotic dysfunction resulted in 28% onset of affective disorder, but solely 15% schizophrenia at 1-year follow-up. Depressive Disorder (Unipolar Mood Disorder) Major Depression the mainstay of major depressive dysfunction is a significant depressive episode. At least five or more of the next signs throughout the identical 2-week interval are required: (1) depressed temper most of the day, nearly every single day (sadness, feelings of vacancy, tearfulness); (2) marked diminished interest or pleasure in almost all actions; (3) vital weight loss or weight achieve or fluctuations in urge for food; (4) insomnia or hypersomnia; (5) psychomotor retardation or agitation practically every day; (6) fatigue or loss of power; (7) emotions of Persistent Depressive Disorder (Dysthymia) Persistent depressive disorder, the new designation for dysthymic dysfunction, is a continual type of despair during which the depressed temper has persisted for a minimum of 2 years (in kids for a minimum of 1 year), as manifested by at least two of the following signs: (1) poor urge for food or overeating, (2) insomnia or hypersomnia, (3) low power or fatigue, (4) low self-esteem, (5) poor focus or issue making choices, and (6) emotions of hopelessness. Persistent depressive dysfunction may also qualify for any of the specifiers described in Table 1. Minor melancholy refers to two to four symptoms of melancholy lasting for more than 2 weeks but less than 2 years. This scientific variant falls throughout the spectrum of persistent depressive dysfunction (dysthymia). In reality, bereaved people also can develop main despair, which might warrant further medical remedy (see Table 3). Following are some forms of manifestations: � Major depressive dysfunction, single episode: Episodes could occur only one time in life or may happen again years later, often triggered by major tense events. The first few episodes usually tend to be triggered by annoying life occasions, while in time the situation turns into self-maintained and self-triggered. Some patients present with melancholic options (profound lack of pleasure, melancholy worse in the morning, early morning awakening, extreme psychomotor retardation, extreme anorexia and weight loss). Atypical depression features are characterized by inverted useful shift (weight gain and increased appetite, longing for sweets, hypersomnia, leaden paralysis, long-standing interpersonal rejection sensitivity). There is a significant overlap between disruptive temper dysregulation disorder and the onset of bipolar dysfunction. Premenstrual Dysphoric Disorder � the situation is characterised by the majority of menstrual cycles that embody 5 symptoms. The following signs happen within the ultimate week earlier than the onset of menses and start to enhance within a quantity of days after the onset of menses. Substance/Medication-Induced Depressive Disorder this prognosis is used when persistent disturbance in temper predominates the scientific image and is characterized by despair and diminished interest or pleasure in activities. These signs occur throughout or quickly after substance intoxication or withdrawal or after exposure to a drugs. Depressive Disorder Due to Another Medical Condition this diagnosis is used when a depressive dysfunction is triggered by a medical situation (diagnosed by bodily examination and laboratory findings) known to trigger signs of despair. However, they might appear in one of the following varieties: � Recurrent transient depression (symptoms of despair lasting from 2 to 13 days no much less than as quickly as per month) not associated with menstrual cycles � Short-duration depressive episode (lasting from 4 to 13 days), with a minimum of four signs of main depressive episode associated with scientific distress and impaired functioning that persist but never meet standards of major despair � Depressive episode with insufficient symptoms (at least one of many signs of major despair related to distress and impairment persisting for at least 2 weeks with no prior history of major depression) these "other specified depressive disorders" are helpful to clinicians in refining the description of a clinical pattern exhibited by a particular patient. Unspecified Depressive Disorder Finally, the previously used designation of "not otherwise specified" now reads "unspecified depressive dysfunction" (when not certainly one of the criteria are fully met, yet the patient is suffering from a mood disorder). Hypomania A hypomanic episode is just like, however much less intense than, a manic episode. Usually, people with bipolar I disorder also have both manic and depressive episodes, however the depressions can vary from severe and disabling to very transient and unnoticed. Such individuals are usually not hospitalized for their hypomania and tend to operate comparatively properly between depressive episodes. Mixed States and Rapid Cycling the particular specifiers for bipolar disorder are combined states and fast biking. Mixed states refers to manic or hypomanic episodes with a minimum of three of the following depressive signs: prominent dysphoria or depressed temper, diminished interest in activities, psychomotor retardation, fatigue or loss of energy, emotions Specifiers for Bipolar and Related Disorders Please discuss with Table 1 for specifiers of depressive disorders that apply to bipolar problems as well. Diagnosis When confronted with symptoms of temper disorder, a clinician has to decide whether or not these are transient manifestations related to life circumstances or signs of treatable psychopathology. The medical evaluation of sufferers with mood issues starts with an intensive history of the current illness. At least three of the following also wants to be current: (1) inflated shallowness or grandiosity, (2) decreased want for sleep (yet still feeling rested), (3) extra talkative than usual or inability to cease talking, (4) flight of ideas or racing ideas, (5) distractibility, (6) enhance in goal-oriented actions (socially, sexually) or psychomotor agitation, and (7) excessive involvement in pleasurable actions with little regard for penalties. Contingent upon severity, combined states are normally accompanied by extreme impairment. Rapid biking refers to bipolar dysfunction that includes no much less than 4 episodes of illness per yr. In addition, bipolar problems may embody any of the specifiers described in Table 1. During a 2-year period (1 year in youngsters and adolescents), hypomanic and depressive periods have been present for no much less than half the time, and the individual has not been without symptoms for more than 2 months at a time. However, in the long run, some sufferers might develop signs of bipolar affective disorder. A variety of subclinical types of subthreshold cyclothymia may be encountered in clinical practice. Such sufferers tend to develop overt symptoms of cyclothymia, or even bipolar dysfunction, when uncovered to a big selection of psychosocial stressors, substance abuse, and/or a selection of drugs. Past historical past will provide not solely a suspicion toward a analysis but also clues towards scientific manifestations, which, within the circumstances of melancholy and mania, are sometimes just like previous episodes. An early historical past of childhood behavioral issues can constitute a precursor of mood issues. For depressive states, patients often exhibit psychomotor retardation; sluggish speech; constricted have an result on; and sluggish, observable mental activity. Patients show increased psychomotor activity, pressured speech, full or labile have an result on, and elevated mood. In common, the diagnosis of mood dysfunction is aided significantly by obtaining a collateral historical past from friends or family members. The value of the Mental Status Examination is enhanced if the clinician knows the affected person from before the mood dysfunction episode. While extremely helpful in quantifying signs of melancholy, psychological testing is time consuming and not necessary for the initial analysis of a mood dysfunction.
Blue Barberry (Oregon Grape). Pentoxifylline. - What is Oregon Grape?
- Stomach ulcers, heartburn, stomach upset, and other conditions.
- Dosing considerations for Oregon Grape.
- What other names is Oregon Grape known by?
- Are there safety concerns?
- How does Oregon Grape work?
- Are there any interactions with medications?
- Psoriasis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96499
Order genuine pentoxifylline on lineDespite intensive analysis efforts, the precise mechanisms and interrelationships between extracellular amyloid plaque and intracellular neurofibrillary tangle deposition remains elusive. In discussing this situation, several associated however distinctly completely different terms are used: � Cognitive impairment refers to the presence of one or more measurable deficits in cerebral function compared with regular persons of the same age. Each neurocognitive disorder is split into mild and main varieties, with the latter distinguished by clinically vital practical incapacity due to compromise in multiple domains. Word-finding difficulties, lack of time orientation, getting misplaced or misplacing things, and impaired judgment and planning are different frequent features. There are two common varieties: (a) cortical-resulting from a number of infarcts within the cerebral cortex; and (b) subcortical-resulting from small-vessel illness with multiple lacunar infarcts. This prognosis is relatively uncommon however accounts for as a lot as half of all instances before age 65. The scientific presentation is highly variable, depending on the lateral distribution of pathological modifications. Language disturbances involving expression or comprehension or outstanding changes in habits and personality. This is a situation by which the individual is prepared to carry out his or her regular actions however has deficits in sure areas of higher operate corresponding to short-term reminiscence, judgment, and planning. In contrast to the dementias, delirium tends to be subacute or acute in onset and to be utterly or partially reversible. Key characteristics include fluctuating consciousness, confusion, and hallucinations or delusions. The cause is normally identifiable and is most frequently because of medicine, stress (such as an infection or surgery), or a metabolic disturbance. Delirium often happens in sufferers with dementia, reflecting elevated vulnerability of a compromised mind to poisonous, metabolic, or infectious insults. Improved interviewing methods and routine use of despair screening checks as part of a dementia evaluation have largely eliminated this confusion. However, melancholy stays an essential consideration in the dementia analysis because it regularly coexists with dementia, significantly in early stages of the illness. Advantages of early prognosis include offering earlier treatment and analysis participation, allowing the individual a chance to make lifeplanning decisions at a point where his or her residual cognitive perform is at its finest, serving to family understand what is going on and learn the way finest to provide assist, offering guidance to patient and family about managing funds properly and avoiding scams, and providing time for determination making about such issues as durable energy of attorney and advance-care planning. Medicare at present requires cognitive screening as part of the annual Medicare wellness go to; as well as, we advocate screening anyone age 75 and older and anyone for whom a memory lapse or vagueness noted in an interview or an error in judgment. Each may be administered simultaneously by a nurse or medical assistant in about 3 minutes. It inquires about whether the person has had a change over the previous several years in eight areas: judgment, curiosity in hobbies/activities, repeating issues, studying, orientation, monetary management, remembering appointments, and other memory. In explicit, the examination should look for asymmetry in energy and/or motor perform (suggesting one or more prior strokes), tremor and bradykinesia (suggesting parkinsonism), abnormalities of eye motion, particularly lack of ability to gaze downward (suggesting progressive supranuclear palsy), and peripheral neuropathy (suggesting the possibility of vitamin B12 deficiency, hypothyroidism, alcoholism, or neurosyphilis [although diabetes is extra often the cause]). Laboratory Testing and Neuroimaging If the cognitive standing examination confirms dysfunction, then a laboratory battery ought to be carried out largely to assist identify remediable causes of cognitive impairment. It can identify cerebrovascular illness as discrete old infarcts (usually cortical) or as greaterthan-normal deep white-matter changes (leukoariosis, suggesting subcortical vascular disease). Judgment and decision-making could be impaired early within the disease, which can lead to an incident that pulls consideration to the issue. Examples embody auto accidents, uncharacteristic purchases or donations, issues managing a family budget, or being victimized by a scam. Increased awareness of early warning signs and following the Medicare requirement for cognitive screening should help identify the next proportion of sufferers with gentle, versus major, neurocognitive disorder. An individual who presents with reminiscence or other cognitive difficulties might not have the ability to present a dependable historical past. The main or at least collateral supply of historic details about functional change needs to be a member of the family near the person. An essential component of the historical past must be questions aimed toward identifying different potential causes of cognitive impairment, such as alcoholism, illicit drug use, and prescription medications. Cognitive Status Examination the cognitive status examination ought to embrace a standardized cognitive check, both for comparison with different patients and to present a numerical end result that can be followed over time. A widespread thread in this dualistic strategy is to promote security and quality of life for all involved. While cognitive operate is the necessary thing to prognosis, behavioral symptoms are sometimes crucial to handle in the context of administration and burden of care. Treatment 676 Counseling and Caregiver Support the patient and caregiver ought to be recommended concerning the illness course, about elevated safety dangers from such issues as operating equipment and driving a motorized vehicle, about the desirability of building a sturdy power of legal professional for well being care decisions, and concerning the value of having conversations early on about desires for end-of-life care, together with completion of advance directives. As the disease progresses, common conferences with the patient and family are necessary in order to anticipate and tackle key choice factors. Make certain the caregiver has a physician and is underneath remedy for any medical problems she or he could have. Management of Cognitive Symptoms the shortage of novel therapeutic approaches through the previous 10 years, despite very lively analysis, has been a serious disappointment. The cholinesterase inhibitors and memantine (Namenda) remain mainstays of remedy. Donepezil (Aricept), whereas usually given at bedtime, might cause leg cramps, insomnia, or vivid bizarre dreams that usually abate by switching to morning dosing. Management of Behavioral Symptoms A broad variety of behavioral symptoms can develop. Among the more frequent are (a) early within the disease-repetitive questions, wandering, and refusing assistance; (b) in the mid-stage of the disease-resistance to care, agitation or pacing, verbal and physical agitation and aggression, and delinquent behaviors corresponding to inappropriate sexual remarks; (c) late in the disease-resistance to care and repetitive vocalizations such as moaning and screaming. The key to managing most behavioral symptoms rests on nonpharmacologic approaches involving good adaptive dementia communication skills. Key parts include making eye contact before speaking; utilizing simple language; talking slowly, clearly, and in a low-pitched voice; speaking empathy via such actions as smiling and giving a hug; asking just one question at a time and permitting the patient sufficient time to respond; breaking directions down into small steps and presenting one at a time; and backing off and trying later if the particular person turns into agitated or refuses. Eliminating anticholinergic or lowering dopaminergic medicines must be the first line of therapy. This focus would include coordinating dementia screening within the practice, figuring out each of the sufferers and households with dementia, coordinating a support group (if the follow chooses to have one), and responding to questions from caregivers. Melanoma is a less-prevalent malignancy however has a high propensity to metastasize to the brain. Gliomas are major brain tumors which might be categorized as high-grade gliomas or low-grade gliomas. The histology of the first neoplasm confers the risk of mind metastases as a end result of lung most cancers, breast cancer, and melanoma are extra likely to metastasize to the brain, whereas colorectal, ovarian, and prostate cancers are less more probably to metastasize to the brain. Past publicity to ionizing radiation and a family history of a genetic cancer syndrome are the one known threat elements for major tumors. Despite a lot press, cell phone use has not been irrefutably proven to be a risk issue for brain tumors. A tissue prognosis through a biopsy or surgical resection is important to confirm the pathology, besides in sufferers with metastatic tumors with a identified major tumor.
Buy pentoxifylline 400 mg cheapPreliminary data suggest that dronabinol (Marinol) could additionally be of some utility in relieving cravings and withdrawal symptoms without inflicting intoxication. Even newer "safer" brokers corresponding to modafinil (Provigil) and armodafinil (Nuvigil) are associated with abuse and dependency, albeit much less commonly than with traditional stimulants. Prescription stimulant abuse can contain using extreme doses to obtain a euphoric high, or by way of nonmedical use or diversion of prescriptions. When taken at prescribed doses for an acceptable condition, even methamphetamine is generally secure and efficient. No other commonly abused drug is so strongly associated with permanent mind harm, resembling that seen in traumatic brain damage victims. To this finish, several latest pharmacologic developments have introduced improved choices for remedy. Cocaine and different stimulants induce sympathomimetic effects including tachycardia, hypertension, mydriasis, and diaphoresis. These drugs are generally associated with seizures, myocardial infarction, hemorrhagic strokes, dyskinesias and dystonias, and psychosis when taken at the doses usually used to achieve euphoria. Withdrawal is usually experienced as a crash and includes fatigue, depressed temper, elevated urge for food, and cravings. Considered nonaddictive until about 1980, cocaine is now well known as one of the most addictive drugs, significantly in the base type (crack or freebase). Currently, no medication has demonstrated efficacy in treating cocaine or stimulant dependence. Stimulant-induced psychosis and mania reply nicely to conventional psychotropics when warranted; nonetheless, to date, no medications have reliably demonstrated efficacy in stopping relapse. In the meantime, conventional psychosocial treatments stay the mainstay of scientific care. Opioids are categorized as endogenous (endorphins, enkephalins, dynorphins), opium alkaloids (morphine, codeine), semisynthetic (heroin, oxycodone [Roxicodone, OxyContin]), or artificial (methadone [Dolophine], fentanyl [Sublimaze, Duragesic]). The final three classes have a variety of scientific makes use of together with analgesia, anesthesia, antidiarrhea, cough suppression, and detoxification and maintenance remedy. The effect on mu receptors is considered the most important, with its activation directly linked to each analgesic and euphoric effects. However, when utilized in enough portions by genetically susceptible persons, some customers experience energy, aid of emotional pain, and a euphoria many describe as a "total body orgasm. The withdrawal syndrome is characterised by a constellation of depressing but not life-threatening symptoms including mydriasis, piloerection, muscle cramps, diaphoresis, vomiting, lacrimation, rhinorrhea, chills, insomnia, cravings, and autonomic hyperactivity. Since ache was acknowledged as "the fifth important signal" in the Nineties, concurrent with heavy marketing campaigns from pharmaceutical companies, the United States has experienced a veritable explosion of widespread opioid prescribing for nonmalignant pain. An whole industry of ache administration has developed, with the unlucky aspect effect of having a sizable proportion of its output getting used nonmedically. It is necessary for prescribers to acknowledge that the abuse potential of prescription opioids matches, or in some instances even exceeds, that of heroin. The commonest method of abuse entails merely taking more than prescribed, often by the suitable route of administration. Alternatively, opioid abusers generally take their medicines via nasal insufflation or inject them intravenously. The time-release property of certain drugs, similar to oxycodone (OxyContin), is well circumvented by crushing the pills, which significantly enhances the euphoric impact. Even transdermal fentanyl patches (Duragesic) are abused through any number of strategies, such as applying heat to a worn patch, using complex extraction methods described on the Internet, or simply sucking on the patch itself (a widespread finding by the coroner). Once the prescription is completed early, the user must both supplement the availability or face the unpleasant effects of withdrawal. These include seeing a number of prescribers (doctor shopping), purchasing on-line at foreign "pharmacies," and common trade or buy on the black market. Many states are implementing managed substance databases aimed to curb the problem of abuse of opioids and other prescribed drugs. Acute detoxing from opioids is achieved by way of certainly one of two primary methods: symptomatic remedy with unrelated drugs, or substitution with a cross tolerant (opioid) drug with much less abuse potential (Table 2). The first technique could make use of the use of clonidine (Catapres),2 an 2-adrenergic agonist, to assist with the autonomic part of withdrawal. This is commonly carried out together with different symptomatic treatments on an as-needed foundation, corresponding to diazepam (Valium) for nervousness, loperamide (Imodium) for diarrhea, and promethazine (Phenergan)2 or ondansetron (Zofran)2 for nausea. The second technique usually involves either methadone or buprenorphine (Subutex). Methadone, a pure mu agonist with a half-life of about 36 hours, is normally started in the 20- to 30-mg vary and titrated cautiously by 10 mg every 4 to 7 days. Maintenance therapy with methadone happens only in highly regulated methadone clinic settings. Buprenorphine, a partial agonist on the mu receptor (and kappa antagonist) is run sublingually and has a half-life just like that of methadone. It was accredited in 2002 for office-based therapy of opioid habit, making pharmacotherapy much more extensively out there. Caution ought to be used to not administer buprenorphine too soon (before onset of withdrawal syndrome), or acute withdrawal can truly be precipitated. Buprenorphine is out there both alone or in combination with naloxone (Suboxone). Here, the function of naloxone is solely to deter intravenous abuse, because naloxone is inactive when taken sublingually as prescribed. Buprenorphine and methadone are useful in managing acute withdrawal in addition to long-term (months to years) maintenance therapy for preventing relapse to heroin or the opioid of alternative. As upkeep remedy, these agents serve to block euphoria, satisfy cravings, and reduce illicit use, with consequent verifiable hurt reduction. Buprenorphine, with a built-in ceiling effect because of its unique pharmacology, is way safer than methadone, which is commonly deadly in overdose. Also permitted for prevention of opioid relapse is naltrexone, an opioid antagonist, which is on the market in oral (ReVia) and intramuscular depot formulations (Vivitrol). Drug Abuse Sedative-Hypnotics this class of medication contains a extensive array of compounds (benzodiazepines, barbiturates, and numerous associated compounds) (Table 3), most of which have a minimum of some potential for abuse.
[newline]Overall, these medicines do far more good than hurt, and are useful in treating anxiety disorders, insomnia, seizures, and muscle spasms. They are also important in managing withdrawal states and as a part of surgical anesthesia. Sedative-hypnotic intoxication and withdrawal states carefully resemble these of alcohol, except for a extra protracted time course of withdrawal. Anxiety, restlessness, insomnia, tremor, nystagmus, tachycardia, and hypertension often seem 2 to 12 hours after the last dose, and symptoms steadily resolve over 1 to 2 weeks. Detoxification is best accomplished on an inpatient basis and sometimes involves tapering doses of a long-acting benzodiazepine. Acute sedative overdose is managed primarily with supportive care and airway management. Since their introduction in the Sixties, benzodiazepines have largely changed barbiturates, given their enhanced security profile. Phenobarbital, used primarily for treating seizures, is taken into account to have low potential for abuse.
Pentoxifylline 400mg amexTypical dosing is chlordiazepoxide 50 to a hundred mg, diazepam 10 to 20 mg, oxazepam 20 to 403 mg, or lorazepam 2 to 4 mg. Long-acting barbiturates, such as phenobarbital1, can be also used on a fixed-dose routine of 60 mg every four to 6 hours, with a loading dose of a hundred and twenty mg orally or intramuscularly every hour for acute withdrawal symptoms. Thiamine (vitamin B1) supplementation of 100 mg/day for three days can counteract the thiamine deficiencies which would possibly be common in alcoholic sufferers. Psychosocial Interventions for Alcohol Use Disorder In addition to temporary interventions for dangerous alcohol use, the most opportune and sensible psychosocial intervention that the first care workplace can provide is scientific behavioral help for pharmacotherapy for alcohol dependence. Simply put, medication administration assist consists initially of suggestions to the affected person of screening and medical analysis outcomes and the negative well being effects of continued heavy drinking, as in a short intervention. Otherwise, price severity: 0 not present 1 very delicate 2 mild three moderate four moderately extreme 5 extreme 6 very extreme 7 extraordinarily severe Orientation and Clouding of Sensorium � Ask, "What day is this This evaluation for monitoring withdrawal symptoms requires approximately 5 minutes to administer. The patient is then given the idea for the analysis of alcohol dependence, the rationale for abstinence, and recommendation for pharmacotherapy. Follow-up visits encompass evaluation of medication unwanted effects, patient adherence to the medication routine, evaluation of abstinence or amount and sample of alcohol consumption, and assessment of total functioning. Any of those drugs can and should be given concurrently with different interventions corresponding to psychosocial therapy or mutual help teams. It reduces heavy ingesting total and helps maintain abstinence in those who are abstinent at preliminary drug administration. Acamprosate (Campral) is a taurine analogue that has been demonstrated to cut back relapse to any drinking as nicely as lowering heavy ingesting in nonabstinent sufferers. It is excreted unchanged through the kidneys and has no interactions with other drugs. Side effects are benign, and the most frequent is loose stools, that are delicate to average and self-limited. Bertholet N, Daeppen J-B, Wietlisbach V, et al: Reduction of alcohol consumption by transient alcohol intervention in major care systematic evaluate and meta-analysis, Arch Intern Med 165:986�995, 2005. The patient is given information about treatment and the suitable prescriptions and is encouraged to search community support for sobriety in mutual assist teams such as Alcoholics Anonymous or to follow a plan corresponding to Rational Recovery. Cognitive behavior remedy, community remedy, behavioral family remedy, and motivational interviewing are effective approaches for the therapy of alcohol dependence. Disulfiram (Antabuse) works by inhibiting the metabolism of ethyl alcohol, inflicting a buildup of acetaldehyde, a noxious substance, which causes a powerful stereotypic aversive response (flushing, diaphoresis, nausea, tachycardia) within the patient. The major medical concern with disulfiram is affected person noncompliance with the medicine regimen. More just lately, the opioid antagonist naltrexone (ReVia) was accredited for the therapy of alcohol dependence. Naltrexone in a long-acting intramuscular formulation (Vivitrol) permits once-monthly dosing (380 mg) and reduces the chance of noncompliance. Common side effects include paresthesias, style perversion, decreased appetite, and difficulty concentrating. Preventive Services Task Force: Screening and behavioral counseling interventions in primary care to scale back alcohol misuse: recommendation statement, Ann Intern Med a hundred and forty:554�556, 2004. American Psychiatric Association: Diagnostic and statistical handbook of psychological problems, fifth ed. Epidemiology Delirium is a typical medical condition seen in numerous care settings. Patients that suffer from delirium have longer hospital stays, larger prices of care, larger risk of long-term cognitive impairment, and increased mortality charges. Alteration of neurotransmitter levels, similar to extra dopamine, depletion of acetylcholine, or melatonin deficiency are doubtless involved within the growth of delirium. However, remedies focused at correcting these imbalances have mixed outcomes, further accentuating the complexity of the sickness. Moreover, predisposing factors such as cognitive dysfunction, superior age, and chronic medical circumstances have an effect on the magnitude of neuronal resiliency needed to stand up to precipitating events. Prevention Risk Factors Once viewed as a reversible course of attributable to a single underlying trigger, delirium is now believed to be multifactorial. Several threat elements have been recognized and could be divided into predisposing and precipitating elements as famous in Table 1. A advanced relationship exists between predisposing factors and exposures to precipitating occasions. A weak patient may solely require a small triggering incident whereas a healthy affected person may be subject to a number of noxious insults, however each could lead to delirium. To reduce the possibility of delirium, modifiable variables ought to be assessed and eliminated. Recent evidence means that a quantity of completely different units of interacting biologic factors instigate the disruption of large-scale neuronal networks within the mind, leading to acute cognitive dysfunction. Ultimately, a quantity of insults may find yourself in neuronal cell apoptosis and decreased synaptic plasticity. Contributing biologic factors could include neuroinflammatory processes, neurotransmitter disruption, and circadian rhythm dysregulation. For example, insults corresponding to severe infection, surgery, and trauma are recognized to enhance inflammatory cytokines and endotoxins. Three subtypes of delirium have been recognized: � Hypoactive (at least 4 of the following): unawareness, decreased alertness, decreased or delayed speech, lethargy, slowed actions, staring, apathy, diminished appetite, or new incontinence. Diagnosis Unfortunately, lack of recognition by health-care professionals is a significant concern and the analysis of delirium is often missed. The key to early identification is having a high scientific suspicion of the syndrome. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, the next 5 criteria must be fulfilled to precisely diagnosis delirium. The disturbance develops over a short time frame (usually hours to a number of days), represents a change from baseline attention and awareness, and tends to fluctuate in severity through the course of a day; 4. There is proof from the history, bodily examination, or laboratory findings that the disturbance is a direct physiologic consequence of another medical situation, substance intoxication or withdrawal. When carried out by a skilled particular person, this instrument is reported to have 94% to 100% sensitivity and 90% to 95% specificity in detecting delirium. For most sufferers this includes a full blood rely, complete metabolic panel, urinalysis, chest radiograph, and electrocardiogram. Individual situations may warrant additional diagnostic investigation such as a computerized tomography scan, electroencephalogram, lumbar puncture, or supplementary laboratory exams. Multiple mnemonics have been created to help in identification of underlying medical circumstances that may cause or contribute to delirium. For preliminary symptom administration, nonpharmacologic tactics are the first-line technique. The most widely disseminated strategy is the Hospital Elder Life Program, a multicomponent hospital intervention technique involving health-care professionals, households, caregivers, and sufferers. Pharmacologic therapies should be reserved for severely agitated sufferers, psychotic individuals, or those who threaten substantial harm to self or others.
Buy pentoxifylline with a visaIt is structured and generally brief time period with an emphasis on reducing symptoms and stopping "flare-ups" by monitoring and altering unhelpful or inaccurate pondering patterns that lead to emotions of tension and fear. Its efficacy can be contingent upon the power of the therapist and the length of time in therapy. Comorbid psychiatric issues considerably decrease the probability of restoration from anxiety and enhance recurrence charges. If benzodiazepine remedy was initiated, this frustration can and does often lead to an elevated dependence on the treatment and a requirement of more and more higher doses to achieve the identical effect. For long-term gains, remedy along with medicine treatment ought to be beneficial. Education is critical to reassure the affected person that efficient remedy is out there, but that patience may be necessary until the best mixture of modalities is found. Although all anxiousness disorders display a major amount of chronicity, most patients have an improved consequence with acceptable remedy. Patients with an earlier onset of signs (childhood or adolescence) can typically anticipate a extra chronic course and their anxiety symptoms could additionally be harder to deal with. Patients not often have a spontaneous remission of symptoms, however most can proceed to perform despite the symptoms. Nevertheless, time to decision of symptoms is shortened and total functioning usually improves with remedy. Despite the prevalence of anxiety disorders, patients usually stay undiagnosed and untreated, and sufferers with unrecognized nervousness disorders tend to be higher utilizers of general medical care. Patients with anxiousness problems can current with multiple somatic complaints and comorbid disorders, inflicting great effort and expense in identifying the cause of unexplained symptoms. The previously entitled "not otherwise specified" syndromes are now called "unspecified mood problems. X Psychiatric Disorders Conclusion 768 Anxiety disorders are highly prevalent in the United States. This condition can be disabling and expensive to the affected person and to the health care system. Once an nervousness dysfunction is identified, patients may be handled utilizing well-tested and efficacious pharmacologic and psychotherapeutic treatments. References Mood disorders and mood dysregulation encompass a broad vary of human experiences. They can be divided into three forms of manifestations: (1) psychiatric problems, which make up a major chapter in medical texts; (2) a big selection of temper syndromes, usually comorbid, less properly categorized, that coexist with medical and psychiatric issues alike; and (3) an combination of reactive transient behavioral manifestations exterior the pathologic realm, inherent to human nature. A thorough account of all symptoms current in a patient can level to treatment alternative and outcome. Depression signs could be classified into at least three main groups: � Emotional symptoms: disappointment, dysphoria, emotional numbness � Physical signs: low power, sluggishness with difficulties in initiating actions, difficulties concentrating, sleep and urge for food problems � Cognitive (mental) symptoms: pessimism, lack of enthusiasm, hopelessness, thoughts of death Not all three teams of signs are current from the start. In many people, the presence of cognitive symptoms may be an indication of chronicity. At different times, it might have been a premorbid feature or a continuing presence between episodes. Cognitive symptoms tend to respond both to medication and to psychotherapy (cognitive-behavioral techniques), and their monitoring is paramount to suicide prevention. If a mood disorder is secondary to a medical situation, the analysis might be made both by monitoring for temper symptoms and by pathognomonic medical findings. Differential Diagnosis Given the multitude of scientific manifestations, a differential diagnosis each between subtypes of mood issues and between temper and different psychiatric problems is critical. Table three presents comparisons and variations between subtypes of mood problems and pointers to the differential diagnoses. Depending on the first prognosis, the clinician might choose between including this specifier or the comorbid separate prognosis of "anxiety dysfunction" along with temper dysfunction. Treatment As a common rule, the therapy method to mood problems depends on the combination of psychopharmacology and psychotherapy. Close monitoring of remedy with frequent visits usually predicts higher end result. In common, response is taken into account to be a 50% reduction of signs, whereas remission refers often to the absence or only minimal signs for six months or more. Mood Disorders: Depression, Bipolar Disease, and Mood Dysregulation Treatment of Unipolar Depression (Major Depression and Dysthymia) Given the reality that many depressive problems occur alongside a spectrum, the remedy of major melancholy and dysthymia shall be covered together. Many clinicians favor to provoke therapy with psychotherapy, which includes addressing quite lots of family issues, before initiating psychopharmacologic intervention. In medical practice, other factors have to be weighed when choosing the primary antidepressant. Prior response history to a specific antidepressant or to an general treatment modality ought to take precedence in the first choice of remedy. If such a history is unavailable, any household history of response to a specific remedy should be thought-about. Table 4 includes a listing of the more frequent drugs used in medical apply for the remedy of unipolar and bipolar dysfunction. Given the potential for manic switch with antidepressants, it is recommended that in bipolar depression, temper stabilizers be began concomitantly with antidepressants. Any trial of medications must be continued for four to 6 weeks earlier than failure is said. However, clinical judgment in assessing each circumstance, especially relating to suicide danger, is essential. The coexistence of higher power and thoughts of demise may represent a brief suicide risk within the preliminary part of antidepressant treatment. Currently, organic markers for the prediction of therapy response and side effects are being thought-about. Results can be found for antidepressants, temper stabilizers, stimulants, second-generation antipsychotics, and so forth. Given the danger of suicide, close monitoring during therapy of main melancholy is required. The alternative of medication and adjustment has to be tailor-made according to the most dominant preliminary presentation. Currently, for atypical depression, clinicians choose as a first selection a norepinephrine/serotonin reuptake inhibitor (venlafaxine [Effexor], desvenlafaxine [Pristiq]) or a norepinephrine/dopamine energetic medication (bupropion [Wellbutrin]). Again, early in treatment, a thorough medical workup, which should all the time embody a thyroid panel, must be the norm. Pharmacologic augmentation with mood stabilizers, neuroleptics, and thyroid hormone has been utilized in circumstances of treatment-resistant melancholy. Medication resistance (after several failed trials) dictates the reassessment of analysis to additional rule out psychiatric and medical comorbidity. For medication-resistant mood issues, Table 5 presents an inventory of further biological treatments.
References - Chow PH, Chan CW, Cheng YL: Contents of fructose, citric acid, acid phosphatase, proteins and electrolytes in secretions of the accessory sex glands of the male golden hamster, Int J Androl 16(1):41n45, 1993.
- Manucha W, Carrizo L, Ruete C, et al: Apoptosis induction is associated with decreased NHE1 expression in neonatal unilateral ureteric obstruction, BJU Int 100(1):191n198, 2007.
- Kurth K, Tunn U, Ay R, et al: Adjuvant chemotherapy for superficial transitional cell bladder carcinoma: long-term results of a European Organization for Research and Treatment of Cancer randomized trial comparing doxorubicin, ethoglucid and transurethral resection alone, J Urol 158:378n384, 1997.
- Tunis, M. M., & Wolff, H. G. (1954). Studies on headache: cranial artery vasoconstriction and muscle contraction headache. Archives of Neurology and Psychiatry 71, 425.
- McVary KT, Monnig W, Camps JL Jr, et al: Sildenafil citrate improves erectile function and urinary symptoms in men with erectile dysfunction and lower urinary tract symptoms associated with benign prostatic hyperplasia: a randomized, double-blind trial, J Urol 177(3):1071, 2007. McVary KT, Roehrborn CG, Kaminetsky JC, et al: Tadalafil relieves lower urinary tract symptoms secondary to benign prostatic hyperplasia, J Urol 177(4):1401, 2007. McVary KT, Roehrborn CG, Avins AL, et al: Update on AUA guideline on the management of benign prostatic hyperplasia, J Urol 185:1793n1803, 2011.
|
|


