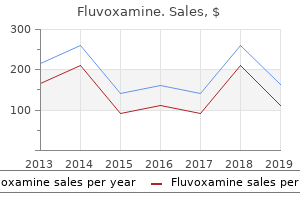
"Buy fluvoxamine discount, anxiety helpline."By: Joshua C Briscoe, MD - Medical Instructor in the Department of Psychiatry and Behavioral Sciences
- Medical Instructor in the Department of Medicine
 https://medicine.duke.edu/faculty/joshua-c-briscoe-md
Discount 100mg fluvoxamine fast deliveryStatins have potential advantages, together with: � Protection of the vascular endothelium. From a clinical point of view, statins: � Decrease the incidence of brain and cardiovascular events. It is our current apply to use of simvastatin or atorvastatin forty mg every day for 1 week and then continue with 20 mg/day for the first 3 months after an ischemic cerebrovascular occasion. Brain oxygenation and power metabolism: part I-Biological function and pathophysiology. Supplement to the guidelines for the administration of transient ischemic assaults: A assertion from the 771 Intensive Care in Neurology and Neurosurgery � � � � � � � � � � � � � � � Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks, Stroke Council, American Heart Association. Clinical follow pointers: prognosis and quick administration of transient ischemic attacks in adults. Report of the joint stroke pointers development committee of the American Academy of Neurology and the American Stroke Association. The American Academy of Neurology affirms the worth of this assertion as an academic software for neurologists. Primary prevention of ischemic stroke: a press release for healthcare professionals from de Stroke Council of the American Heart Association. Validation and refinement of scores to predict very early stroke danger after transient ischemic attack. Circulation 2006; 113: e409-49 Carotid Disease � Brott T, Brown R, Meyer F, et al. Carotid revascularization for prevention of stroke: carotid endarterectomy and carotid artery stenting. Safety and efficacy of endovascular remedy of carotid artery stenosis compared with carotid endarterectomy: a Cochrane systematic review of the randomized evidence. Beneficial results of carotid endarterectomy in symptomatic sufferers with high-grade carotid stenosis. Stroke 1985; 16: 885-90 � Treatment of Ischemic Stroke � 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: Part 9: Adult stroke. Stroke Council of the American Stroke Association: Guidelines for the early administration of sufferers with ischemic stroke: A scientific statement from the Stroke Council of the American Stroke Association. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke three to 5 hours after symptom onset. Expansion of the time window for therapy of acute ischemic stroke with intrave- � � � � � � � � � � 774 Acute Ischemic Stroke: General Approach � � � � � � � � � � � � � � � � � � � nous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Serum glucose stage and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Body temperature in acute stroke: relation to stroke severity, infarct measurement, mortality and outcome. Disturbances of sodium in critically grownup neurologic sufferers: A clinical review. Acute hyperglycemia and the innate immune system: clinical, mobile and molecular features. Neurology 2002; fifty nine: 67-71 776 43 Ischemic Penumbra: Role of Neuroimaging in Treatment Decision Alvaro Cervera 1, Geoffrey A. However, as a end result of the slender time window, lower than 5% of patients with this condition obtain this drug. To be able to deal with a higher variety of sufferers it might be essential to lengthen this time window. There are totally different approaches aimed at increasing the normal 3 hour time window. There are research analyzing the efficacy of alteplase in eligible sufferers who present with acute ischemic stroke in both the 3-4. The second approach is to choose patients that are extra likely to reply to the thrombolytic remedy. This will result in ischemic harm, which magnitude and localization will depend on the extent, severity, and duration of the perfusion deficit. However, not all the hypoperfused tissue surrounding the ischemic core can be called ischemic penumbra. This idea arose by scientific observations of fluctuating neurological deficits that instructed completely different perfusion thresholds for lack of neuronal perform and cell demise. Schematic illustration of the of these thresholds in experimental mod- ischemic tissue after a major vessel occlusion. The ischemic penumbra duced cerebral blood move, absent electri- is represented by the "A" space. This is the tissue cal activity, however preserved ion homeostasis that might be salvaged after using thrombolytic and transmembrane electrical potentials. Penumbral tissue is an irregular tissue with physiological and biochemical characteristics of cellular dysfunction but not mobile death, caused by hypoperfusion. The primary relevance of this tissue is that it can both survive or progress to necrosis, and its salvage is related to better clinical end result. The tissue surrounding the infarct core stays viable, but severely compromised due to metabolic, hemodynamic, and neurochemical alterations attribute of the ischemic environment. The dissociation between metabolism and circulate is pronounced in focal cerebral ischemia. Maintenance or focal will increase in glucose utilization have been observed in mind regions adjacent to the ischemic core. Therefore, the uncoupling of metabolism and move is an important pathogenetic mechanism that affects the crucial power stability within the penumbra. Lastly, the ischemic penumbra is a dynamic tissue structure of restricted viability surrounding a spotlight of dense cerebral ischemia. Therefore, with time will increase the viability of the penumbra will lower and more tissue will be recruited in the core. There are many neuroimaging tools which have shown efficacy in penumbra assessment. It is predicated on the detection of pairs of gamma rays emitted by a positron-emitting radionuclide (tracer), which is introduced in to the body on a biologically lively molecule. Thus, in ischemic stroke is possible to detect the 4 tissue subtypes: core, penumbra, oligaemia and unaffected tissue, in addition to the thresholds that reliably and efficiently separate them. This ligand it is prepared to distinguish ischemic core from penumbral tissue early after acute stroke. Another marker, 18F-fluoromisonidazole, supplies a direct image of the penumbra, however not of the ischemic core. Studies with 18F-fluoromisonidazole have proven that penumbra could final for long periods in some patients, and that penumbral salvage is time-independent, with a minimum of 50% tissue survival even beyond 12 h. Tmax is the time to peak of the residue function, indicating bolus delay between the positioning of number of the arterial enter function and the tissue. Therefore, Tmax represents bolus arrival time, with out the confounding effects of bolus administration.
Diseases - Seemanova Lesny syndrome
- Barbiturate overdose
- Mental retardation nasal papillomata
- Mental retardation, X linked, Marfanoid habitus
- Hymenolepiasis
- Myopathy Moebius Robin syndrome
- Kaolin pneumoconiosis
- Hereditary peripheral nervous disorder
Buy fluvoxamine discountInterstitial tubal implantation: the placenta may get implanted in the part of the fallopian tube passing through the uterine wall. Layers of Placental Barrier Up to the Third Month of Pregnancy From fetus to mother: i. The placenta acts as transport of oxygen, water, electrolytes and nutritions between the maternal to fetal blood. It also helps excretion of carbon dioxide, urea and other metabolic finish product from the fetus in to the maternal blood. Transport of maternal antibodies (IgG gamma globulins) reaching the fetus by way of the placenta fetus will get passive immunity from the mother towards infectious diseases like diphtheria, chicken pox and whooping cough. It prevents the entry of many bacteria and other dangerous brokers from mother to fetus. Most of the viruses like poliomyelitis, measles and rubella and some bacteria can pass across it. Most of the medication taken by the mom move by way of the placenta and might produce congenital malformations. Lesion of the cervical a half of the spinal wire which interrupt the reticulospinal tracts, carrying fibers from the hypothalamus to the sympathic outflow to the primary thoracic phase of the spinal wire. Clinical Features Formation � Growthretardation � Mongolianfacewithflatnose Notochord is fashioned within the following stages: � Mentallyretarded 1. Appearance of blastopore: A depression medial corners of the eyes) appears in the heart of the primitive node. Formation of notochordal process: It is the cranially prolonged part up to the prochordal plate by the multiplication of the cells of the primitive knot. Formation of notochordal canal: the blastopore extends in to the notochordal course of and converts in to a canal referred to as notochordal canal. Appearance of neuroenteric canal: the ground of the notochordal canal break forming small openings and talk between the yolk sac and amniotic cavity. Formation of notochordal plate: the opening quickly becomes confluent and the ground of the notochordal canal closed, flattened to notochordal plate. Formation of notochord: Finally, the cells of the notochordal plate life prorate and thickened forming in to a strong rod of cells known as notochord. Posterior or inferior: On its free margin often presents two clefts, which subdivides the cusp in to three scallops Fate 1. Free margin: Connected with the chordae tendineae, on the free margin of the post leaflet usually presents two clefts. The cusps are closed during ventricular systole by the apposition of the ventricular surfaces with the zones of the adjoining cusps. The tough zone: It is thick and provides attachments to the chordae tendineae on its ventricular surface. The basal zone: It is thick and vascular about 2 to three mm in extent and supplies attachments of to the basal chordae on its ventricular floor. These are connecting the apical one-third a half of the papillary muscle tissue to the free margins and ventricular floor of the cusps. The chordae tendineae are assist in the valve closure during ventricular systole and prevent eversion of the cusps in the path of the atrium. They are following: � Commissural � Cleft � Freemarginal � Roughzone � Deep � Basal. Commissural and Cleft Chordae: They are fan formed, and hooked up to the commisssures and free margins of the adjoining cusps or scallops. Free Marginal: these are attached to the margins of the cusps and dividing in to branches: Rough zone chordae, deep chordae and basal chordae. Rough Zone Chordae: these are consists of three strands, one is connected to the free margin, one to the junction of rough and clear zones and the opposite to the tough zone midulary between former two. Blood supply is just current in the collagenous ring and within the basal one-third of the cusps. Central two-thirds of the cusps derived their diet from the blood within the cavity of the heart. These are conical muscular projections Number: Usually three in numbers Position: Anterior, posterior and septal (medial) Base of the anterior papillary muscle (largest) is hooked up to the sternocostal surface near the septal wall v. The septal papillary muscle is smaller and is attached to the ventricular septum the Chordae Tendineae i. The apical one-third of the papillary muscles gives attachments to the chordae tendineae which are anchored to the tricuspid valves viii. The chordae tendineae of anterior papillary muscle are hooked up to the anterior and posterior cusps, and posterior papillary muscle is connected to the posterior and septal cusps ix. Functionally, the valve cusps are saved competent by energetic contraction of the papillary muscles. Carrying motor and sensory (mixed) fibers: Fifth, seventh, ninth and tenth nerves. Origin the fibers of the olfactory nerve arise from the central processes of the bipolar olfactory cells that are positioned olfactory zone of the nasal mucous membrane. The olfactory nerve contains about 20 bundles which move via the foramina of the cribriform plate of ethmoid bone in lateral and medial teams ii. The bundles of olfactory nerve end in the glomeruli of the olfactory bulb which is situated at the anterior finish of the olfactory sulcus on the orbital surface of the frontal lobe of the cerebral hemisphere iii. The olfactory nerve could be tested by applying the substance of varied odors to every nostril alternately ii. The check of odor sensation is completed by the asking the patient to close his or her eyes and soaked cotton of the food flavors iii. Formation/Origin It is made up of the axons of ganglionic cells within the ganglionic layer of the retina. Anosmia: It means loss of odor of sense which can outcome from severe injuries of the anterior cranial fossa a tumor or abscess in the frontal lobe of the mind, and so on. It is roofed by three layers of meninges of the brain with subdural and subarachnoid areas. It will get rich blood provide as vascular pial sheath gives quite a few septa in to the substance of the nerve. It has a slightly sinuous course, the nerve being about 6 mm longer than the space between the optic canal and the eyeball. Anteriorly: Separated from the cone of muscle tissue by fat, in which incorporates the ciliary vessels and nerves. The optic nerve begins at the optic disk (blind spot) where the fibers of stratum opticum converge ii. It pierces the choroid and lamina cribrosa sclerae at the posterior part of eyeball about three or 4 mm in the path of the nasal aspect of its posterior pole iii. Then the optic nerve runs backwards and medially and passes by way of the optic canal to enter the center cranial fossa the place it joins with the optic chiasma. Cranial Nerves and Some Neural Pathways 603 Laterally: the ciliary ganglion lies between the optic nerve and lateral rectus muscle. Inferomedially: the central artery and vein of the retina pierce the optic nerve about 12 mm behind the eyeball. Medially: Sphenoidal and posterior ethmoidal air sinuses separated by a skinny osseous lamina.

Order fluvoxamine 50 mg otcExtensor pollicis longus cross the extensor carpi radialis longus and brevis of the wrist, and inserted to the bottom of the distal phalanx of the thumb v. Extensor digitorum, it divides in to 4 tendons for the second to fifth digits and inserted by way of dorsal digital expansions vi. Extensor indicis, it blends with the decrease and medial aspect of the extensor digitorum tendon for index finger vii. Extensor digiti minimi, it blends with extensor digitorum for the little finger on its medial aspect viii. Now, expose the anatomical snuffbox-By retracting the abductor pollicis longus and extensor pollicis brevis laterally and extensor pollicis longus medially which comprise from superficial to deep i. Now, expose the ground of the anatomical snuffbox which is shaped, by the following bones from proximal to distal-styloid process of radius, scaphoid, trapezium and base of the primary metacarpal bones. Now, remove the fat and fasciae within the dorsal floor of the intermetacarpal spaces and expose dorsal interosseous muscle in every space. Now, separate the dorsal interosseous muscle from the 2 adjacent metacarpal bones from where it originates. An oblique incision is given along the inguinal ligament from the symphysis pubis to the anterior superior iliac backbone iii. Superficial fascia on abdomen is divided in to two layers below the extent of umbilicus: a. The membranous layer of superficial fascia generally recognized as fascia of Scarpa mendacity deep to it. Superficial circumflex iliac artery going in direction of anterior superior iliac spine d. Anterior cutaneous branches of the arteries accompanying the anterior cutaneous nerves discovered on either facet of midline. Iliohypogastric nerve on the upper part of inguinal canal going downwards and medially c. The superficial fascia in two layers are minimize and mirrored like skin-structures uncovered. External oblique muscle going downwards and medially, turning into aponeurotic beneath the line joining anterior superior iliac spine with umbilicus b. Linea alba: It is avascular fibrous structure connecting symphysis pubis to xiphoid course of c. The iliohypogastric nerve enters the rectus sheath by piercing the exterior obliquus aponeurosis g. Superficial inguinal ring transmitting the ilio inguinal nerve and spermatic twine in male or round ligament of uterus in female. Incision on the Anterior Wall of Rectus Sheath the anterior wall of rectus sheath is minimize by vertical incision � inches lateral to linea alba, dissecting the tendinous intersections. Rectus abdominis going upwards to turn into expanded from pubic crest and symphysis pubis to the lower costal cartilages It is adherent to the anterior wall of rectus sheath by tendinous intersections but free from posterior wall ii. Pyramidalis muscle when present arising from the pubic crest to be inserted in to the linea alba iii. The rectus abdominis muscle is retracted laterally preserving its supplies-structures uncovered: i. Posterior wall of rectus sheath fashioned by the posterior lamina of the inner indirect and transversus abdominis muscle tissue It is deficient above the costal margin the place the rectus abdominis lies directly on the costal cartilages to give entry to superior epigastric vessels. Superior epigastric artery enters the rectus sheath where the posterior wall of rectus sheath is deficient above. A long with the superior and inferior epigastric arteries the accompanying veins also present. Posterior wall is deficient: Here the rectus abdominis muscle immediately lies over the costal cartilages. The area starting from midpoint between xiphoid course of and umbilicus as a lot as the midpoint between the umbilicus and symphysis pubis: i. Steps of Dissection Position of Body Body will be in supine place with hip joint prolonged. A horizontal incision is given on the degree of anterior superior iliac backbone going from it to the midline of abdomen ii. A vertical incision is given along the midline from the medial finish of 1st incision, downwards to the symphysis pubis. Now, the triangular skin flap thus mapped is reflected downwards and laterally-structures uncovered: i. Superficial circumflex iliac artery, going upwards and laterally to the anterior superior iliac backbone vi. Superficial veins are dissected out in this region accompanying with the superficial arteries vii. Iliohypogastric nerve, happening wards and medially from the middle of the area. The external oblique aponeurosis with its fibers are dissected downward medially and forwards ii. The inguinal ligament shaped by the condensation of exterior obliquus abdominis aponeurosis iii. The superficial inguinal ring lying above and lateral to the pubic tubercle, transmitting the spermatic twine in male or spherical ligament of uterus in feminine, together with ilioinguinal nerve. The superficial inguinal ring is a triangular aperture bounded by upper or medial crus attached to the pubic tubercle, a lower or lateral crus connected to the pubic crest and intercrural fibers connecting two, being directed upwards and laterally. The iliohypogastric nerve piercing the aponeurosis about three cm above the superficial inguinal ring passes forward and medially. The external indirect aponeurosis is reflected from its insertion-structures uncovered: i. The internal oblique muscle arising from the lateral twothirds of the inguinal ligament going upwards and medially to reach over the inguinal canal to kind the conjoint tendon medial a half of inguinal canal 658 Human Anatomy for Students. The inguinal canal transmitting the spermatic wire in male and spherical ligament of uterus of feminine together with the ilioinguinal nerve solely in its medial half iii. The iliohypogastric nerve piercing the inner indirect about 2 cm medial to the anterior superior illiac backbone v. The inside indirect muscle is cut in its origin and reflected-structures uncovered: i. The transversus abdominis muscle is arising from the lateral onethird of inguinal ligament going backwards forming the roof of the inguinal canal, and turning downwards and medially to kind conjoint tendon ii. The cremasteric muscle and its fascia arising from the transversus abdominis and in addition inside oblique to be part of the masking of spermatic cord in male and is much less prominent in feminine iii. The circumflex iliac artery going upwards between transversus abdominis and internal oblique v. The complete size of inguinal canal containing the spermatic wire in male and spherical ligament of uterus in feminine vi.

Order 100mg fluvoxamine with amexFurthermore, a simple rating chart was developed to estimate the outcome probability. For deciding on the variables these for which there was sturdy evidence of an affiliation with the outcomes in each regions were selected, so that a common core of variables could possibly be chosen. The rationale for this technique was that a common mannequin for the different areas and outcomes can be less complicated to use. Plausible explanations for this relationship embody extracranial comorbidities, adjustments in mind plasticity, or variations in medical administration associated with increasing age. Pupil Reactivity In settlement with earlier studies, the absence of pupil reactivity was a strong predictor of poor end result. The effect estimate (odds ratio) for mortality was among the many highest of all predictors. This finding could possibly be explained by random error, as the usual errors have been bigger because of the relatively low frequency of pupil abnormalities (6% with one pupil unreactive and 8% with each pupils unreactive). Cause of Injury Cause of harm was not found to be an impartial predictor of poor outcome. Unfortunately, the "different" category includes a extensive range of diverse causes, so it was not attainable to disentangle the potential explanation for this finding. Gender There was no strong proof for an association between gender and poor end result. As previously reported, traumatic subarachnoid hemorrhage was found to be an independent predictor. The finding that a non-evacuated hematoma was associated with an increased risk of poor end result is consistent with studies showing an increased threat of poor consequence with different varieties of intracranial hematoma. Differences within the Strength of Association of Predictors Another important discovering was the difference observed within the power of affiliation between several important predictors and consequence. The other variable that showed a special strength of associations in accordance with the area was age. The core mannequin was developed utilizing the entire dataset (8509 patients), while the opposite two models used smaller samples as they have been pressured to limit the sample to research with the related variables. The prolonged mannequin was derived from 6999 patients and the laboratory model from 3554 sufferers. Because of missing values for a number of the variables within the completely different research, they used the tactic of chained equations to impute the missing knowledge. A complete of 5%, 13% and 8% of the values have been imputed on the core model, the prolonged model and the laboratory mannequin, respectively. The discriminatory capability of the fashions for predicting unfavourable consequence at 6 months within the inside validation ranged from zero. The calibration was poor for all the models when assessed with the Hosmer-Lemeshow take a look at (p <0. The authors offered a simple score with an accompanying determine and also made the fashions obtainable as a web-based calculator. Finally, each studies attempted to make the models simply obtainable to docs worldwide with a web-based calculator and in a simple paper-based format. Finally, a typical characteristic of the external validation for each studies was that the discrimination was acceptable, however the calibration was poor when assessed with the Hosmer-Lemeshow test. All of those components provide reassurance concerning the internal validity of the models. The large sample measurement in relation to the variety of prognostic variables examined is one other particular power. Finally, the information required to make predictions with the mannequin are simply obtainable to clinicians, and a web-based risk calculator was developed. There are some limitations: the data from which the models had been developed originate from a clinical trial and this might subsequently limit its exterior validity. The exterior validation showed good discriminatory ability, albeit somewhat lower than in the authentic knowledge. The calibration of the models was good when evaluated with the Hosmer-Lemeshow take a look at. Most importantly, the fashions kept an appropriate discriminative capacity when externally evaluated, although the calibration, in particular for the basic mannequin, was poorer. The fashions were developed and validated via a rigorous methodological process to ensure their inner validity. Traumatic brain harm: classification of initial severity and determination of functional consequence. Size and quality of randomised controlled trials in head harm: evaluate of printed studies. Young men were vulnerable to becoming lost to follow-up in a cohort of head-injured adults. Addressing the rising burden of trauma and harm in low- and middle-income nations. J Head Trauma Rehabil 1999; 14: 602-15 694 Prognosis in Traumatic Brain Injury 19. Identifying phases of investigation helps planning, appraising, and applying the outcomes of explanatory prognosis studies. Attitude and self-reported apply relating to prognostication in a national sample of internists. Systematic reviews in well being care: Systematic reviews of evaluations of prognostic variables. Methodologic requirements for the event of clinical determination guidelines in emergency drugs. Translating medical analysis in to medical practice: impact of utilizing prediction rules to make choices. Short-term mortality predictions for critically ill hospitalized adults: science and ethics. Assessing the performance and scientific impression of a computerized prognostic system in severe head harm. Effects of computerized medical determination help techniques on practitioner efficiency and affected person outcomes: a systematic review. Bias and uneven loss in expert forecasts: a study of physician prognostic habits with respect to patient survival. Neuroprotection in traumatic mind damage: a posh battle towards the biology of nature. Progression of traumatic intracerebral hemorrhage: a potential observational examine. Glasgow Coma Scale rating, mortality, and practical consequence in head-injured patients. Patient age and consequence following severe traumatic brain harm: an evaluation of 5600 patients. Traumatic intracerebral hematoma-which patients should undergo surgical evacuation Acute subdural hematoma-prediction of end result with a linear discriminant function. Prediction of end result in traumatic brain damage with computed tomographic traits: a comparability between the computed tomographic classification and combinations of computed tomographic predictors. Head harm outcome prediction in the emergency division: a job for protein S-100B Prediction of consequence and the administration of severe head injuries: the attitudes of neurosurgeons.
Langwort (Butterbur). Fluvoxamine. - Are there any interactions with medications?
- What is Butterbur?
- Dosing considerations for Butterbur.
- Pain, colic, cough, asthma, irritable bladder, urinary tract spasms, wounds, and other conditions.
- How does Butterbur work?
- Are there safety concerns?
- Hayfever caused by grass pollen.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96639

Generic 100mg fluvoxamine fast deliveryThe edema that could be present from the start can also improve and generate mass effect. Intracerebral hemorrhage is a homogeneous collection of blood with well-differentiated margins and appreciable diameter. They tend more frequently to be multiple, whereas intracerebral hemorrhage is a number of in solely 20% of instances. Hypodense areas round contusions and intracerebral hemorrhage are associated to low cerebral blood move. Cytotoxic substances are released from these contused areas in to the encircling tissue and blood stream. The formation of free radicals, excitatory amino acids and the altered homeostasis of Ca and K in these areas additional generate tissue damage. Some authors have argued that evacuation of those lesions could help to preserve extra vulnerable cerebral areas. Surgical evacuation of lesions in this space with evidence of basal cistern collapse is suggested to stop this complication. Contusions over silent areas ought to be broadly evacuated attempting to resect all devitalized tissue, whereas the resection must be more modest in these situated in eloquent areas. They might seem any time inside the first 24 hours, 50% may appear after the 24 hours and really not often after 7 days. Epidural hematoma is essentially the most frequent and the etiology is similar to the lesions seen in the supratentorial compartment. The presence of hydrocephalus ought to prompt suspicion of a lesion of the posterior fossa. Since epidural hematoma in this area tends to increase and cross the midline and tentorium, all efforts should be made to determine and management the source of bleeding. Subdural hematoma ought to be evacuated, and contused tissue, if current, additionally resected to obtain enough hemostasis. Compound depressed cranial fractures are depressed fractures with an overlying scalp laceration in continuity with the fracture site and galeal disruption, and have conventionally been treated with debridement and surgical elevation. Compound depressed fractures are neurosurgical emergencies, and they should be solved in the first 24 hours, ideally the primary 12 hours. If surgery is done within the first 24 hours, with out indicators of an infection and the dural may be closed in a watertight fashion, bone repositioning may be accomplished safely and the risk of infection is similar as when we remove the bone fragments [5]. Also, the presence of motor deficit, dural laceration and history of epilepsy may predispose to post-traumatic epilepsy. Most publications are retrospective research and only a few are pro- 650 Surgical Management of Severe Traumatic Brain Injury spective non randomized in design. Patients with worsening of the circulate pattern and the presence of systolic peak have the worst end result. As blood loss during craniectomy could additionally be essential, hemostasis is of great significance to avoid hypotension and secondary harm during the process. A duroplasty is at all times really helpful; autologous (galeal flap, temporal aponeurosis, facia lata aponeurosis) or heterologous (dural substitutes bovine, fibrillar, and so on. We choose to create two Condition Hemicraniectomy Yes yes No No Bicoronal No No Yes yes Midline shift Unilateral a quantity of contusions Bilateral diffuse cerebral edema Multiple bilateral contusions Table 35. The drawing shows the planned craniectomy for hemicraniectomy, bone of the fossa media to be eliminated (in grey) (A). As in hemicraniectomy, it could be very important resect the temporal bone as basal as potential. The bone bridge over the superior sagittal sinus averts pointless blood loss and helps for a less difficult craneoplasty surgical procedure posteriorly. Some authors propose resection of this bone bridge and cutting of the falx on the base of insertion, however we consider that is unnecessary. With sufficient bilateral publicity of the center fossa, it is extremely important to keep away from compression of the brainstem by the mesial facet of the temporal lobe. Intraoperative brain swelling it not commonly seen if the craniectomy is wide sufficient and timing is right. The swelling could also be additionally related to hyperperfusion phenomena, leading to intracerebral hematoma or cerebral infarction, particularly if the surgery is delayed; therefore, we suggest performing the process as soon as possible. The criteria for outlining whether a bicoronal or hemicraniectomy must be performed (Table 35. Immediate problems are a rise within the measurement of contusions or subdural hematomas, usually on the identical facet, and carry a poor prognosis if >20 cm3 in comparability with the 654 Surgical Management of Severe Traumatic Brain Injury preliminary lesions [19]. Another complication is cerebral herniation via the craniectomy (26% of cases), which may be brought on by hyperemia through the first days and associated with the lack of autoregulation. If the craniectomy is small, we may see one thing known as cerebral fungus, which is extensive herniation of the brain with vascular cerebral alterations of the mind via the borders of the craniectomy which worsen the situation. Paradoxal herniation is an indication of neurological deterioration with brainstem manifestations after a lumbar puncture in a decompressed patient and may happen days after the puncture; the mechanism is believed to be associated to an increase within the adverse pressure over the mind with the open cranium. It known as paradoxical as a result of the therapy is opposite to the administration of a classic herniation; the patient should be positioned in the Trendelenburg place and hyperosmolar answer must be stopped. Closure of ventricular or spinal drainage and even cranioplasty are all alternate options for the management of this situation. Some authors advise resolving the cranial defect earlier than beginning with surgical administration of the hydrocephalus. Another complication seen in this interval is the syndrome of the trephined characterised by headache, dizziness, irritability, reminiscence disturbances and mood modifications. And if the bone flap was preserved on the subcutaneous aircraft of the stomach with the thought of posterior reposition, 50% of partial reabsorption of the bone could happen if bone reposition is delayed. Since the instances are usually emergency surgery, the surgeon ought to be quick while guaranteeing pointless blood loss and situations of adequate asepsis. Guidelines for administration of severe head damage in adults: European Brain Injury Consortium. A randomized trial of very early decompressive craniectomy in kids with traumatic brain injury and sustained intracranial hypertension. The position of decompressive craniectomy in the treatment of post-traumatic intracranial hypertension. Safety and feasibility of craniectomy with duraplasty because the preliminary surgical intervention for extreme traumatic mind damage. Large decompressive craniectomy within the administration of extreme cerebral contusion: a review of 207 instances. Decompressive bifrontal craniectomy within the remedy of extreme refractory posttraumatic cerebral edema. Post-operative expansion of hemorrhagic contusions after unilateral decompressive hemicraniectomy in extreme traumatic brain injury.
Discount fluvoxamine 50 mg without prescriptionNevertheless, experimental and clinical studies have documented that ptbO2 monitoring after shock trauma is often a useful guide to enhance oxygen delivery. Studies by the Rotterdam group have clearly shown lower values of ptbO2 in nonsurvivors versus survivors in the course of the first 24 hours after injury [144]. Over the next days, nonetheless, there was no clear distinction in the common values between the groups. According to the Rotterdam research, low ptbO2 values are most frequently noticed through the first 24 hours after harm. In a series of a hundred sufferers, values <15 mmHg occurred in fifty seven sufferers, values <10 mmHg in 42, and values 5 mmHg in 22. It was subsequently suggested that this period may be characterized by "oxygen depression". In the 36-48-hours after harm, the average ptbO2 values increased to approximately 46 mmHg. This interval was due to this fact thought of to symbolize an "overshoot" probably as a end result of vasodilation secondary to the initial ischemia. Over the next days, the average tissue oxygen remained stable at round 30 mmHg and was thought of as the "stabilization stage". The three phases of evolution of brain tissue oxygen over time are summarized in Table 8. Further work is required to determine acceptable thresholds for initiating therapy to enhance cerebral oxygenation. Evolution over time is a extremely related issue and not all the time acknowledged in studies. We have found that an individualized evaluation may yield extra relevant insights. The Rotterdam group discovered no relationship between patient age and ptbO2, whereas the Robertson group did [15,136]. This distinction may be defined by the truth that they preferentially placed the probe within the penumbra of a damaged space, thus introducing bias towards older patients. The Stocchetti group described decrease mean ptbO2 in the pericontusional tissue (19. The prognostic worth of low ptbO2 values has been studied in multivariate logistic Regression evaluation. These studies confirmed an impartial prognostic effect of ptbO2; the chance of demise elevated 3. The native one was measured in the healthy brain, whereas the worldwide parameter was positioned in the broken mind. Lower ptbO2 values are additionally related to poorer cognitive functioning in survivors, leading to extra issues in work re-integration [149]. These outcomes clearly demonstrate an association between brain tissue hypoxia and elevated mortality and poorer end result in survivors [15, 142,144,150]. Thus, it will appear appropriate to forestall mind tissue hypoxia from occurring, and if it does, to right it rapidly. The correlation between hypoperfusion induced by bleeding and ptbO2 may be very shut. The first path tested the ptbO2 response on the preliminary 24 hours compared with the 72 hours response. The authors examined ptbO2 response solely on a imply of sixty two hours over time, ptbO2 increased 5 mmHg. Its practical efficacy will, nonetheless, be influenced by particular person components such because the time after damage and the degree to which autoregulation is disturbed [15,30,a hundred and forty,147,151]. The results from two research illustrate the time-dependency of the effectiveness of accelerating blood stress [30,147]. Increasing blood pressure with norepinephrine during the "melancholy stage" after harm produced a median enhance in ptbO2 of seven mmHg, with a 30% improve in imply arterial stress and improved cerebral perfusion. No data exist that specifically describe the response of ptbO2 to vasopressors in the course of the overshoot phase. The Cambridge group described an increase of 5 mmHg after vasopressors administration at seventy two hours after damage. Hypoxic areas of the mind will not be able to extracting adequate oxygen as a end result of oxygen diffusion gradients leading to a diffusion barrier [152]. Microvascular collapse and vascular edema might contribute to this diffusion barrier [153]. The efficacy of increasing blood pressure to improve ptbO2 may also depend on the diploma to which autoregulation is undamaged or disturbed [154]. Unfortunately, few circumstances have been studied through the crucial period of the first 24 hours. Further studies are needed to establish which affected person subgroups are at specific threat of ischemia and will likely respond to this remedy modality. The end result was different, with a mortality rate of 44% for the first group and 25% for the second. Despite the relatively small sample dimension and the dearth of a randomized design, the examine results help the concept of oxygen-targeted administration [155]. When contemplating whether or not to improve blood strain in order to enhance brain perfusion and oxygenation, consideration should be given to the selection of vasopressors. With norepinephrine a major reduction was observed in oxygen extraction (37�11 versus 33�12 ml/l) and a significant enhance in tissue pO2 (19. Response to the challenge test with dopamine was extra variable than with norepinephrine [101,103). The response was expressed as oxygen reactivity and related to consequence at 6 months. In a complete of 145 tests, the baseline ptbO2 ranged between 4 and 15 mmHg and the arterial paO2 between seventy three and 237 mmHg. After quarter-hour of 100% FiO2 administration, the ptbO2 elevated to a minimal of 9. We noticed three different patterns of response: response sort A was characterised by a pointy improve in ptbO2, reaching a plateau within a number of minutes; sample B by the lack of a plateau; and sample C by a short-duration plateau, adopted by a subsequent increase. Patterns characterised by a plateau (type A) were thought of to have extra stable regulatory mechanisms. This pattern observed in the first 24 hours after harm was associated with a more beneficial outcome (P=0. The association between higher O2 reactivity and poorer consequence could reflect more severe disturbances of autoregulatory mechanisms [126]. In one case, hyperoxia is a good treatment because it decreases the poisonous metabolites and promotes oxide reduction. Regardless of the absence of accredited therapeutic pointers, hyperoxia is used such as a "helmet" for mind protection, particularly in the initial 24 hours after trauma underneath ptbO2 monitoring. Pmean was increased to 23 mmHg and 40 mmHg progressively, oxygenation response was satisfactory: SjO2 from 43 to 85% and ptbO2 from 8 to forty mmHg. We suggest short durations (15-20 min) of hyperoxia (FiO2 100%) throughout resuscitation and as treatment for unexplained tissue hypoxia [59].
Purchase fluvoxamine 100 mg with visaA transverse incision is given in front of the elbow between the two epicondyles of humerus ii. A transverse incision is also given on the junction of upper and middle onethird of infront of forearm Boundaries Medially Lateral border of pronator teres. Before insertion, the bicipital aponeurosis extends downward and medially from the medial margin tendon of biceps. It is the smaller lateral terminal department of brachial artery and extra superficial than the ulnar artery ii. It is the brief department at the ulnar artery arising just distal to the radial tuberosity ii. It inclines downwards and backwards to the upper border interosseous membrane dividing in to anterior and posterior interosseous arteries. Anterior ulnar recurrent artery: It arises from the ulnar artery just distal to the elbow and ascends between the brachialis and pronator teres to reach in entrance of medial epicondyle of humerus. Common interosseous artery branch of ulnar artery, dividing in to anterior and posterior interosseous arteries. It passes backwards between the radius and ulna to be inserted radial tuberosity 4. It is bigger arises from the ulnar artery distal to the origin of anterior ulnar recurrent ii. It passes dorsomedially between the flexor digitorum profundus and superficialis to reach behind the medial epicondyle of humerus. It arises from the radial artery simply distal to the elbow, which ascends between the superficial and deep branches of radial nerve ii. It seems in the superolateral angle of brachioradialis and extensor radialis longus laterally carpi Dissection 647 ii. Opposite lateral epicondyle, it divides in to deep posterior interosseous nerve and superficial branch iii. The deep branch leaves the fossa by piercing the supinator and superficial branch passes downward deep to the brachioradialis. A transverse incision is given anterior to the wrist between the styloid processes of ulna and radius ii. Another transverse incision is given on the junction of upper onethird and center one third of the front of the forearm iii. A longitudinal incision is given becoming a member of the midpoints of the previous two incisions. Now the flaps of pores and skin mirrored on each side- Expose the superficial fascia, which contains the following constructions: a. Median cubital vein, it connect between basilic and cephalic veins close to the elbow d. Lateral cutaneous nerve of the forearm, which is the continuation of the musculocutaneous nerve. Incisions on Superficial Fascia Now superficial fascia is incised and mirrored like skin-deep fascia is uncovered. Bicipital aponeurosis, it extends in to the higher part of deep fascia of the forearm ii. Now deep fascia is cut and reflected like skin however as a result of attachments of the muscle tissue the deep fascia becomes lacerated during reflection. Identified Structures Muscles the muscular tissues of the front of forearm lie in three layers: i. Radial artery: It passes inferolaterally between the brachioradialis and flexor carpi radialis to reach the anterior floor of the lower end of the radius ii. Ulnar artery: Follow the ulnar artery to its origin from the brachial artery which is the bigger medial department and determine its major branches. Identify the pronator quadratus lies transversely between the anterior surfaces of the distal quarters of the radius and ulna Dissection 649 v. Anterior interosseous artery at the upper border of the pronator quadratus pierces the interosseous membrane to reach the extensor compartment vi. The interosseous nerve curves around the lateral aspect of the tendon of flexor digitorum superficialis and lies between it and the tendon of flexor carpi radialis deep to the tendon of palmaris longus vii. It enters the forearm through the posterior floor of the medial epicondyle of the humerus ii. It emerges on the lateral aspect of the tendon of the flexor carpi ulnaris near the pisiform bone v. Then the nerve passes together with the ulnar artery superficial to the flexor retinaculum and divides in to deep and superficial branches. Now establish the median nerve enters the forearm between the two heads of pronator teres ii. It lies between the flexor digitorum profundus and flexor digitorum superficialis iii. About 5 cm above the flexor retinaculum the nerve turn into superficial and lies between the tendons of flexor digitorum superficialis medially and flexor carpi radialis laterally v. Then the nerve passes deep to the flexor retinaculum via the carpal tunnel to enter the palm. A transverse incision is given in entrance of the wrist alongside the base of the thenar and hypothenar eminences (between the styloid processes of the radius and ulna respectively) ii. A longitudinal incision is given from the tip of the midpoint of the middle finger up to the center of the 1st incision iv. Another curved incision is given from the midpoint of the first incision up to the bottom of the thumb. Now, mirror the pores and skin in the following method Now the flap of pores and skin is reflected-now expose the superficial fascia. Palmaris brevis muscle current on the proximal a half of the hypothenar eminence iii. Cutaneous nerves: these are very tough to identify within the superficial fascia however these nerves are greatest identified once they pierces the deep fascia of their course: a. Extension of the anterior department of the lateral cutaneous nerve of the forearm, which reaches to the ball of the thumb b. Palmar cutaneous branch of the ulnar nerve which pierces the deep fascia anterior to the wrist c. Palmar cutaneous branch of the median nerve pierces the deep fascia simply above the wrist and provide the lateral twothirds of the palm of pores and skin. Now, take away the superficial fascia and expose the deep fascia, which is skinny on the thenar and hypothenar eminences however in between them the deep fascia is thickened to kind the palmar aponeurosis. The palmaris brevis muscle which is a thin cutaneous muscle arises from the flexor retinaculum and palmar aponeurosis passes over the proximal 23 cm. Follow the palmar aponeurosis, which is proximally steady with the deep fascia of forearm and the palmaris longus. Between it and the long flexor tendons lie the branches of the median and ulnar nerves iii.
Purchase fluvoxamine cheapMultiple components modify water Recommended doses Nitrogen (g/kg/day) losses, such as high-protein diets, fever, polyuria, vomiting and kidney failure. Vitamin requirements could also be affected by adjustments in food regimen, use of some drugs, ailments corresponding to malnutrition, sepsis and trauma, and artificial nutrition, primarily parenteral diet. The deficit of the water-soluble vitamins occurs more simply as a result of the fat-soluble nutritional vitamins are stored within the body and have a slower turnover (Table 20. Vitamin B12 must be taken 2 or 3 times a week and at very broad intervals thereafter. Fat-soluble vitamins should be administered as soon as per week and vitamin K twice every week. These substances are involved in a quantity of cellular features and various enzyme techniques. Daily requirements Electrolite Sodium (Na+) Chlorus (Cl-) Kalium (K+) Calcium (Ca++) Phosphorus (P) - 1-2 mEq/kg 1-2 mEq/kg 0. A primary form of therapy, synthetic nutrition plays an necessary role in the complete care of critically unwell sufferers since a dietary deficit can interact with the illness and extend the therapeutic process or have devastating penalties. The routes of administration are enteral diet and parenteral vitamin, discussed under. During the course of important illness, the gut virtually at all times stays inactive because of ileus or other frequent issues that prevent feeding and require nasogastric aspiration. Besides its function in the digestion and absorption of nutrients, the intestine also acts as an enteral flora barrier which prevents host invasion by microorganisms or their toxins. In patients who obtain no food or vitamins in to the digestive tract, the intestinal mucosa become more permeable to the passage of germs and their merchandise in to the bloodstream, resulting in chronic hypermetabolism and multiple organ failure. Volumes of 200 to four hundred ml four to 6 occasions a day can cause nausea, vomiting, diarrhea, cramps and bloating, with a excessive risk of aspiration. Intermittent administration is given in small quantities of 80 to 160 ml from 20 to 30 minutes each hour; nevertheless, tolerance is poor in some sufferers and the approach is impractical since it occupies lots of nursing staff time. An alternative way to be used in patients requiring extended enteral nutrition includes steady administration of enteral solutions at a rate of 160 ml/hour for 12 hours. Isotonic options ought to be began at an infusion price of 50 ml/ hour, after which progressively elevated, as tolerated, as much as eighty ml/hour. If intolerance develops, the volume or concentration of the diet should be reduced to the previous degree of tolerance, and then elevated after enough time for adaptation has elapsed. Wherever potential, regulators must be outfitted with a flow or infusion pump to reduce the chance of insufficient volumes, resulting in less bloating and diarrhea, lower residual volume and less danger of aspiration. The volume ought to be elevated every 24 to 48 hours until it covers the entire nutritional requirement with an intermittent bolus of 300 to 400 ml each, each 3 to four hours. The gastric residual should be managed earlier than each administration and administration discontinued if it is >150 ml. The affected person ought to be rechecked after 2 hours and feeding could be restarted if the gastric residual is less than the acknowledged worth. This route of administration of nutrients is in all probability not utilized in neurocritical sufferers because of the chance of aspiration. The tube should be placed distal to the Treitz ligament to lower the risk of aspiration. The approach for tube placement could also be blind (high failure rate) or by endoscopy, fluoroscopy or ultrasound-guided. The use of prokinetic agents facilitates, a minimum of in theory, the passage of the pylorus, regardless of the approach. Also, these tubes can be positioned by invasive methods similar to endoscopic percutaneous jejunostomy, radiological percutaneous jejunostomy and traditional surgery or by laparoscopy. Use of enteral nutrition, primarily jejunal nutrition, is suitable for early postoperative feeding, is safe and effective, as intestinal paralysis is predominant within the stomach and colon, and in addition it causes poor pancreatic stimulation. Bolus administration of hyperosmolar solutions within the small gut may cause bloating, diarrhea and electrolyte disturbances. To keep away from these antagonistic results, volumetric pumps can be used and solutions with half of the specified concentration should be started at infusion rate of fifty ml/hour. The focus of the options should be increased till the whole osmolality of the nutritional formulation is obtained. The most important limiting consider intolerance to the food plan is the osmolar load (intake per unit time) received by the digestive tract, so a gradual enhance in the infusion price, 410 Nutritional Support in Critically Ill Patients but not the focus of the formulation, is recommended, whereas sustaining a caloric density of 1 kcal/ml. Accordingly, protocols has been devised beneath which the amount must be 20 ml/hour for the first 6 hours and then incremented by 10 ml/hour every 6 hours until the desired volume is reached, or to start with 20 ml/hour for eight hours with increments of 20 ml/ hour each 8 hours until the infusion price matches the necessities. If the patient develops diarrhea, and antidiarrhetic may be given, but when it persists or other antagonistic results arise, feeding must be suspended for 48 hours. The presence of abdominal distention, diarrhea or other unwanted aspect effects have to be checked periodically. Homogenized diets are ready with natural foods under technical homogenization; they differ from regular meals only in consistency and method of administration via a catheter. These diets are prepared from milk, yogurt and ice cream, and other nutrients are added. Milk-based diets use milk as the primary protein supply and different sources of protein like eggs are added; energy are offered as lactose, dextrins, milk fat and soybean or corn oil. They are poorly tolerated in patients with disaccharidase deficiency and may cause diarrhea. Nonproteic energy are supplied as oligosaccharides from glucose, dextrin and fats derived from soybean or corn oil. These diets are helpful in sufferers with lactase deficiency, have low viscosity, and may be administered by way of small-calibre tubes. Nutritionally complete diets can be normal in protein, with a protein intake <20% of complete calories, or excessive in protein, which contain 20% or extra protein in relation to the provision of energy. They encompass carbohydrates as oligosaccharides, sucrose and glucose, short-chain peptides (oligopeptides) or L-amino acids and medium-chain fatty acids, and small quantities of essential fatty acids and vegetable oils. These components trigger little gastric residue and small intestinal contents, which scale back the frequency of bowel actions and reduce colonic bacterial flora. They have a calorie density of 1 kcal/ml, cut back gastric acid secretion, however are costly. They could additionally be helpful in patients with lowered inte411 Intensive Care in Neurology and Neurosurgery stinal absorption surface and in these with impaired digestion or absorption ability. They have excessive molecular density and could additionally be helpful in patients who require fluid restriction. Diets for particular conditions have been created to cover the dietary wants in particular illnesses. In addition, there are immuno-enriched diets with arginine or omega 3 fatty acids and diets enriched with glutamine which is concerned in intestinal barrier integrity. Because of the vast variety of formulas for enteral nutrition, the food plan composition and the proportion of different nutrients in the formulation must be reviewed before use. Mechanical Complications Mechanical complications are related to tube placement and maintenance, tube type and its anatomical place: They may be related to nasoenteral tubes; for example: � Misplacement of the tube in the pharynx, esophagus, airways and lungs increases the danger of aspiration.

Buy discount fluvoxamineIt has been proposed that a cardiac to respiratory wave amplitude ratio >2 signifies cerebral vasodilation, while a lower ratio is indicative of increasing elastance. The Lundberg A wave, also known as a plateau wave, persists for 5 to 20 minutes at amplitudes of 50 to one hundred mmHg. Lundberg B waves are moderately elevated to about 50 mmHg and persist solely over 30 seconds to a few minutes. Lundberg C waves happen approximately 6 to 10 instances a minute and have amplitudes of 20 mmHg. When elastance is excessive, hypercarbia or different maneuvers that cause cerebral vasodilation can produce plateau waves. Since ischemia is often related to Lundberg A waves, they may be associated with everlasting cerebral harm. In this situation, the proper atrial stress and the superior vena cava stress each improve and venous outflow from the brain is lowered. Familiarity with the forms of screens obtainable and recognition of waveforms and their patterns may help the clinician to troubleshoot the technical problems that occur throughout monitoring and to detect worsening of edema. J Neurotrauma 2007; 24(Suppl 1): S37-S44 Broderick J, Connolly S, Feldmann E, et al. Guidelines for the administration of spontaneous intracerebral hemorrhage in adults: 2007 replace. The influence of intraabdominal hypertension on the central nervous system: present insights and scientific suggestions, is it all within the head Traumatic cerebral vascular harm: the results of concussive mind injury on the cerebral vasculature. Continuous recording and control of ventricular fluid strain in neurosurgical practice. In the developed nations, preventive measures, schooling, organization of well being care and treatment based mostly on invasive and non-invasive monitoring have decreased morbidity and mortality [4-7]. In some developing countries, improvements have come about only in some specialised centres mainly via the higher organization of health systems and from the prevention and correction of widespread secondary injury components corresponding to hypotension and hypoxia [2,eight,9]. The implementation of intracranial stress monitoring is really helpful in severely injured patients. Attempts to introduce new monitoring methods to consider blood flow and metabolism, such as cerebral oxygenation, are met with even higher controversy [14-17]. In a submit mortem neuropathological research, Teasdale and Graham [20,21] described diffuse axonal harm in 92% of cases, hypoxic damage in 54%, focal lesions in 94% and congestion in 28%. There is urgent need for a extra multimodal method to seize and monitor the disease profile [17,25]. Some report on remedy response, however few build on previous expertise, for instance, taking the time curve in to consideration [16,30,31]. Nor did they relate therapy thresholds to the identified profiles of ptbO2 development differentiation underlying the causes of low oxygen rigidity values [16,31]). The interpretation of findings and the way these are translated in to medical practice for the person affected person is due to this fact relevant when evaluating the cost-benefit ratio of this monitoring system. Compared to research from the developed countries, several conducted in Latin America reported that ptbO2 monitoring showed the next prevalence of secondary injury elements [33-37]. Outcome improved [34-37] however to not the same level as in the most experienced centres [16,17]. It is unknown whether or not the improved consequence noticed after the introduction of brain tissue oxygen monitoring within the growing countries is attributable to a extra cohesive group effort and a spotlight to care or to particular treatment targets. Whatever the cause of the decline in mortality, the experience of the growing countries is adequate to motivate the purchase of monitoring equipment. Greater familiarity with multimodality monitoring can information the therapeutic choices by neurosurgeons and intensivists along the time evolution curve and monitoring tendencies, no matter clinical grade or sedation stage. We will define which requirements of analysis of ptbO2 may help us to define better therapy approaches. We may also review new areas of utility, limitations, and briefly focus on the position of native measurement approaches, similar to ptbO2, in relation to extra world approaches, similar to jugular oximetry. In world monitoring, oxygen saturation is measured in cerebral venous blood via continuous or intermittent monitoring of SjO2 (jugular bulb oxyhemoglobin saturation) and derived parameters. The most typical method for regional monitoring is to measure the mind oxygen rigidity (ptbO2). The purpose of worldwide monitoring (SjO2) is to guarantee basic cerebral oxygenation. The starting "hyperemia" peak (SjO2 >85%) is expounded to psychometric agitation and ought to be read in relation to median arterial pressure. According to the saturation curve of hemoglobin and oxyhemoglobin at the venous end, a partial pressure of oxygen of forty torr corresponds to a saturation of 75% [42]. The frequent incidence of artefacts and the broad variability in venous drainage of the mind produce inconsistencies within the values mea171 Intensive Care in Neurology and Neurosurgery sured and reduce the reliability of SjO2 measurements [43]; nonetheless, the knowledge derived from SjO2 measurement can be helpful in neurocritical care. It is crucial that the catheter be positioned (and maintained) within the jugular bulb, as placement in a extra proximal position can contaminate it with extracerebral venous blood, making values inaccurate and non-representative of the cerebral condition. Such inferences are legitimate solely when the rate of oxygen consumption and transport, the amount of dissolved oxygen in the blood, the hemoglobin level, and the degree of decoupling of the saturation curve of hemoglobin are all secure [42,46]. The international cerebral oxygen status in healthy people displays the stability between oxygen supply and demand and relies on cerebral blood move and metabolism. Although calculating AjO2 provides detailed information, drawing blood entails a heavy workload, so steady SjO2 monitoring is preferable. In abstract, the SjO2 may be influenced by many variables concerned in international oxygen supply and consumption. It displays the stability between cerebral oxygen supply and metabolic price when oxyhemoglobin saturation, hemoglobin concentration and the hemoglobin dissociation curve stay fixed. A decrease in SjO2 displays a lower in oxygen supply to the brain or elevated metabolic exercise. Any disturbance that will increase the demand or decreases the oxygen provide could lower SjO2. In distinction, extended AjO2 with SjO2 <65%, corresponds to a hypodynamic state, with pump failure and in depth extraction [56]. Increased sedation could additionally be appropriate if ranges are considered insufficient to cut back agitation [59,60]. It is really helpful to calibrate the SjO2 monitor with the co-oximeter every 6 hours when modifications in SjO2 occur and previous to initiating therapeutic changes. With the quick and inexplicable fall of SjO2, blood was extracted and SjO2 modified. The period of monitor disconnection reveals ptbO2 reliability and recalibration of SjO2 (registered between 12. The repercussion in ptbO2 was evident; ptbO2 decreased by 5 mmHg with an related reaction in SjO2. Blood strain control turns into critical at this second to have the ability to limit the development of vasogenic edema. The sustained rise in SjO2, with increased perfusion strain during and after suctioning, suggests disturbed vascular autoregulation [67]. A whole of 2799 samples had been taken from 450 patients within the first 5 days after trauma. In this study, SjO2 >75% was not clearly associated with hyperemia, though some authors think about it a major cause of intracranial hypertension [70,71].
References - Bannister CF, Brosius KK, Wulkan M: The effect of insufflation pressure on pulmonary mechanics in infants during laparoscopic surgical procedures, Paediatr Anesth 13(9):785-789, 2003.
- Otto EA, Loeys B, Khanna H, et al: Nephrocystin-5, a ciliary IQ domain protein, is mutated in Senior-Loken syndrome and interacts with RPGR and calmodulin, Nat Genet 37:282n288, 2005.
- Gurdal H, Sara Y, Tulunay FC: Effects of calcium channel blockers on formalininduced nociception and inflammation in rats, Pharmacology 44:290n296, 1992.
- Vainio S, Lehtonen E, Jalkanen M, et al: Epithelial-mesenchymal interactions regulate the stage-specific expression of a cell surface proteoglycan, syndecan, in the developing kidney, Dev Biol 134(2):382-391, 1989.
|
|