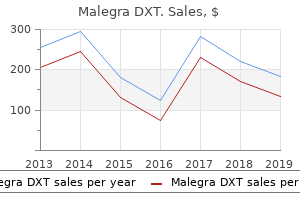
"Order malegra dxt overnight, impotence research."By: Joshua C Briscoe, MD - Medical Instructor in the Department of Psychiatry and Behavioral Sciences
- Medical Instructor in the Department of Medicine
 https://medicine.duke.edu/faculty/joshua-c-briscoe-md
Purchase discount malegra dxt onlineThe presence of noxious stimulation will increase the requirements of propofol and remifentanil to achieve the identical degree of sedative results. When mixed, their effect on respiration is strikingly synergistic, leading to extreme respiratory melancholy. The optimal concentrations vary outcomes from the intersection between the well-being floor and the aircraft representing a well-being value of zero. Response to intubation (blue line), upkeep of anesthesia (gold line), and concentrations associated with emergence from anesthesia (green line). The curve shows the concentrations related to a 50% likelihood of the respective endpoint. The pharmacodynamic interaction of propofol and alfentanil throughout decrease belly surgery in girls. However, blocking the response to esophageal instrumentation and avoiding both intolerable ventilatory melancholy and/or a loss of responsiveness is difficult. It could additionally be essential to accept some discomfort and blunt, rather than block, the response to esophageal instrumentation to constantly avoid insupportable ventilatory despair and/or lack of responsiveness. The interactions between hypnotics such as propofol and sevoflurane must also be understood, as a end result of these medication are regularly used sequentially. LaPierre and coworkers100 explored remifentanil-propofol combos that led to a loss of response to esophageal instrumentation, a lack of responsiveness, and/or an onset of ventilatory melancholy requiring intervention. They found that the combos that allowed esophageal instrumentation and averted intolerable ventilatory despair and/or loss of responsiveness primarily clustered around remifentanilpropofol effect-site concentrations starting from 0. The definition of focus could be rearranged to discover the amount of drug required to produce any desired concentration for a identified volume (Eq. Downward deflection of the surface represents synergy, in units of fractional discount in C50. The three edges characterize relative amounts of propofol to midazolam (Mid-prop), alfentanil to midazolam (Mid-alf), and alfentanil to propofol (Alf-prop). The surface between the sides represents the relative synergy of all three medication taken together. The isoboles for a 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, and 90% response are proven. This formulation is usually used to calculate the initial (loading) bolus dose required to achieve a given concentration. The drawback with making use of this concept to anesthetic drugs is that there are a number of volumes of distribution: V1 (central compartment), V2 and V3 (the peripheral compartments), and Vdss (the sum of the person volumes). Consideration must be given to the dose of fentanyl required to attenuate the hemodynamic response to endotracheal intubation when mixed with thiopental. The C50 for fentanyl, combined with thiopental for intubation, is roughly three ng/mL. A fentanyl bolus of 39 g achieves the desired concentration in plasma for an initial prompt, but plasma ranges virtually immediately lower below the desired target. Additionally, utilizing equations to calculate the fentanyl dose if the ensuing recommendation is to "use a fentanyl dose between 39 and 1080 g" is absurd. The ordinary dosing tips for a bolus dose, introduced earlier, are designed to produce a specific plasma focus. By knowing the ke0 of an intravenous anesthetic, a dosing routine can be designed that yields the specified focus on the web site of drug effect. To avoid an overdose for the affected person, a bolus ought to be selected that produces the specified peak concentration on the impact web site. The decline in plasma concentration between the preliminary concentration after the bolus (amount/V1) and the concentration at the time of peak impact can be regarded as dilution of the bolus into a larger anatomic quantity than the volume of the central compartment. This introduces the idea of Vdpe, the apparent volume of distribution on the time of peak effect,28,ninety four or pseudoequilibration between plasma and the site of drug effect. If the clinical goal is to choose the dose required to achieve a sure drug effect with out producing an overdose, then Eq. This dosing guideline is more cheap in contrast with the previous suggestion of a dose between 39 and 1080 g. These infusion schemes had been designed to obtain a fentanyl plasma focus (Cp) of three ng/mL. The higher blue curve exhibits that a routine utilizing a loading dose primarily based on the amount of distribution adopted by a continuing infusion primarily based on clearance ends in a transient interval of very excessive plasma concentrations. If the identical maintenance infusion is given however the loading dose relies on the quantity of the central compartment, then the distribution of drug to the peripheral compartments causes the plasma focus to fall beneath the desired level till the compartments attain steady-state concentrations as shown within the lower gold curve. The rate of distribution into tissues changes over time because the tissues equilibrate with plasma. At all other times, this upkeep infusion price underestimates the infusion price essential to preserve a goal concentration. Yet in some conditions, this easy upkeep fee calculation could additionally be acceptable. For example, if an infusion at this fee is used together with a bolus dose based mostly on Vdpe and the drug has a long delay between the bolus and peak effect, then a lot of the distribution of drug into tissues could have occurred by the time that the effect-site concentration reaches the goal concentration. In this case, the upkeep infusion fee calculated as clearance occasions goal concentration may be accurate as a outcome of Vdpe is sufficiently larger than V1 to account for the distribution of drug into peripheral tissues. Because the online move of drug into peripheral tissues decreases over time, the infusion fee required to preserve any desired focus must additionally decrease over time. If the initial bolus has been based mostly on 26 � Intravenous Drug Delivery Systems 765 Vdpe, no infusion wants be administered until the effect-site focus peaks. After the height in effect-site focus, the (nearly) correct equation to keep the specified concentration is (Eq. Few clinicians would choose to solve such an equation through the administration of an anesthetic. Fortunately, easy techniques can be utilized rather than solving such a posh expression. Of course, choosing goal concentrations and totally different instances of rate adjustment is possible, depending on the medical circumstances and an assessment of how accurately the intravenous drug needs to be titrated. Infusion Rates to Maintain Stable Plasma Concentrations 5 four Fentanyl (ng/mL) 3 2 1 Suggested preliminary goal 6. The diagonal traces present the infusion charges at different times required to maintain the desired focus selected on the y axis. Although the terminal elimination half-life is commonly interpreted as a measure of how short- or long-lasting a drug is, the speed at which drug plasma concentration decreases is dependent on both elimination and redistribution of the drug from the central compartment. The contribution of redistribution and elimination towards the speed of decrease in drug concentration varies based on the duration for which the drug has been administered108,109 and likewise the time for the reason that infusion has stopped, as a outcome of these processes have completely different rate constants. In 1985, Schwilden110 developed a mathematic mannequin to relate the time course of offset of motion of inhaled anesthetics to the length of anesthetic drug supply.
Buy malegra dxt 130 mgEndotracheal tube as a information for an Eschmann gum elastic bougie to help tracheal intubation using the McGrath or GlideScope videolaryngoscopes. Macintosh blade videolaryngoscopy mixed with rigid Bonfils intubation endoscope offers an acceptable various for patients with tough airways. Elective use of the ventrain for upper airway obstruction throughout high-frequency jet ventilation. The pace of neural blockade is dependent upon the dimensions, floor area, and degree of myelination of the nerve fibers uncovered to the local anesthetic. Blockade of the peripheral (T1-L2) and cardiac (T1-T4) sympathetic fibers is responsible for the decrease in arterial blood strain (cardiac output and systemic vascular resistance) related to neuraxial techniques. Cerebrospinal fluid quantity and native anesthetic baricity are an important determinants for the spread. The use of smaller-gauge spinal needles decreases the incidence of post�dural puncture headache. Serious neurologic problems related to neuraxial blockade are rare, but the danger will increase within the aged and people with preexisting spinal pathology. The use of low-molecular-weight heparin and potent platelet inhibitors increases the chance of epidural hematoma from neuraxial blockade. Epidural blood patches are higher than 90% efficient in relieving post�dural puncture headache. Local anesthetic systemic toxicity results from unintentional administration of the drug into an epidural vein. Use of neuraxial blockade, significantly when used as the solely real anesthetic, can reduce perioperative morbidity and will cut back mortality. Principles Spinal, epidural, and caudal neuraxial blocks end in one or a combination of sympathetic blockade, sensory blockade, or motor blockade depending on the dose, focus, or quantity of native anesthetic administered. Despite these similarities, there are important technical, physiologic, and pharmacologic differences. In distinction, epidural and caudal anesthesia progress more slowly (>20 minutes) after a big mass of local anesthetic that produces pharmacologically energetic systemic blood levels, which can be associated with side effects and problems unknown to spinal anesthesia. The introduction of mixed spinal and epidural methods blurs a few of these differences, but additionally adds flexibility to clinical care. Continuous catheter-based epidural infusions of dilute local anesthetics and opioids are used for obstetric labor analgesia and postoperative pain relief after main surgical procedure. Evidence demonstrating that epidural analgesia can scale back pulmonary morbidity and mortality in high-risk sufferers undergoing major thoracic and belly surgery served to propel the practice of epidural analgesia at the beginning of the millennium. Indwelling spinal catheters may be applied long run (from months to years) for the remedy of persistent malignant and nonmalignant ache. Historical Perspectives the first case of spinal anesthesia in people was performed by August Bier in 1898 utilizing the native anesthetic cocaine. Spinal anesthesia utilizing ropivacaine and levobupivacaine was launched in the Nineteen Eighties. The yr 1901 marked the primary reported use of intrathecal morphine described by Racoviceanu-Pitesti, in addition to the first description of caudal anesthesia reported by Cathleen. Lumbar epidural anesthesia in humans was first described by Pag�s in 1921, the loss-of-resistance technique by Dogliotti within the Thirties, steady caudal for obstetrics by Hingson in 1941, and lumbar epidural catheterization for surgery by Curbelo in 1947. Despite the extensive experience using neuraxial methods throughout the past century, a number of events caused major setbacks alongside the method in which, together with the Woolley and Roe case detailing paraplegia after spinal anesthesia in 1954,four the reviews of persistent neurologic deficits and adhesive arachnoiditis with spinal chloroprocaine in the early Nineteen Eighties, and cauda equina syndrome with continuous spinal lidocaine anesthesia within the early Nineties. This distal termination varies from L3 in infants to the decrease border of L1 in adults due to differential growth charges between the bony vertebral canal and the central nervous system. The pia mater is a highly vascular membrane that intently invests the spinal wire and brain. Surrounding the dura mater is the epidural house, which extends from the foramen magnum to the sacral hiatus and surrounds the dura mater anteriorly, laterally, and posteriorly. The epidural house is sure anteriorly by the posterior longitudinal ligament, laterally by the pedicles and intervertebral foramina, and posteriorly by the ligamentum flavum. Contents of the epidural area include the nerve roots and fat, areolar tissue, lymphatics, and blood vessels together with the well-organized Batson venous plexus. Posterior to the epidural space is the ligamentum flavum (the so-called yellow ligament), which extends from the foramen magnum to the sacral hiatus. Ligament thickness, distance to the dura, and skin-to-dura distance vary with the realm of the vertebral canal. The two ligamenta flava are variably joined (fused) within the midline, and this fusion or lack of fusion of the ligamenta flava occurs at totally different vertebral levels in individual patients. There are 7 cervical vertebrae, 12 thoracic vertebrae, 5 lumbar vertebrae, and a sacrum. The vertebrae are joined together anteriorly by the fibrocartilaginous joints with the central disks containing the nucleus pulposus, and posteriorly by the zygapophyseal (facet) joints. The thoracic spinous process is angulated steeply caudad versus the virtually horizontal angulation of the lumbar spinous process. This is a clinically necessary distinction for needle insertion and advancement within the thoracic versus lumbar ranges. The sacral canal incorporates the terminal portion of the dural sac, which usually ends at S2. Variation is discovered in this feature as nicely, with the termination of the dural sac being lower in youngsters. In addition to the dural sac, the sacral canal incorporates a venous plexus, which is a part of the valveless internal vertebral venous plexus. The volume of the caudal canal in adults, excluding the foramina and dural sac ranges, is about 10 to 27 mL. The anterior and deep portion of the cord (gray matter) is most prone to ischemia (leading to anterior horn motor neuron harm, or anterior spinal syndrome) as a result of there are fewer anterior medullary feeder vessels than posterior feeder vessels. Likewise, the midthoracic part of the spinal cord (from T3 to T9) is most in danger where segmental medullary feeder vessels are rare. Venous drainage of the spinal twine follows an identical distribution because the spinal arteries. There are three longitudinal anterior spinal veins and three posterior spinal veins that talk with the segmental anterior and posterior radicular veins earlier than draining into the internal vertebral venous plexus in the medial and lateral elements of the epidural area. These differences might assist to clarify the interpatient variations in neuraxial block quality when equivalent techniques are used on seemingly related patients. Another anatomic relationship could affect neuraxial blocks; although generally bigger than the ventral (motor) roots, the dorsal (sensory) roots are sometimes blocked extra simply. This obvious paradox is defined by group of the dorsal roots into component bundles, which creates a much bigger floor area on which the native anesthetics act, possibly explaining why larger sensory nerves are blocked more simply than smaller motor nerves. Another research by Hogan18 has additionally shown in cadavers that the spread of answer after epidural injection into the tissues of the epidural space is nonuniform, and he postulated that this accounts for the clinical unpredictability of epidural drug unfold. There is evidence that adipose tissue in the epidural house diminishes with age,19 and this decrease in epidural space in adipose tissue might dominate the age-related changes in epidural dose necessities (see Chapter 65). Mechanism of Action Local anesthetic binding to nerve tissue disrupts nerve transmission, resulting in neural blockade. For spinal and epidural anesthesia, the goal binding sites are positioned throughout the spinal wire (superficial and deep portions) and on the spinal nerve roots in the subarachnoid and epidural areas.

Order malegra dxt overnightIn clinical research comparing potencies of ropivacaine and bupivacaine administered for brachial plexus124 or lumbar epidural block,one hundred twenty five the anesthetic profiles of the medicine were almost identical. In some laboratory animal research and in some human research, ropivacaine also produced blocks of shorter period than these induced by bupivacaine. Other research in animals and humans have found equal durations of sensory and motor block for the 2 medication. Studies in animals have typically found that bupivacaine more readily produces conduction disturbances, cardiac collapse, or ventricular fibrillation than ropivacaine does and that aggressive cardiac resuscitation after an intentional intravenous bolus in canine results in efficient reversal of the toxic results far more frequently with ropivacaine than with bupivacaine. In contrast to bupivacaine, the cardiotoxic profile of ropivacaine in pregnant ewes is the same because the corresponding profile in nonpregnant ewes. Although a quantity of publications have in contrast levobupivacaine with racemic bupivacaine and ropivacaine,129,one hundred thirty conclusions differ amongst research relating to the relative efficiency and length of block of those three drugs at completely different websites of administration with respect to sensory and motor end factors. Clinicians should notice that levobupivacaine is formulated as a weight share with regard to its free base content, whereas the load proportion of most other native anesthetics is calculated on the basis of the hydrochloride salt. Indirect Cardiovascular Effects High ranges of spinal or epidural blockade can produce severe hypotension. A follow-up research of closed claims of patients who suffered perioperative cardiac arrest confirmed earlier stories of a sequence of cardiac arrests involving typically healthy patients present process spinal or epidural anesthesia. Whereas delicate to average degrees of hypotension usually reply well to indirect-acting sympathomimetics similar to ephedrine or incremental dosing of phenylephrine, the mixture of extreme hypotension and severe bradycardia under spinal anesthesia should in most clinical settings be handled promptly with incremental dosing of epinephrine, initially at doses of 0. Hepatic metabolism of prilocaine generates O-toluidine, which oxidizes hemoglobin to methemoglobin. Methemoglobinemia, if severe, may be treated by the intravenous administration of methylene blue. Risk may be elevated in newborns with uncommon metabolic disorders or after the concomitant administration of different medicine that impair reduction of methemoglobin. Aminoesters, not like aminoamides, are derivatives of p-aminobenzoic acid, which is understood to be allergenic. Hypercapnia, 29 � Local Anesthetics 887 methylparaben, whose chemical structure is much like that of p-aminobenzoic acid, however for most aminoamides, preservative-free solutions can be found. In the very rare patient for whom confirmed allergy to both aminoamides and aminoesters precludes their use for spinal anesthesia, meperidine may be thought of in its place. Thus the appliance of 5% (200 mM) lidocaine in viscous, dense options via slender intrathecal catheters had been associated with a high frequency of transient or longer-term radicular signs or even cauda equina syndrome. If cauda equina syndrome was thought of one catastrophic finish of the spectrum, the alternative side would be transient neurologic syndrome, a brief radicular irritation thought to be brought on by native anesthetic software and influenced by patient positioning. Differences in examine design, method of questioning, and criteria for inclusion could also be partially answerable for differences within the prevalence of radicular sequelae in numerous studies. Despite these differences in examine design, a meta-analysis concluded that the pooled relative risk for transient neurologic symptoms after spinal anesthesia with lidocaine was 6. Development of ProlongedDuration and Sensory- or Nociceptive-Selective Local Anesthetics Several strategies for producing long-duration nerve blockade are beneath investigation. First, there have been efforts to use readily available drugs such as tricyclic antidepressants149,one hundred fifty or quaternary local anesthetic derivatives as novel local anesthetics,151 but these efforts have constantly been hampered by concerns over neurotoxicity. Liposomal bupivacaine (Exparel) has been licensed for infiltration analgesia152 but its dose-response for blockade of peripheral nerves is less clear. Other modes of slow-release are embedding in bone wax, polylactic acid, polyglycolic acid, fatty-acid-based biodegradable polymers, and proliposomal formulations. Yet, the concept of targeting specific variants of native anesthetic medicine into specific fibers has been confirmed, and if a mixture of medicine is found which can provide these effects with decreased neurotoxicity, the technique as such could hold promise. Whether any quaternary derivatives of local anesthetics have less neurotoxicity than their mother or father compounds remains as of but unanswered. To summarize, a number of avenues of research may result in new native anesthetics or new modes of utility, however solely liposomal bupivacaine has been launched into scientific practice. Potentially, these new methods might transfer us nearer to the holy grail of regional anesthesia, the place patients benefit from a tailor-made surgical block followed by extended periods of reliable sensory (or even nociceptive) block with out impairment in motor function. Biologic Mechanisms of Local Anesthetic Failure: Inflammation, Hyperalgesia, Tachyphylaxis, and Genetic Variants Failure of native anesthesia is usually ascribed to technical failure of delivery, insufficient volume or concentration of drug, or faulty clinical decisions in number of strategies. However, there are a number of medical conditions by which biologic processes contribute to failed native anesthesia, even with proper technique and drug choice. For instance, in sufferers going to the dentist with infections corresponding to a tooth abscess or severe pulpitis, failure rates of standard doses of local anesthetic have been reported to be as excessive as 70%. Local anesthetic failure at a web site of irritation appears to mirror a combination of pharmacokinetic factors and pharmacodynamic factors. Pharmacokinetic elements include (1) increased local blood move leading to accelerated elimination of drug from perineural injection compartments; (2) local tissue acidosis resulting in a greater proportion of the drug in the hydrochloride kind, which diffuses extra poorly across biologic membranes; and (3) native tissue edema, which will increase diffusion distances for drug into nerves. Pharmacodynamic elements embody the results of irritation on each peripheral sensitization of nerves and central sensitization. Increasing the concentration of native anesthetic can nonetheless lead to satisfactory, albeit shorter, blockade. In scientific apply, these patients require a better native anesthetic dose to obtain enough analgesia. Apparent reductions within the effectiveness of native anesthetic infusions over time could additionally be as a outcome of a selection of causes unrelated to tolerance per se, including dislodgement of catheters and modifications in the dermatomal origin or depth of nociceptive enter. In obstetric patients receiving epidural bolus injections, recurrence of pain earlier than the next injection resulted in a discount within the depth and length of blockade, whereas repeat injection earlier than the return of pain prevented this quickly occurring type of tolerance, or tachyphylaxis. In a rat model, tachyphylaxis was linked to the development of hyperalgesia,162 and drugs that inhibit hyperalgesia, together with N-methyl-d-aspartate receptor antagonists and nitric oxide synthase inhibitors,163 also prevented tachyphylaxis. Conversely, repeated sciatic injections of lidocaine resulted in lowered intraneural lidocaine content along with reduced period of block. This is supported by a medical study which showed that some p.c of individuals reporting inefficient regional anesthesia really did reveal partial resistance when examined in standardized method, and a few sufferers had selective resistance against specific local anesthetics. Interesting case reviews suggest that repeated exposure to scorpion bites can elicit acquired resistance to local anesthetics. Conclusions Local anesthetics have been a central pillar in perioperative management of patients for greater than a century, and continued research will assure that we all know as much as potential about these drugs, and how we will use them as optimally as possible for the good thing about the patients whose care has been entrusted to us. Gary Strichartz for his contribution to this chapter within the prior edition of this work. Tetracaine-membrane interactions: effects of lipid composition and part on drug partitioning, location, and ionization. Structure-activity relations for frequency-dependent sodium channel block in nerve by local anesthetics. Phenotype and function of somatic main afferent nociceptive neurones with C-, Adelta- or Aalpha/beta-fibres. The science of native anesthesia: basic analysis, medical software, and future instructions. Differences in quantitative architecture of sciatic nerve could explain differences in potential vulnerability to nerve injury, onset time, and minimal efficient anesthetic volume. Density of sodium channels in mammalian myelinated nerve fibers and nature of the axonal membrane underneath the myelin sheath. Voltage-gated sodium channels: biophysics, pharmacology, and associated channelopathies.

Buy malegra dxt 130 mg with mastercardVideo Laryngoscopes As with versatile bronchoscopes, video chip know-how has begun to largely replace fiberoptic know-how in inflexible indirect laryngoscopes because of the advantages of the next high quality picture, elevated sturdiness, and decreased maintenance costs. These units are due to this fact of explicit utility in patients with cervical immobilization, micrognathia, or restricted mouth opening. Lighted stylets could additionally be notably helpful when the presence of blood or heavy secretions limits visualization of the airway. The guide is often a metal guidewire, though an epidural catheter can be utilized. The anterior neck should be cleansed before puncture, and aseptic method should be used. The translaryngeal puncture site could be performed superior or inferior to the cricoid cartilage. At this stage, reconfirmation of a place within the trachea and instillation of an area anesthetic may be performed with a second syringe filled with 2 to 4 mL of 2% or 4% lidocaine. The guidewire is then advanced via the angiocatheter till it exits the mouth or nose. The guidewire is clamped with a hemostat on the degree of the pores and skin of the neck to stop migration. Potential problems embrace bleeding (usually minimal), subcutaneous emphysema, pneumomediastinum, pneumothorax, and damage to the posterior trachea or esophagus. They are designated as left-sided or right-sided, relying on whether the bronchial lumen goes to the left or proper primary bronchus. The blue bronchial cuff ought to be positioned just below the carina in the applicable bronchus. Inflation of the blue bronchial balloon under direct visualization helps confirm proper placement. Bronchial blockers are basically hollow, balloon-tipped catheters which might be endobronchially placed to isolate and deflate one lung. In these situations, the usage of a modified single-lumen tube with an built-in bronchial blocker. Archie Brain in 1997; it became obtainable for industrial use within the United States shortly thereafter. The inflexible handle and airway tube allow a fast and exact management of masks position. An epiglottic elevating bar is designed to elevate the epiglottis because the tube is advanced into the bowl. A disposable, single-use model is available in addition to the unique reusable mannequin. The tubes are straight, wire-reinforced, and have a soft molded tip designed to stop impingement on laryngeal structures. This could additionally be especially useful in the morbidly overweight affected person or sufferers with soiled airways. During the classic technique of retrograde intubation, after a catheter is placed within the inferior cricothyroid membrane, the J-tip of a guidewire is directed upward till it may be retrieved from the mouth or nares. The hemostat that held the guidewire in place internally might now be launched and the guidewire eliminated. These methods may also be used as a primary airway in some tough airway conditions when makes an attempt at securing a noninvasive airway are prone to fail, corresponding to a affected person with a laryngeal neoplasm and critical airway obstruction. Expiration is passive as a result of the elastic recoil of the lungs and the chest wall. Allowing adequate time for passive expiration to avoid barotrauma from breath stacking is crucial. Expiration occurs by way of the glottis and is dependent upon a nonobstructed upper airway, which is imperative to avoid barotrauma and resulting pneumothorax. Confirmation of proper intratracheal placement of the catheter by testing for aspiration of air is crucial earlier than initiating jet ventilation. The pipeline stress for oxygen in hospitals within the United States is approximately 55 psi. Commercially available jet ventilators typically include strain regulators to lower the pipeline stress to present profitable jet ventilation whereas avoiding larger pressures that may result in barotrauma. In most cases within the operating room, sufficient pressure for jet air flow can be achieved by connecting straight to the pipeline provide. To forestall this complication, guaranteeing that a path for air egress exists and that enough time for passive expiration is available is an absolute necessity. The lowest potential strain that can provide enough oxygenation and ventilation must be used. Cricothyrotomy equipment ought to be included in all emergency airway storage units and readily available. Other contraindications to cricothyrotomy embrace laryngeal fractures, laryngeal neoplasm, subglottic stenosis, coagulopathy, and distorted or unidentifiable neck anatomy. The two most common methods for performing a cricothyrotomy are the percutaneous dilational cricothyrotomy and the surgical cricothyrotomy. For the anesthesiologist, the percutaneous approach has traditionally been most popular due to the familiarity of using the Seldinger technique for different procedures. Recently, nonetheless, surgical cricothyrotomy has been advocated as the popular method because of its sooner pace and higher reliability. It is recommended that all anesthesiologists be taught this method and obtain regular training to avoid fading of talent. The foundation for this process is the insertion of an airway catheter over a dilator that has been inserted over a guidewire. Holding the scalpel in your right hand, make a transverse stab incision through the pores and skin and cricothyroid membrane with the cutting edge of the blade going through toward you. Keep the scalpel perpendicular to the skin and turn it through 90� in order that the sharp edge points caudally (toward the feet). Maintain light traction, pulling the scalpel toward you (laterally) with the left hand, maintaining the scalpel handle vertical to the pores and skin (not slanted). Holding the bougie at a proper angle to the trachea, slide the coud� tip of the bougie down the aspect of the scalpel blade furthest from you into the trachea. Difficult Airway Society 2015 pointers for administration of unanticipated troublesome intubation in adults. Complications embrace hemorrhage, harm to the posterior tracheal wall or esophagus, vocal cord harm, laceration of the thyroid gland, and improper insertion of the cannula. Placement of the airway cannula within the subcutaneous tissue can end result in subcutaneous or mediastinal emphysema. Late complications from cricothyrotomy embrace swallowing dysfunction, infection, voice modifications, and tracheal stenosis.

Order malegra dxt with a mastercardSystolic compression of epicardial coronary and intramural arteries in kids with hypertrophic cardiomyopathy. Anesthetic administration for cardioverter-defibrillator implantation in a patient with Kearns-Sayre syndrome. Anesthetic concerns in mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes syndrome: a case collection. Anesthesia-related morbidity and mortality after surgical procedure for muscle biopsy in kids with mitochondrial defects. Ketamine monoanaesthesia for diagnostic muscle biopsy in neuromuscular issues in infancy and childhood: floppy toddler syndrome. Progressive exterior ophthalmoplegia and ambulatory remifentanil-propofol based anaesthesia. Anaesthetic issues for a child with combined PraderWilli syndrome and mitochondrial myopathy. Inborn oxidative phosphorylation defect as risk factor for propofol infusion syndrome. Cardiac preconditioning by unstable anesthetic brokers: a defining function for altered mitochondrial bioenergetics. Minimum alveolar concentration for halothane in children with cerebral palsy and severe psychological retardation. Anaesthetic administration of labour and delivery in the parturient with mitochondrial myopathy. Severe hyponatremia occurring after surgical stress in a patient with mitochondrial disease. Sensitivity to each vecuronium and neostigmine in a sero-negative myasthenic patient. A new approach to anesthesia management in myasthenia gravis: reversal of neuromuscular blockade by sugammadex. Serum and plasma from sufferers with Lambert-Eaton Myasthenic Syndrome scale back depolarization-dependent uptake of 45Ca2+ into rat cortical synaptosomes. Anesthetic administration of familial hypokalemic periodic paralysis throughout parturition. Familial hypokalemic periodic paralysis and Wolff-Parkinson-White syndrome in being pregnant. Sodium channel inactivation defects are related to acetazolamide-exacerbated hypokalemic periodic paralysis. Propofol-remifentanil target-controlled anesthesia in a affected person with hyperkalemic familial periodic paralysis. Epidural anesthesia in a patient with hyperkalemic periodic paralysis present process orthopedic surgical procedure. Combined spinal/general anesthesia with postoperative femoral nerve block for complete knee replacement in a patient with familial hyperkalemic periodic paralysis: a case report. Total intravenous anaesthesia in a patient with familial hypokalaemic periodic paralysis. Anaesthetic administration of a affected person with hypokalemic periodic paralysis- a case report. Mutation evaluation of two patients with hypokalemic periodic paralysis and suspected malignant hyperthermia. An anterolateral precordial lead (V3, V4, or V5) ought to be chosen for essentially the most sensitive detection of myocardial ischemia. Most automated noninvasive arterial blood strain measuring units use an oscillometric measurement technique and rarely cause complications. Despite the absence of anatomic collateral circulate at the elbow, brachial artery catheterization for perioperative blood stress monitoring is a safe alternative to radial or femoral arterial catheterization. The accuracy of a directly recorded arterial strain waveform is decided by the natural frequency and damping coefficient of the pressure monitoring system. Optimal dynamic response of the system might be achieved when the pure frequency is excessive, thereby permitting correct pressure recording across a extensive range of damping coefficients. The extra conventional location for the reference degree used for hemodynamic monitoring including central venous and pulmonary artery pressures, is the mid-thoracic stage, which corresponds most closely to the mid-left atrial place and is positioned halfway between the anterior sternum and the mattress floor in the supine affected person. Because of wave reflection and other physical phenomena, the arterial blood stress recorded from peripheral sites has a wider pulse strain than when measured extra centrally. Right inside jugular vein cannulation is most popular due to its consistent, predictable anatomic location and its relative ease of entry intraoperatively. Mechanical problems from central venous catheters could be decreased by the use of ultrasound vessel localization, venous stress measurement before massive catheter insertion, and radiographic affirmation that the catheter tip lies outside the pericardium and parallel to the walls of the superior vena cava. Catheter misuse and information misinterpretation are among the most typical issues of central venous and pulmonary artery catheters. Pulmonary artery wedge strain is a delayed and damped reflection of left atrial pressure. The wedge strain supplies an in depth estimate for pulmonary capillary stress in plenty of instances, however it might underestimate capillary pressure when postcapillary pulmonary vascular resistance is elevated, as in sufferers with sepsis. Pulmonary artery catheter monitoring has not been shown to improve patient outcomes. Reasons cited for these outcomes embrace misinterpretation of catheter-derived knowledge and failure of hemodynamic therapies that are guided by particular hemodynamic indices. Thermodilution cardiac output monitoring, probably the most extensively used medical method, is topic to measurement errors introduced by fast intravenous fluid administration, intracardiac shunts, and tricuspid valve regurgitation. Mixed venous hemoglobin oxygen saturation is a measure of the adequacy of cardiac output relative to physique oxygen necessities. This measurement is also dependent on the arterial hemoglobin oxygen saturation and hemoglobin concentration. Regardless of the manner used, though, you will want to understand the strengths and limitations of monitoring techniques. Considering both in monitoring and medical analysis improves accuracy and reduces measurement errors and false alarms. Heart Rate and Pulse Rate Monitoring the flexibility to estimate the heart fee quickly with a "finger on the pulse" is as important as this expression is widespread despite near-universal use of digital gadgets for steady monitoring. Pulse deficit describes the extent to which the pulse fee is less than the heart price and should arise in conditions corresponding to atrial fibrillation during which stroke quantity is periodically compromised by a very short R-R interval to such an extent that no arterial pulse is detectable for that systolic ejection. Electricalmechanical dissociation and pulseless electrical activity are extreme examples of pulse deficit by which cardiac contraction is totally unable to generate a palpable peripheral pulse. Typically, two of those 12 normal leads are concurrently displayed on the bedside monitor. Historically, the augmented limb leads and precordial leads were described as unipolar, whereas the usual limb leads have been described as bipolar. In some instances, surgical incisions, patient positioning, or other procedural elements might mandate adjusting these limb lead electrode places. The V5 precordial lead is the one mostly chosen for monitoring patients at risk for myocardial ischemia, since historically it has been shown to be essentially the most sensitive single lead for detecting ischemia throughout train stress testing12,thirteen and through anesthesia. Accurate lead placement is facilitated by finding the manubrial-sternal junction, its immediately inferior rib interspace (the second), and then palpating all the way down to identify the fourth and fifth interspaces for correct precordial lead location. Precise positioning of the lateral precordial leads is ensured by identifying the fifth intercostal house in the mid-clavicular line for lead V4, shifting laterally to the anterior axillary line for V5, and additional laterally to the midaxillary line for V6.

Purchase generic malegra dxt lineWhen the infusion is turned off, the concentrations of every drug decrease, as shown on the z axis. The SmartPilot (Dr�ger, L�beck, Germany) (upper display) is a two-dimensional show that reveals the effect-site concentrations of combined medicine (opioids and intravenous or inhalation hypnotics), based on pharmacokinetic models and the ensuing anesthetic impact and on pharmacodynamic fashions. The orange level signifies the current mixture of effect-site concentrations; the white line reveals the retrospective concentrations; and a 10- and 15-minute prediction is marked by a black level and arrowalready calculated during presetting of delivery. Event markers could also be set to present particular states of the affected person related to the extent of anesthesia. The Medvis show (Medvis, Salt Lake City, Utah) (lower display) exhibits a real-time visualization of anesthetic utilizing pharmacokinetic and pharmacodynamic fashions to predict drug effect-site concentrations and drug results in the past, present time, and 10 minutes into the long run. Drug doses as boluses and infusions are administered through a separate information interface or user interface. Drugs are categorized based on sedation (top plot), analgesia (middle plot), and muscle leisure (bottom plot). Effects are depicted as a population-based probability of unconsciousness (top plot), no response to tracheal intubation (middle plot), and no twitch response to a prepare of four stimulus (bottom plot). Synergistic interactions of sedative-hypnotics and analgesics are shown by the white curves in the plot. For example, the top plot reveals that with only propofol, the probability of unconsciousness is between 50% and 95% (yellow curve), however as a end result of propofol interacts with the opioids, the probability of unconsciousness is larger than 95% (white curve). For example, it takes roughly 12 minutes to awaken from 600 minutes of anesthesia maintained with three g/mL of propofol and 2. On the opposite hand, if the remifentanil focus is increased to 5 ng/mL, then the propofol focus may be decreased to between 2 and a pair of. One might be concerned that such a technique places sufferers at increased risk for awareness as a result of a propofol focus of two g/mL is beneath the C50 value for wakefulness. Infusion units may be categorised as either controllers or constructive displacement pumps. Explicit in their title, controllers comprise mechanisms that control the speed of flow produced by gravity, whereas optimistic displacement pumps contain active pumping mechanisms. The mostly used pumps for administration of intravenous anesthetics are positive displacement syringe pumps that use quite lots of mechanisms. These pumps have acceptable accuracy and have several options that make them significantly suitable for anesthetic supply. An necessary advance has been the introduction of a calculator function inside the pump in order that the clinician can enter the burden of the affected person, the drug focus, and the infusion rate in dose/unit weight/unit time and the pump will then calculate the infusion in volume/unit time. These pumps additionally allow easy software of a staged infusion scheme by permitting an initial dose and a upkeep infusion fee to be programmed into the pump. Further enhancements are drug libraries by class of drug, instructed dosing schemes, and maximal dosing alerts. These modest advances in pump know-how and design allow intravenous anesthetics to be conveniently and safely delivered. When the drug administration set has too massive a deadspace, the precise supply price can be altered, depending on the flow fee of coadministered fluid. After the loading dose, an initially high infusion rate to account for redistribution ought to be used after which titrated to the bottom infusion price that may maintain adequate anesthesia or sedation. When utilizing opiates as a part of a nitrous-narcotic method or for cardiac anesthesia, the dosing scheme listed beneath anesthesia is used. When the opiate is mixed as a part of balanced anesthesia, dosing listed for analgesia is required. Ultimately, the adequate fee of drug administration is predicated on statement and examination. Individual patients differ significantly of their response to a given drug dose or concentration; therefore titrating to an adequate drug stage for every particular person affected person is crucial. Drug concentrations required to present adequate anesthesia also differ in accordance with the type of surgery. Drug focus requirements are sometimes smaller through the finish section of surgery; therefore titration typically involves considered discount of the infusion fee towards the end of surgical procedure to facilitate rapid restoration. If the infusion rate is insufficient to maintain enough anesthesia, then both a further loading (bolus) dose and an increase in infusion are required to increase the plasma (biophase) drug concentration rapidly. Various interventions additionally require bigger drug concentrations, normally for brief intervals. Consequently, the infusion scheme should be tailor-made to provide peak concentrations throughout these transient intervals of intense stimulation. An sufficient drug level for endotracheal intubation is commonly achieved with the initial loading dose; nevertheless, for procedures such as pores and skin incision, an extra bolus dose could also be necessary. At start-up the person is required to enter the weight of the patient and the drug focus. Thereafter, the pumps are in a place to accept as input mass-based rates, from which they calculate and implement volume infusion charges. The aim of computer-controlled closed-loop techniques is to formalize this means of observation and intervention to provide fine-tuned and more correct control. Such systems use a close to continuous signal of drug impact, calculate the error between the observed value and the set level value (selected by the user), and use this error figure in an algorithm to make frequent and common changes to drug administration charges. Some computer-controlled drug delivery systems try to predict the longer term drug impact to make applicable adjustments properly upfront. A computer or microprocessor is required to perform the complex calculations and to management the infusion pump. Briefly, the infusion begins with an preliminary bolus of drug required to achieve the preliminary target focus. Since the elimination fee fixed is fixed, the amount of drug eliminated in every unit of time is proportional to the plasma focus; accordingly, at steady-state plasma concentrations, drug elimination by elimination could be compensated for by a relentless rate infusion. Third, a second infusion is run to exchange drug distributed or transferred to peripheral tissues. The amount redistributed exponentially declines over time as the gradient between the central compartment and the peripheral compartment decreases. Replacing distributed drug requires an infusion at an exponentially declining fee to exchange drug lost from the central compartment by distribution until regular state. Using the dose-response relationship, drug titration ought to be performed as close as potential to the drug effect. Titrating to a particular effect or, if not attainable, a particular effect-site focus provides benefits. Pharmacokinetic elements similar to distribution, metabolism, and/or excretion decide the relationship between drug dose and drug concentration in the biophase. In the biophase, the drug interacts with the receptor, and the pharmacologic impact is accomplished via effectuation processes. Computer-controlled, closedloop suggestions measures the error between the effect and the goal impact to control the dose administration (blue).
Order malegra dxt 130mg amexDuchenne and Becker muscular dystrophies are X-linked recessive disorders that occur primarily in males. Affected people have elevated creatine phosphokinase levels, often preceding the onset of signs. Female carriers of the irregular gene may have dilated cardiomyopathy regardless of having no other manifestations of the disease. Facioscapulohumeral muscular dystrophy (also generally identified as faciohumeroscapular or Landouzy-Dejerine muscular dystrophy) is an autosomal dominant disorder 31 � Preoperative Evaluation 973 that affects both sexes and causes a sluggish, progressive weak point of muscle tissue in the shoulders and face. Cardiomyopathy happens a lot much less regularly than in other dystrophies, however arrhythmias have been reported. Limb-girdle dystrophies have a variable genetic inheritance sample and primarily have an result on the muscular tissues of the shoulders and pelvis. Conduction abnormalities are present in some sufferers, although frank cardiomyopathies are less frequent. The preoperative evaluation is essentially similar to that described previously for Duchenne muscular dystrophy. Myotonia is characterised by extended contraction and delayed relaxation of muscular tissues. It is a standard symptom of several dystrophies, together with classic myotonic dystrophy, congenital myotonic dystrophy, myotonia congenital, and central core disease. Myotonic dystrophy, which is the most typical of those conditions, is an autosomal dominant inherited dysfunction affecting both sexes. Congenital myotonic dystrophy is a extreme form of this illness that manifests in infancy, usually within the children of affected mothers. The classic findings are severe muscle losing, typically involving the diaphragm, face, palms, pharynx, and larynx. The illness severity is variable, with symptoms typically not apparent till the second or third decade of life; hence, a family history is essential. Cardiomyopathies, arrhythmias, and conduction abnormalities are frequent, while some patients also have cardiac valvular abnormalities. Cardiac involvement might not correlate with the diploma of atrophy or weak spot in skeletal muscle. Affected individuals are additionally at risk for aspiration, pneumonia, respiratory failure, and postoperative pulmonary problems. Central core disease is a uncommon dysfunction brought on by deficiency of mitochondrial enzymes. The name derives from findings of muscle biopsies, which reveal "cores" of abnormalities. Affected individuals have proximal muscle weakness, scoliosis, and sometimes cardiomyopathies. As with myotonic dystrophy, patients are in danger for respiratory failure and aspiration. The preoperative evaluation focuses on the cardiopulmonary system, with particular emphasis on evaluating for pulmonary infection, heart failure, syncope, conduction abnormalities, and valvular abnormalities. Central Nervous System Tumors Pituitary tumors are categorised as functioning (associated with endocrine abnormalities) versus nonfunctioning, in addition to benign (adenomas are the most typical pituitary lesion) versus malignant. The tumor can have mass effects that result in related signs, similar to headaches, visual subject defects, and increased intracranial pressure (with resulting gait disturbances, vomiting, cranial nerve deficits, bladder incontinence, bowel incontinence). These hormones are all produced by the anterior lobe of the pituitary and are managed by a suggestions loop from the hypothalamus. The posterior pituitary shops and secretes vasopressin and oxytocin, that are synthesized in the hypothalamus. Acromegaly results in enlargement of connective tissue, bone, and visceral organs. Affected individuals have increased dangers of sleep apnea (both central and obstructive), neuropathies (from nerve entrapment), hypertension, diastolic dysfunction, and cardiac valvular abnormalities. The preoperative evaluation ought to doc any chest ache, dyspnea, snoring, numbness, polydipsia, headaches, and visual disturbances. The physical examination focuses on blood pressure, airway examination, murmurs, neurologic findings, and peripheral edema. It is important to plan for possible tough airway administration and inform the affected person concerning the potential use of awake fiberoptic intubation. Prolactin- and gonadotropin-secreting tumors have little impact on anesthetic administration, but their symptoms may alert clinicians to an undiagnosed pituitary tumor. A deficiency ends in diabetes insipidus, which is characterised by extreme urine output from a failure to reabsorb water. Patients with pituitary tumors, pituitary apoplexy (hemorrhage into pituitary, which is associated with hypertension, trauma, or pregnancy), or earlier pituitary tumor resection might require hormone replacement therapy. The adequacy of replacement remedy may be decided primarily based on the clinical analysis, in addition to blood sampling for electrolyte concentrations, creatinine concentrations, and thyroid operate exams. Other intracranial tumors embrace gliomas (45% of tumors), astrocytomas, ependymomas, medulloblastomas, oligodendrocytomas (malignant and highly lethal), benign meningiomas (15% of tumors), schwannomas, craniopharyngiomas, and dermoid tumors. Metastatic lesions (6% of intracranial tumors) can even happen with nearly all kinds of main malignant ailments. Common sources of metastatic intracranial lesions include breast, colorectal, and lung cancers. Most intracranial tumors are detected both incidentally, or when sufferers develop seizures or signs related to mass impact. Symptoms of mass effect include headaches, strokelike signs, vomiting, visible disturbances, altered cognitive operate, and ataxia. For patients with metastatic lesions, issues pertaining to the first malignant disease and previous remedy. Continuation of preexisting corticosteroids (to deal with cerebral edema) and anticonvulsant medications is important. Assessment of deformities is necessary due to their potential implications for airway management and regional anesthesia approach. Affected organ techniques may include cardiovascular, pulmonary, renal, hematologic, integumentary, gastrointestinal, central nervous, and peripheral nervous methods. Rheumatoid Arthritis Rheumatoid arthritis is a chronic autoimmune disorder that primarily affects joints, nevertheless it usually additionally affects multiple organ methods. The illness impacts roughly 1% of the inhabitants, and ladies are 2 to three times extra prone to be affected as are men. Joint involvement is characterized by inflammation that may progress to severe deformity, although the disease course can differ dramatically. The temporomandibular joints and cricoarytenoid cartilage can be concerned, leading to limited mouth opening, hoarseness, and attainable difficulties with airway administration. Subluxation, which is caused by ligamentous laxity, versus joint illness, may also happen, though the prevalence appears to be reducing with the advent of improved disease modifying brokers. Symptoms of myocardial ischemia may be masked in sufferers with rheumatoid arthritis due to impairment of practical standing by concomitant joint illness. In addition, exertional dyspnea because of coronary heart failure could additionally be confused with pulmonary involvement.
Purchase malegra dxt visaThis enhance is associated with an antidepressant impact, an antihypertensive effect, an antinarcoleptic impact, elevation of liver enzymes, and delayed onset of Parkinson disease. The most serious effects of this interplay are convulsions and hyperpyrexic coma (particularly after narcotics). A regional block may be attempted as therapy of postoperative ache to avoid having to give narcotics. Alternative medication for the treatment of extreme despair embody the tricyclic antidepressant medication: amitriptyline, imipramine, desipramine, doxepin, nortriptyline, trazodone, and others. Given on a long-term basis, these medication lower stores of noradrenergic catecholamines. Although arrhythmias induced by tricyclic antidepressants have been treated successfully with physostigmine, bradycardia has sometimes occurred. The selective serotonin reuptake inhibitors have gained reputation and embrace citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline, though these can also have serious unwanted aspect effects. Discontinuing medicine could cause withdrawal signs or precipitate recurrence of psychiatric illness. In addition, these drugs possess various levels of parasympathetic stimulation and skill to block -adrenergic receptors. The phenothiazines embrace chlorpromazine, promazine, triflupromazine, fluphenazine, trifluoperazine, prochlorperazine, and many others. Both the phenothiazines and butyrophenones produce sedation, melancholy, and antihistaminic, antiemetic, and hypothermic responses. They are additionally associated with cholestatic jaundice, impotence, dystonia, and photosensitivity. In excitable cells, lithium mimics sodium and decreases the discharge of neurotransmitters each centrally and peripherally. Lithium prolongs neuromuscular blockade and will decrease anesthetic necessities as a outcome of it blocks brainstem launch of norepinephrine, epinephrine, and dopamine. Psychoactive medicine such because the amphetamines (including methamphetamines, and crystal methamphetamine) and cocaine acutely release norepinephrine, epinephrine, and dopamine and block their reuptake. Taken on a long-term foundation, they deplete nerve endings of those neurotransmitters. Drugs that appear to improve central -adrenergic release increase anesthetic requirements, whereas medicine that seem to decrease central -adrenergic launch decrease anesthetic requirements. The pharmacologic traits of the varied antiarrhythmic medication can affect anesthetic management. Disopyramide is similar to quinidine and procainamide in its antiarrhythmic effectiveness. Disopyramide is excreted primarily by the kidneys, however hepatic disease increases its half-life. This drug often produces anticholinergic results, including tachycardia, urinary retention, and psychosis. Reports have confirmed this enhancement for quinidine, phenytoin, lidocaine, procainamide, and propranolol. Amiodarone, an antiadrenergic drug used to deal with recurrent supraventricular and ventricular tachycardia, causes thyroid dysfunction on account of the big amount of iodine in its structure, in addition to peripheral neuropathy, and has been associated with hypertension, bradyarrhythmias, and lowered cardiac output throughout anesthesia. Appropriate antibiotic prophylaxis for surgery requires a knowledge of the likelihood of an infection for that type of surgical process and, if the incidence of infection warrants, using a drug regimen directed towards the most likely infecting organisms. These drugs inhibit serum cholinesterase, which is answerable for the hydrolysis and inactivation of succinylcholine and estertype local anesthetics similar to procaine, chloroprocaine, and tetracaine. High-dose insulin remedy attenuates systemic inflammation response in coronary artery bypass grafting patients. Effect of an intensive glucose administration protocol on the mortality of critically ill grownup patients. Intensive broad glucose control and vascular outcomes in sufferers with sort 2 diabetes. Strict blood glucose control with insulin after cardiac surgery: impact on 4-year survival, depending on medical care, and high quality of life. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically sick sufferers. Preoperative autonomic operate abnormalities in patients with diabetes mellitus and patients with hypertension. Haemoglobin A1c (HbA1C) in non-diabetic and diabetic vascular patients: is HbA1C an impartial danger issue and predictor of antagonistic outcome Elevated preoperative hemoglobin A1c level is associated with lowered long-term survival after coronary artery bypass surgical procedure. Haemoglobin A1c as a predictor of postoperative hyperglycaemia and complications after major colorectal surgical procedure. Intensive intraoperative insulin therapy versus typical glucose administration throughout cardiac surgery: a randomized trial. Effect of intensive remedy on residual beta-cell operate in sufferers with kind 1 diabetes in the diabetes management and problems trial: a randomized, managed trial. Perioperative maternal and neonatal acid-base status and glucose metabolism in sufferers with insulin-dependent diabetes mellitus. Risk adjustment of the postoperative mortality price for the comparative assessment of the quality of surgical care: results of the National Veterans Affairs Surgical Risk Study. Prevention of kind 2 diabetes mellitus by adjustments in life-style amongst subjects with impaired glucose tolerance. Society for Ambulatory Anesthesia consensus statement on perioperative blood glucose administration in diabetic patients present process ambulatory surgery. Use of enalapril to attenuate decline in renal operate in normotensive, normoalbuminuric sufferers with kind 2 diabetes mellitus: a randomized, managed trial. Corrigendum: evaluation of proof for adult diabetic ketoacidosis management protocols. Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Management of hyperglycemic crises: diabetic ketoacidosis and hyperglycemic hyperosmolar state. Hypoglycemia in sufferers present process cerebral aneurysm surgical procedure: its affiliation with long-term gross neurologic and neuropsychological perform. National Lipid Association suggestions for patient-centered management of dyslipidemia: part 1 - executive abstract. A two institution experience with 226 endoscopically positioned jejunal feeding tubes in critically ill surgical sufferers. Enteral versus parenteral vitamin in critically sick patients: an up to date systematic review and meta-analysis of randomized controlled trials. Physiological cortisol substitution of long-term steroid-treated patients undergoing main surgery. Supplemental perioperative steroids for surgical sufferers with adrenal insufficiency.
References - Severi G, Morris HA, MacInnis RJ, et al: Circulating steroid hormones and the risk of prostate cancer, Cancer Epidemiol Biomarkers Prev 15:86n91, 2006.
- Muntener M, Nielson ME, Romero FR, et al: Long-term oncologic outcome after laparoscopic radical nephroureteretomy for upper tract transitional cell carcinoma, Eur Urol 51(6):1639n1644, 2007. Muntener M, Schaeffer EM, Romero FR, et al: Incidence of local recurrence and port site metastasis after laparoscopic radical nephroureterectomy, Urology 70(5):864n868, 2007. Murphy DM, Zincke H, Furlow WL: Management of high grade transitional cell cancer of the upper urinary tract, J Urol 125:25n29, 1981.
- Park S, McAninch JW: Straddle injuries to the bulbar urethra: management and outcomes in 78 patients, J Urol 171(Pt 1):722n725, 2004.
- Simmons JL, Bunce PL: On the use of an antihistamine in the treatment of interstitial cystitis, Am Surg 24(9):664n667, 1958.
|
|


